Article Text

Abstract
Objectives To determine if a topically applied non-steroidal anti-inflammatory drug (diclofenac) can provide short-term pain relief for chronic Achilles tendinopathy (CAT), in order to inform the development of a new rehabilitation protocol.
Design and setting Pilot double-blind, cross-over randomised controlled trial providing participants with tertiary care. The study was conducted at a single research centre in Vancouver, BC.
Participants Sixteen adults with unilateral CAT and three adults with bilateral CAT participated.
Interventions Participants received two successive treatments (10% diclofenac gel or placebo gel) in random order over a 3-day period. There was a 1-week washout period between the treatments. Allocation was by simple randomisation, and the participants as well as the assessing/treating researcher were blinded to treatment allocation.
Outcome measures The primary outcome measure was pain level (0–10) during tendon loading (hopping). Secondary outcome measures included pain at rest, pressure pain threshold of the Achilles tendon and symptom improvement.
Results Nineteen adults participated in the study, and all were included in the analysis. Diclofenac gel significantly reduced the average pain during tendon loading (p<0.001) and at rest (p=0.031). The average baseline hopping pain was 4.8/10 (95% CI 3.92 to 5.68) and was reduced to 3.1/10 (2.35–3.85) by diclofenac. Pain at rest was decreased and pressure pain threshold increased with diclofenac treatment, but not with placebo gel. There were no observed or reported side effects of either treatment.
Conclusions In this small, short-term study, diclofenac was able to improve symptoms and reduce pain during tendon loading in participants with CAT, whereas placebo gel was not. A future study of diclofenac as a supplement to rehabilitation, with longer follow-up and powered to detect a difference between diclofenac and placebo, is indicated.
Trial registration ISRCTN60151284, http://www.isrctn.com/ISRCTN60151284
Ethics UBC Clinical Research Ethics Board approval was obtained for this research. The certificate number of the ethics certificate of approval to conduct research is H15-00999.
- Chronic pain
- Achilles tendon
- Tendinopathy
- Diclofenac
- Achilles tendinopathy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study presents preliminary evidence that topical diclofenac exerts an analgesic effect on chronic Achilles tendon pain.
This was a well-controlled, double-blinded experiment conducted in a research setting with no dropouts and all data analysed.
Given that full recovery from chronic Achilles tendinopathy requires many months and that the gold standard of treatment involves exercise-based rehabilitation, it is not, by itself, sufficient evidence to change practice.
The study was not adequately powered to detect significant differences between placebo and diclofenac and is of insufficient length to determine impact on clinical outcomes.
Introduction
Chronic Achilles tendinopathy (CAT) is characterised by a breakdown and disorganisation of collagen fibres, increased tendon blood flow, an increase in the amount of non-collagenous matrix and resultant chronic pain and swelling.1 The condition is often attributed to a failure in the tendon’s adaptive and reparative responses following repetitive tendon loading, and the pathogenesis may involve a chronic low-grade inflammation in the tendon and surrounding tissues.2 3 Training at excessive or unaccustomed volumes can lead to a degradation of the viscoelastic characteristics of the tendon and an accumulation of dysfunctional repair tissue.4 CAT is common in athletes that participate in sports involving running and jumping, but the condition also occurs in sedentary, middle-aged adults.5 6 The causes and pathogenesis of CAT are likely to be diverse and multifactorial in many cases: extrinsic factors (such as training errors) have been suggested to interact with intrinsic factors (such as advancing age, male sex, increasing body composition, genetic predisposition and insufficient muscle strength or flexibility) to predispose to the chronic condition.3 7
One of the long-term goals of rehabilitation is to strengthen the injured Achilles tendon enough to withstand the same force as a healthy tendon. Various forms of exercise including eccentric training, heavy slow resistance and a combination of eccentric/concentric exercise have been reported to promote the recovery of Achilles tendons to healthy states.8 However, chronic pain may be a limitation in CAT rehabilitation. It has been suggested that allowing the patient to experience pain during rehabilitation of CAT appears to have no negative effect on overall recovery9 10 and that, in fact, some pain may be unavoidable to ensure that the Achilles tendon load is sufficient to create meaningful adaptive changes in the tendon.11 Nevertheless, in the current study we investigated the effects of topical diclofenac on patients with CAT in order to determine if participants could achieve a physiological tendon load (ie, hopping in place) with less pain, based on the clinical observation that pain may be a limiting factor during rehabilitation, particularly in the early stages of recovery.
Diclofenac is a non-steroidal anti-inflammatory drug (NSAID) that works by preventing cyclooxygenase from synthesising prostaglandins.12 Topical diclofenac has been shown to be a safe and effective medicine in treating several painful musculoskeletal disorders.13 Topical diclofenac is used in osteoarthritis of the knee to reduce pain, morning stiffness and improved physical function. At high tissue concentration, diclofenac can block sodium channels and prevent nociceptive afferent action potentials.13 Thus, in addition to reducing the levels of classic inflammatory substances like prostaglandins E2, diclofenac could inhibit other relevant nociceptive mechanisms.14
CAT is prevalent in the general population, yet no programme has been developed that can successfully treat this disorder in all cases, and there are no controlled trials to our knowledge of treatments that can successfully reduce pain in the short term, although case studies have demonstrated the efficacy of individualised biomechanical interventions such as taping.15 In order to make progress towards the long-term goal of developing more effective rehabilitation programmes, we investigated the effects of topical diclofenac on individuals with CAT. In addition, this study investigated how pain may influence exercise performance (eg, force output during single-leg hopping at voluntary intensity) in individuals with CAT. The objective of this study was to evaluate the potential utility of incorporating diclofenac into a larger controlled study with a longer treatment course including exercise-oriented rehabilitation.
Methods
Study design and recruitment
This study was a short-term, pilot cross-over randomised controlled trial conducted in a research setting. Recruitment occurred for a predetermined period from August 2015 to March 2016 and was stopped due to the timeline of an investigator’s (EB) academic programme. Participants were recruited by placing advertisements in the community. Each participant received one of the two treatments (placebo or diclofenac) in random order, then after a 1-week wash out period, the participant received the other treatment. The purpose of the placebo group was to assess the magnitude of non-specific effects related to the application of gel and interaction with the study team and to blind the assessor (EB). Following the registration of the trial but before enrolling any patients, additional secondary outcome measures were added (pain at rest and change in symptoms are described below). Participants volunteered and were free to withdraw at any time during the study. No compensation was provided for participation in this study.
Experimental procedure
The following procedures were conducted at the University of British Columbia Hip Health and Mobility (figure 1).

Experimental procedures. The step-by-step outline of study visits (1–4) over 30 days. BMI, body mass index
Visit 1
The coinvestigator (EB) met with the participant at their intake appointment time to review inclusion/exclusion criteria (Box 1), assess interest in study participation and answer questions. If the participant agreed, the consent form was completed. In order to characterise the level of function of enrolled participants, they completed the Tegner Activity Level16 and the VISA-A Questionnaire17 (a self-report questionnaire that measures Achilles tendinopathy severity). The screening visit was completed by having the participant rate their pain (using a numeric pain rating scale (NPRS) from 0 to 10) during 25–28 single-legged hops at a self-selected pace on each leg18 19 on a force plate (Leonardo Mechanograph, Novotec Medical, Pforzheim, Germany). On conclusion of the initial visit and verification of eligibility criteria (Box 1), the following visits were scheduled. The second visit was scheduled after a 1-week washout period. Participants were instructed to refrain from moderate to vigorous physical activity for 72 hours prior to the appointment, to refrain from taking any NSAIDs for 1 week or other analgesics for 24 hours, to receive no new treatment throughout the study and not to make any changes to treatment they might already be receiving.
Inclusion and exclusion criteria
Inclusion criteria
Male and female participants aged 19 years and older
Fluent in English
Participants previously diagnosed with Achilles tendinopathy by a healthcare professional and demonstrating the following criteria: localised Achilles tendon pain and thickening, worsened with palpation and tendon loading activities and no clinical suspicion of other diagnoses
Symptoms for 3 months or more
Participants who are able to give informed consent
VISA-A score less than 80
Pain score (numeric pain rating scale) greater than 2/10 when performing a hopping test (25–28 single-leg hops on the painful side)
Exclusion criteria
Male and female participants aged 18 years and younger
Participants with a BMI greater than 30.0
Participants with previous Achilles tendon rupture
Participants diagnosed with chronic pain syndrome, diabetes, hyperproteinaemia, metabolic syndrome or systemic inflammatory diseases
Participants with symptomatic osteoarthritis of the spine or lower extremities
Participants who have received corticosteroid injections
Participants who take non-steroidal anti-inflammatory medication regularly
Participants who have been prescribed statins, anticoagulants or fluoroquinolones within the past 3 months.
Participants with known allergies to diclofenac or placebo cream.
Participants who are unable to give informed consent.
BMI, body mass index.
Visit 2
The coinvestigator completed the eligibility screen, which included data collection (demographic information, rehabilitation history and medical questionnaire including date of last NSAID taken) and a grey-scale ultrasound scan (10 MHz Terason probe, UTC Technologies scanner, GD Stein, Netherlands) to assess the presence of tendinopathic change (scans performed by EB and read by AS). Following the ultrasound scan, the investigator (EB) used the AlgoMed Algometer (Medoc, Ramat Yishai, Israel) to assess the participant’s pressure pain threshold (PPT) on the affected Achilles tendon(s). Testing was conducted at a controlled rate (30 kPa/s) with the participant lying prone on a treatment plinth. Pressure was gradually applied until the participant first experienced onset of pain, at which point they pushed a button to record the PPT. In cases where the person with CAT had baseline (resting) pain, they were instructed to press the button at the first increase in pain.
Following the PPT measurement, participants were asked to rhythmically hop 25–28 times, at a comfortable pace and intensity (approximately two jumps per second), on one leg, first on the unaffected side, and then on the affected side (15 s rest between each leg). At the end of the hopping, the participant’s pain level was recorded using an NPRS (0–10). Prior to the hopping test, participants warmed up with 5 min of very light stationary biking (no resistance and self-selected pace) and three sets of 10 two-legged toe raises (60 s rest between sets).
Participants were then issued with either placebo gel or 10% diclofenac gel (Medisca, PLO Mediflo 30, an opaque gel base with an off-white hue), which were identical in appearance. A pharmacist uninvolved in the study supplied the gel in semiopaque syringes, and the investigator (EB) and participants did not know the content of the tubes supplied. Participants were instructed to massage 1 g of the gel on the most painful area of the tendon for 30–45 s three times a day at 8-hour intervals for 3 days before the next scheduled appointment. They were asked to complete a medication administration diary to confirm their compliance with the pretest regimen.
Visit 3
At the start of the third visit, participants were asked which treatment they thought they received, any remaining gel was collected from the participant, any suspected side effects were documented and they were asked whether their condition had worsened, improved or stayed the same. They then repeated the following procedures from visit 2: PPT, warm-up and hopping test. At the conclusion of this visit, participants were issued with their second tube of gel (placebo or diclofenac). They were instructed to wait for 1 week before using the remaining gel.
Visit 4
Their fourth appointment was scheduled within 10 days to 2 weeks following the second appointment, where they were required to repeat the same assessments.
Randomisation and blinding
A randomisation list with 32 non-blocked, unstratified allocations was created by a researcher (AS) using a simple random number generator. The same researcher labelled the identical-appearing gels (A or B) before giving them to the researcher (EB) conducting the study. The researcher (AS) who created the allocation list was not involved in any other study procedure and did not interact with participants. The researcher (EB) who conducted the study was not aware of the allocations until after the statistical analysis was complete.
Outcomes
The primary outcome measure was pain during tendon loading (single-leg hopping and numeric scale from 0 to 10). The secondary outcomes were (A) change in overall symptoms, indicated by asking patients if symptoms had improved, worsened or stayed the same, (B) current pain at rest (from 0 to 10) and (C) PPT of the Achilles tendon. When examining the results of the secondary outcome ‘change in symptoms’, we noted a binary distribution (only one tendon worsened, whereas the rest either stayed the same or improved); therefore, this measure was collapsed into a binary outcome of ‘improved’ or ‘worsened/stayed the same’.
Sample size
For this pilot study, we actively recruited over an 18-month period. Sixteen adults with unilateral CAT and three adults with bilateral CAT participated. All available subjects during this period that met all the eligibility criteria were included in this study.
Statistics
Means (SD) are reported in the text to describe continuous variables including age, height, weight, body mass index (BMI), VISA-A scores, symptom duration, resting pain and hopping pain. All calculated values are given to two significant figures. Frequency data were reported for categorical variables including sex, previous treatments and type of Achilles tendinopathy. All data were present and included, as there were no extreme outliers, and the data met all the assumptions for the statistical tests used. The primary analysis was prespecified and consisted of a repeat-measures linear mixed model to examine whether there was a statistically significant effect of type of gel on the outcomes, and the figures display the means and SEs generated by the model. The model also generated a series of uncorrected comparisons using the t-statistic (each with p<0.05) as a post hoc analysis. The following non-prespecified analyses were also conducted: a McNemar’s test to compare paired proportions was used to compare the frequency of those experiencing a change in Achilles tendinopathy symptoms after different treatments (improved vs worsen/stayed the same), and the OR was also calculated as an ancillary in accordance with the Consort statement. Spearman’s correlation was used to examine the association between pain and force for all of the conducted hopping tests. An exploratory sensitivity analysis was conducted to see if the bilateral cases had any effect on the overall results (ie, the linear mixed models were rerun but leaving out the cases with bilateral tendinopathy; n=16). The sensitivity analysis showed that there was no change in significance for the major findings within the study. Pain during the hopping test with the use of diclofenac versus baseline (n=22, p=0.0003; n=16, p=0.0006) and pain at rest with the use of diclofenac versus baseline (n=22, p=0.0313; n=16, p=0.0359) remained significant when participants with bilateral tendinopathy were removed for the analysis. Finally, on examination of the data, we suspected the existence of a learning effect in the Achilles PPT measurement; therefore, we reran the linear mixed model to see if the visit (2, 3 or 4) exerted a main effect on this outcome.
Results
Participants
The participant demographics are shown in table 1. A total of 26 participants were screened at visit 1 for eligibility. After the first visit, seven of the participants did not qualify for the study because they did not fit the inclusion/exclusion criteria (table 1). A total of 19 participants were enrolled. Primary reasons for excluding participants after the first visit were that their pain rating during hopping was 2 or below, their BMI was over 30, they were not diagnosed with Achilles tendinopathy or they were currently receiving statins. With regard to numbers analysed, three of the 19 participants who had bilateral CAT, and the pain levels and symptoms in both of their Achilles were examined separately (total of 22 Achilles), yielding n=22 for all analyses. No patient was excluded after randomisation.
Participant demographics and clinical characteristics
Allocation and blinding
Twelve participants (15 tendons) received diclofenac at visit 2 and placebo at visit 3; the remaining seven participants (seven tendons) received placebo at visit 2 and diclofenac at visit 3. Before the assessment at each visit, participants were asked if they thought the gel they received was placebo or diclofenac. Of the 19 participants, 11 correctly (four incorrectly and four unsure) identified the diclofenac gel, and 12 correctly (three incorrectly and four unsure) identified the placebo gel.
Adherence, dropouts and side effects
There were no dropouts and no drug side effects reported in this study. All 19 participants completed the study, and all data for primary and secondary outcomes were used from all participants, with no missing data. Seventy-nine per cent (15 out of 19) of all participants successfully brought back their diary that recorded gel application. Twenty-one per cent (4 out of 19) stated that they filled out the form properly but forgot it at home or lost it.
Effect of diclofenac and placebo on Achilles tendinopathy hopping pain
Figure 2 and table 2 show the rating of pain (NPRS) during the hopping test. At baseline the average hopping pain was 4.3 (95% CI 3.42 to 5.18). With the use of diclofenac, the average hopping pain declined to 3.1 (95% CI 2.35 to 3.85), and with the use of placebo the average pain was 3.8 (95% CI 2.63 to 4.97). Despite the overlapping CIs in the group means, the linear mixed model (which accounted for the repeated measures design) revealed that diclofenac resulted in a statistically significant decrease in mean hopping pain when compared to baseline (p<0.001). There was no statistically significant difference in hopping pain between the placebo and diclofenac treatment, or between placebo and baseline.
Achilles pain ratings

Pain at rest and during the hopping test. Mean pain rating for the three conditions is shown; error bars represent the SE of the estimate. *, Significant difference in resting pain between the diclofenac and baseline, p=0.031. ø, Significant difference in pain between the diclofenac and baseline during the hopping test, p= 0.003. There was no significant difference in pain between the placebo and baseline or between diclofenac and placebo at rest or during the hopping test. NPRS, numeric pain rating scale.
Effect of diclofenac on Achilles tendinopathy symptoms and resting pain
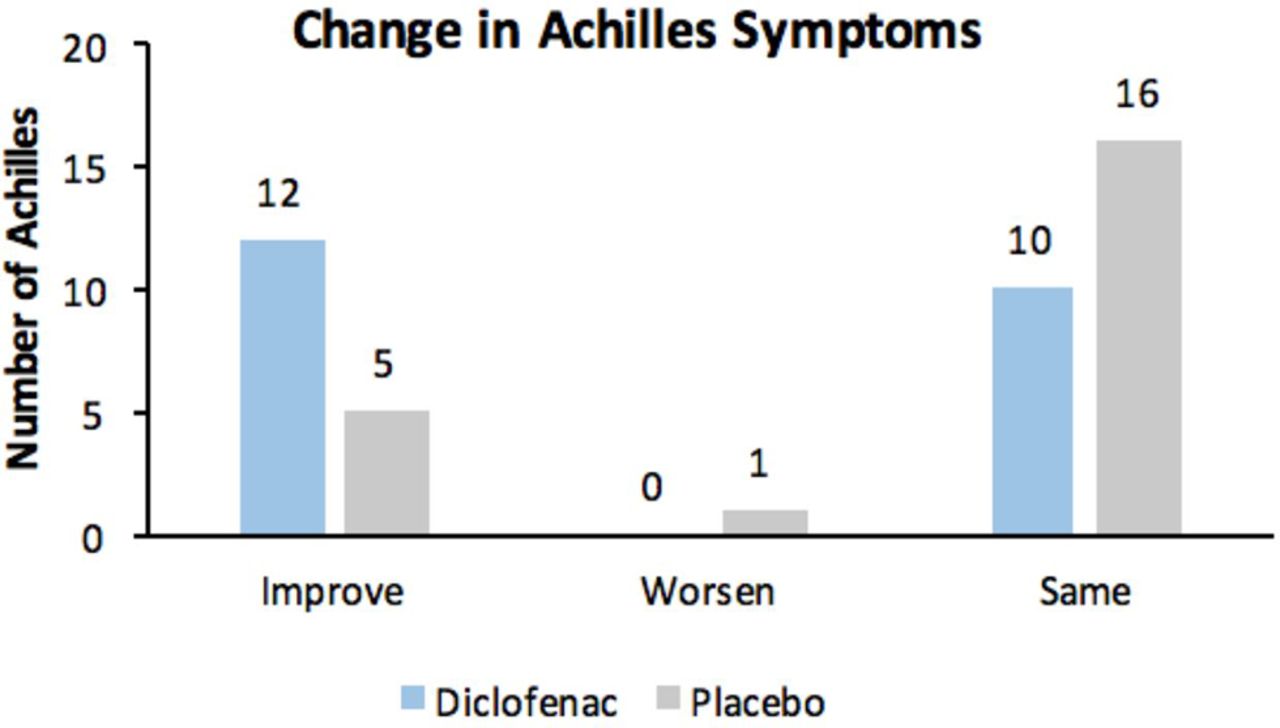
Figure 3 shows the participants’ responses to the question about whether their Achilles tendinopathy symptoms improved, worsened or stayed the same over the 3-day period of gel application. There was a significant (two-tailed McNemar’s test, p=0.045) trend favouring improvement with diclofenac treatment, with 55% of subjects reporting improvements in symptoms compared with 23% following placebo. The OR of improved symptoms with diclofenac versus placebo was 8.0 (95% CI 1.1 to 350, p=0.041).
Figure 2 and table 2 show the rating of pain during rest on the NPRS. At baseline, the average resting pain was 3.1 (95% CI 2.51 to 3.69), with the use of diclofenac the average pain was 2.3 (95% CI 1.67 to 2.93) and with the use of placebo the average pain was 2.7 (95% CI 1.86 to 3.54). The change in resting pain from baseline to application of diclofenac was statistically significant (p=0.031). There was no statistically significant difference in resting pain between the placebo and diclofenac treatment or between placebo and baseline.

{kind=link}
{kind=link}
{kind=link}
Achilles tendinopathy symptoms. Nineteen participants (22 Achilles) were asked if their Achilles symptoms improved, worsened or stayed the same over the 3-day course of their treatment (two-tailed McNemar’s test, p = 0.045).
Relation between pain and force during hopping
We conducted an ancillary analysis of the relationship between the amount of force exerted during hopping and the amount of pain felt (NPRS). As the amount of pain decreased, the amount of force exerted during hopping increased (rs=−0.41, p<0.001).
Effect of diclofenac and placebo on PPT in the affected Achilles
Table 2 outlines the effects of the placebo and diclofenac on the affected Achilles tendons. There was a statistically significant difference in Achilles PPT between the application of diclofenac and baseline, but not with application of placebo gel. This difference occurred despite the fact that the mean Achilles PPT with placebo gel was higher, perhaps due to a slightly larger number of individuals receiving the placebo gel as the second treatment (12 vs 7 participants), in combination with an apparent learning effect (ancillary analysis revealed that PPT values rose over the course of the study from visit 2 to visit 4 from 220 to 310, p=0.028).
Discussion
The purpose of this study was to determine if diclofenac could provide pain relief for individuals with CAT and to determine if a larger, adequately powered clinical study of this treatment incorporating a longer treatment course of rehabilitation would be indicated. The data presented here demonstrate that the majority of participants reported that their condition improved with the use of diclofenac. Resting pain and the PPT of the Achilles were also significantly improved with diclofenac, but not placebo. This pilot study therefore provides some preliminary evidence that diclofenac could be a beneficial option for partial symptom relief, and a larger study powered to detect differences between diclofenac and placebo is warranted.
The force–pain relationship in this study, although generated via an exploratory/ancillary analysis and only demonstrating a moderate correlation, showed that when a participant was feeling less pain, they generated more force during hopping. Participants were free to hop at a self-selected pace and intensity. This finding is consistent with the existing neurophysiological literature. Acute muscle pain of a prime mover has shown to reduce voluntary force and velocity performance in muscles.20 21 However, although the pain was reduced with the use of diclofenac, there was no significant change in jumping force over the three visits. It is possible that longer term use of diclofenac in combination with physical rehabilitation could allow participants to exert more force and thereby achieve a faster recovery, but this hypothesis is very speculative, especially given concerns that the use of NSAIDs may interfere with exercise adaptation.22–25
This study has a number of limitations. Although PPT of the Achilles tendon significantly increased with diclofenac treatment, we also found that the PPT of the Achilles tendon tended to increase over the course of each visit, regardless of treatment allocation. This could be due to a learning effect, that is, participants gaining comfort with the test. Future studies should incorporate a longer period of baseline measurement to ensure that the PPT values are stable prior to initiating an intervention. One of the biggest limitations when researching new treatments for CAT stems from the nature of CAT, which is characterised by fluctuating pain and a slow time to recovery.26 In addition to a longer period of baseline measurement, future studies could ask participants to record all the activities they participate in over the course of the study or, alternately, ask them to wear an activity monitor. This would make participants more accountable for their activities and researchers could take their activity level into consideration when analysing results.
Although this sample size was sufficient to demonstrate a statistically significant improvement with diclofenac treatment compared with baseline, a larger sample size is needed to examine the effectiveness of diclofenac across a more representative sample population, to reduce the possibility of type I and II errors and to specifically examine the potential effects of diclofenac over and above those achieved with placebo. For such a study, one could consider recruiting through rehabilitation centres and making patient-rated change in symptoms (improved vs stayed the same or worsened) a primary, binary outcome; assuming the results obtained in this study are representative, this study would require a sample size of 72 individuals (36 per group) to have an 80% chance of detecting a difference in clinical improvement with 95% confidence. However, binary outcomes may be more clinically informative and less subject to bias when accompanied by a variety of other well-validated measures. For example, the VISA-A score used in this study is a well-validated and frequently used outcome measure that requires participants to rate their level of activity and the associated amount of pain; this score could serve as a useful outcome measure, as would average daily or weekly ratings of pain, at rest and during activity.
Conclusion
This pilot study explored the potential usefulness of incorporating an existing treatment (topical 10% diclofenac) into future studies of CAT rehabilitation. Because this is a pilot study designed to inform future research, it is not appropriate to generalise or consider issues of external validity. Pain is one of the main symptoms for patients with CAT, and diclofenac was apparently able to help some of the participants manage their Achilles pain during rest and tendon loading. We also learnt that patients naturally generated more force during cyclic tendon loading (hopping) when pain was better controlled, which has implications for the ability to achieve positive tendon adaptations with exercise-based rehabilitation. Diclofenac is therefore a potential option to be incorporated into a larger study on pain and symptom relief during Achilles tendinopathy rehabilitation.
Acknowledgments
The authors acknowledge the valuable contributions of statistician Rick White,† research engineer Vivian Chung, research assistant Douglas Race and all the staff at the Centre for Hip Health and Mobility, Vancouver. † Deceased 2 September 2016.
References
Footnotes
Contributors ERB drafted the study protocol, piloted study procedures, recruited and consented participants, carried out interventions and data collection, contributed to the statistical analysis and drafted the manuscript. AS, JB and BC assisted in developing the protocol and study procedures and in editing the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Medisca (Burnaby, Canada) supplied the gel base as an in-kind contribution, but they played no role in the design or execution of the study and had no access to the data at any time. Diclofenac was purchased from a commercial pharmacy (Northmount, West Vancouver, Canada) and compounded by them for a fee. ERB was supported in part by a Graduate Student Initiative award from UBC, and Dr AS was supported in part by the Michael Smith Foundation of Health Research. The drug and study supplies and facility usage for the Centre for Hip Health and Mobility were paid through internal (UBC) unrestricted research funds allocated to Dr AS’s tendinopathy research program.
Competing interests None declared.
Ethics approval UBC Clinical Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available by contacting the corresponding author at alex.scott@ubc.ca.