Article Text

Abstract
Objective The aim of this study was to identify and analyse communication skills learning outcomes via a systematic review and present results in a synthesised list. Summarised results inform educators and researchers in communication skills teaching and learning across health professions.
Design Systematic review and qualitative synthesis.
Methods A systematic search of five databases (MEDLINE, PsycINFO, ERIC, CINAHL plus and Scopus), from first records until August 2016, identified published learning outcomes for communication skills in health professions education. Extracted data were analysed through an iterative process of qualitative synthesis. This process was guided by principles of person centredness and an a priori decision guide.
Results 168 papers met the eligibility criteria; 1669 individual learning outcomes were extracted and refined using qualitative synthesis. A final refined set of 205 learning outcomes were constructed and are presented in 4 domains that include: (1) knowledge (eg, describe the importance of communication in healthcare), (2) content skills (eg, explore a healthcare seeker's motivation for seeking healthcare),( 3) process skills (eg, respond promptly to a communication partner's questions) and (4) perceptual skills (eg, reflect on own ways of expressing emotion).
Conclusions This study provides a list of 205 communication skills learning outcomes that provide a foundation for further research and educational design in communication education across the health professions. Areas for future investigation include greater patient involvement in communication skills education design and further identification of learning outcomes that target knowledge and perceptual skills. This work may also prompt educators to be cognisant of the quality and scope of the learning outcomes they design and their application as goals for learning.
- Communication Skills
- Learning Outcome
- Qualitative synthesis
- Systematic Review
- Health Professions Education
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Communication Skills
- Learning Outcome
- Qualitative synthesis
- Systematic Review
- Health Professions Education
Strengths and limitations of this study
As far we are aware, no previous paper has reported a comprehensive systematic literature review and qualitative synthesis of learning outcomes in communication skills across the health professions.
Learning outcomes were restructured using qualitative synthesis to remove duplication and ambiguity; and to be concise, defined and accessible to educators developing individualised education programmes.
The final list provides a comprehensive summary of published literature for consideration by patients, educators, learners and other stakeholders.
The search strategy was limited to the English language and the specific education of communication skills. By restricting the search strategy, we may have excluded papers that contained relevant learning outcomes.
Introduction
It is widely acknowledged that skilled communication is essential for all health professionals. For the purposes of this paper, communication is defined as a two-way process involving speech, writing or non-verbal means that aim to create shared interpretation for those involved.1 As such, effective communication skills are emphasised as a target for health professional education programmes locally2 and internationally (including medicine,3 physiotherapy4 and across interprofessional groups5). Over the past 20 years, there has been a growth in communication skills research, and the implementation of communication skills programmes in entry-level medical programmes has become commonplace worldwide.6 ,7 Despite its recognition as a key competency for practice, communication skills teaching has not been routinely adopted in all health professional programmes, and discourse related to communication skills pedagogy remains less common outside medicine.8
The literature on learning and teaching communication skills includes guides and consensus statements for doctor–patient communication (such as Calgary Cambridge Referenced Observation Guides, the UK Consensus Statement, the Kalamazoo Consensus Statement and the German Basel Consensus Statement).9–12 The content of these documents could be presented as intended learning outcomes (ie, what learners are expected to be able to know and/or do after participation in an education programme). However, many of the individual items in these documents target multiple constructs and do not directly translate into specific learning goals.
Learning outcomes in education design
For many years, researchers in education have proposed alternate ways of structuring goals in educational design. From the 1960s, the term ‘instructional objective’ was used to define a statement expressing what learners should be able to do at the end of the learning period.13 These instructional objectives were designed to be constructively aligned with methods for teaching and assessment.14 Learning objectives have been described as focusing more discretely on observable knowledge, attitudes and skills, whereas the more contemporary term ‘outcome’ is defined as a broader statement of what is achieved and assessed at the end of a course of study.15 ,16 More recently, competency-based medical education (CBME) argues for education organised around a defined set of competencies towards which learning is targeted to achieve proficiency.17 Competencies have been defined as the observable capabilities of a health professional (ie, knowledge, skills, values and attitudes).18 Grant19 and Prideaux20–22 argue that the differentiation of terms is not greatly important, as long as the goals for learning are clear. Regardless of semantics, it is acknowledged that some aspects of healthcare practice are difficult to define in these terms, and the identification of an objective, outcome or a competency may not specify exactly what is to be achieved.20 ,23 This argument suggests that the ‘sum’ of healthcare practice is far greater than the ‘parts’ and that any reduction of complex human behaviour into objectives or competencies may be seen as unhelpful.24 This stance resonates with reports within the communication skills literature, which argue that communication also cannot be separated into its parts.25
Communication as a skill
Although learners may develop many aspects of communication through experience prior to university,26 ,27 effective communication in the context of healthcare practice is highly technical and is likely to require training, deliberate targeted practice and feedback to develop skilled performance.28 ,29
One school of thought in the communication literature is that positioning communication as a set of behavioural skills is reductionist and mistaken.25 ,30 ,31 It has been argued that the ‘atomisation’ of communication into discrete observable skills may not take into consideration the complexity of a communication interaction, and nor does it consider the authenticity and creativity required in complex practice.25 ,31 These authors also argue that the deployment of a communication skill does not necessarily equate to skilled communication.25 ,30 It is important here therefore to make a distinction between learning and assessing skilled communication. Salmon and Young25 may be correct when they contend that by assessing communication skills using a reductionist checklist, there is a risk of trivialising the communication interaction. This is particularly the case if assessment procedures require the demonstration of the many discrete communication skills proposed (ie, the ‘parts’) regardless of the context. Such rating requirements may inaccurately judge the ‘whole’.22 ,25 ,32 However, breaking a complex phenomenon, like communication, into discrete ‘parts’ may allow a novice learner to appreciate what may be required for their own skill development.33 Targeted performance development and self-regulated learning require targeted learning goals: therefore, the clarification of these skills has the potential to be useful for learners and educators.34–36 Learning the component ‘parts’ of a communication interaction may allow for skill acquisition and improved performance of the ‘whole’.37 With increased proficiency, learners would then be able to use these skills in a flexible, personal and creative way depending on the context.33 ,38
Communication skills learning outcomes
To the best of our knowledge, there is only one published review identifying communication skills learning outcomes relevant to multiple health professional groups. In 2013, Bachmann et al8 produced the European consensus on learning objectives (HPCCC: Health Professions Core Communication Curriculum). Bachmann et al use the term learning ‘objective’ in their report to which we attribute the same meaning as the term learning ‘outcome’. The HPCCC presents learning objectives that are based on the literature and a medical communication consensus statement and were developed using an extensive Delphi process. In total, 121 communication experts from 16 countries and 15 professions reviewed learning objectives in four stages. Each stage included a review of drafts, ranking of statements and comments regarding acceptability.8 This process drew on a large community of practice within Europe that has a significant focus on communication in healthcare. The HPCCC presents learning objectives that go beyond ‘health professional-patient’ communication and target interprofessional and intraprofessional communication skills. However, the report omits the key quality indicator of detail about the literature review processes, subsequently limiting potential for replication.39 While the Delphi process and the quantitative and qualitative analysis methods were clearly described, the development of the initial draft list of statements is less clear.
Research aim
The work presented here builds on the contributions of previous studies and aims to identify and analyse communication skills learning outcomes via a systematic review and to present the results in a synthesised list.
Methods
Methodology
Research design
A systematic review of the literature (stage 1) was completed to assemble published learning outcomes relevant to health professional communication skills. A parsimonious set of learning outcomes was then developed through an explicit and iterative process of qualitative synthesis (stage 2).
Research team
The research team for stage 1 was the core research team (CD, EM, JLK). Researchers in the field (RW-K, DN, FK: see acknowledgements) joined the core researchers, expanding the research team to six for stage 2 of this study. The stage 2 team consisted of educational researchers, social scientists and an educational linguist based in medical education. Four of the members had clinical backgrounds (physiotherapy). The members had published extensively across health professions education and communication skills research in areas that included scale development, healthcare simulation education, communication skills teaching, curriculum and resource development, feedback and assessment, clinical education and interprofessional education. All members were actively involved in the education of prequalification and postqualification health professional students and medical education research.
Theoretical perspective and guiding principles
This work forms part of a broader research programme exploring the social construction of skilled communication in the health professions. According to social constructionism, knowledge and meaning are constructed through the interaction of a learner and the surrounding environment; therefore, multiple realities exist and there is no ‘true’ interpretation of a phenomenon.40 In this work, we did not set out to define a single truth in relation to learning targets for communication skills. Instead, we investigated published interpretations of this phenomenon and synthesised the findings for application in education. The research team considered that the results of this review would provide a foundation for others to interpret rather than a prescriptive list.
As a research team, we also ascribed to the notions of person-centredness during the qualitative synthesis phase of this study. Aligning with social constructionism, patient-centredness appreciates the individual and social dimensions of a phenomenon. Values of person-centredness including acknowledging patient-as-person and the multiple other persons involved in healthcare practice (eg, colleagues, students and the health professional themselves), and sensitivity to another's perspective and preferences41 informed the choice of language in the results of this work.
Stage 1: systematic literature review
The first stage of this work was a systematic literature review to identify published learning outcomes of health professional communication skills programmes.
Inclusion and exclusion criteria
For inclusion, papers must have described learning outcomes within an education programme targeting the development of communication skills. Participating learners had to be health professionals and could be of any health profession and level of education. Any statement describing what learners were expected to know and/or do after participation in a programme was included, irrespective of the terminology used (eg, learning outcomes, objectives, targets and goals). Knowledge, behavioural and attitudinal learning outcomes were included. Papers were excluded if not available in English, if the education targeted English language fluency or the learning outcomes related to improvement of communication disorders (eg, those related to deafness or aphasia). Any study design was eligible for review.
Search strategy
A comprehensive search was conducted in August 2016, on the full holdings of MEDLINE, PsycINFO, ERIC, CINAHL plus and Scopus databases. Search terms included health professional, communication, training and their synonyms. The strategy used to search OVID databases is presented in online supplementary appendix A. The full yield from each database was exported to a bibliographic management system and duplicates deleted. On the basis of the title and abstract, papers that were ineligible were deleted. The remaining papers were read in full, and their eligibility was assessed against the inclusion and exclusion criteria. The primary author (CD) independently reviewed all papers and consulted with authors JK and EM on papers when eligibility was difficult to determine.
supplementary appendix
Data extraction
Table 1 describes the data that were extracted from each paper. All data were descriptively analysed and synthesised for discussion. Learning outcomes described in each paper were extracted and referenced to the source using an alphanumeric identifier. They were pooled and common learning outcomes were collated under preliminary themes, and subthemes, in a process of thematic analysis for commonality.42 Preliminary thematic groups rendered the data set manageable for qualitative synthesis. The core research team (CD, EM, JLK) collaborated to delete duplicated learning outcomes (eg, those with exact wording) that were revealed as the learning outcomes were collated.
Items for data extraction
Quality analysis
This work does not resemble a traditional systematic review, in that quality assessment was not carried out on the included papers as we were not attempting to establish the validity of the recommended learning objectives. A systematic review approach, however, was used to identify eligible papers to enable transparency and replication and to address the research aim. Aligning with this aim, our focus was to extract the learning outcomes used in education design and review the content and quality of these statements. In other words, we applied a quality assessment filter to the learning outcomes (see decision guide, figure 1), not to the papers themselves.

Decision guide.
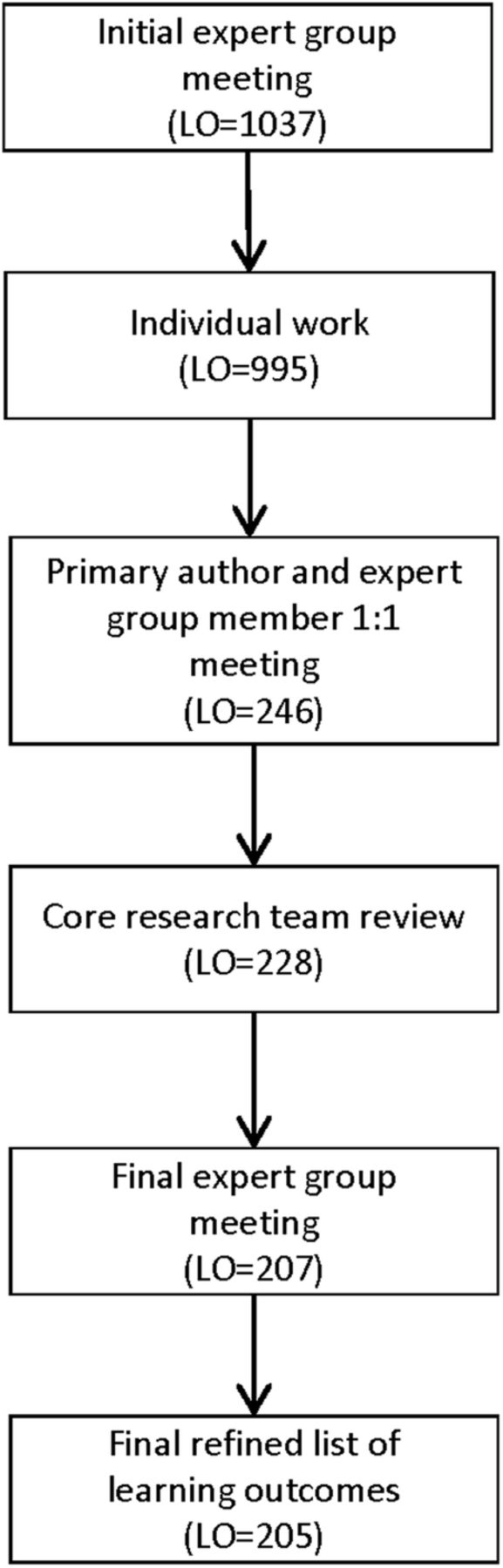
Stage 2: qualitative synthesis
In stage 2, learning outcomes identified in stage 1 were synthesised by the research team through an iterative process of individual, paired and group work. An initial meeting of the expanded research team was convened, and a random subset of learning outcomes was taken from the data set to rehearse the process of learning outcome synthesis. Synthesis was guided by the notions of person-centredness, and the decision guide is shown in figure 1. The decision guide was adapted from that used by Dalton43 in the refinement of assessment targets for competency to practice. This set of criteria was deemed the most fitting to guide the construction of learning outcomes. The decision guide was used to judge the quality of the learning outcomes and to address semantics in order to emphasise the important characteristics when constructing statements to be used for goal setting and practice.28 ,36 ,43
Following this group meeting, the remaining learning outcomes were divided into five equivalent sections (eg, equivalent work per group member) and each member completed an individual review of one section. The primary author (CD) reviewed all sections.
Following this individual work, the primary author met with each member to compare work. After consensus was reached on all five sections, the core research team (CD, EM, JLK) reviewed themes and subthemes to reflect the synthesised data set. The refined learning outcomes were returned to the full group for consideration with a request for individual review prior to finalisation. A final group meeting enabled consensus regarding content, definition of terms and structure and presentation of the document.
Throughout the synthesis process, the number of learning outcomes was reduced as the research group collapsed multiple learning outcomes into one representative learning outcome, as further duplicates were identified, and as the group modified learning outcomes to align with the decision guide (see table 2 for an example of the qualitative synthesis process). At each step of this iterative process, the research group engaged in discussion to resolve different interpretations of the data, to highlight concepts that were absent from the data set, to resolve inconsistencies in language/terms and to ensure the learning outcomes continued to reflect the source literature. The primary author (CD) made an audit trail of decisions throughout the analysis. The audit trail included clear documentation of the process to make transparent the methods used in learning outcome refinement.44
Example of qualitative synthesis
Results
Stage 1: literature review
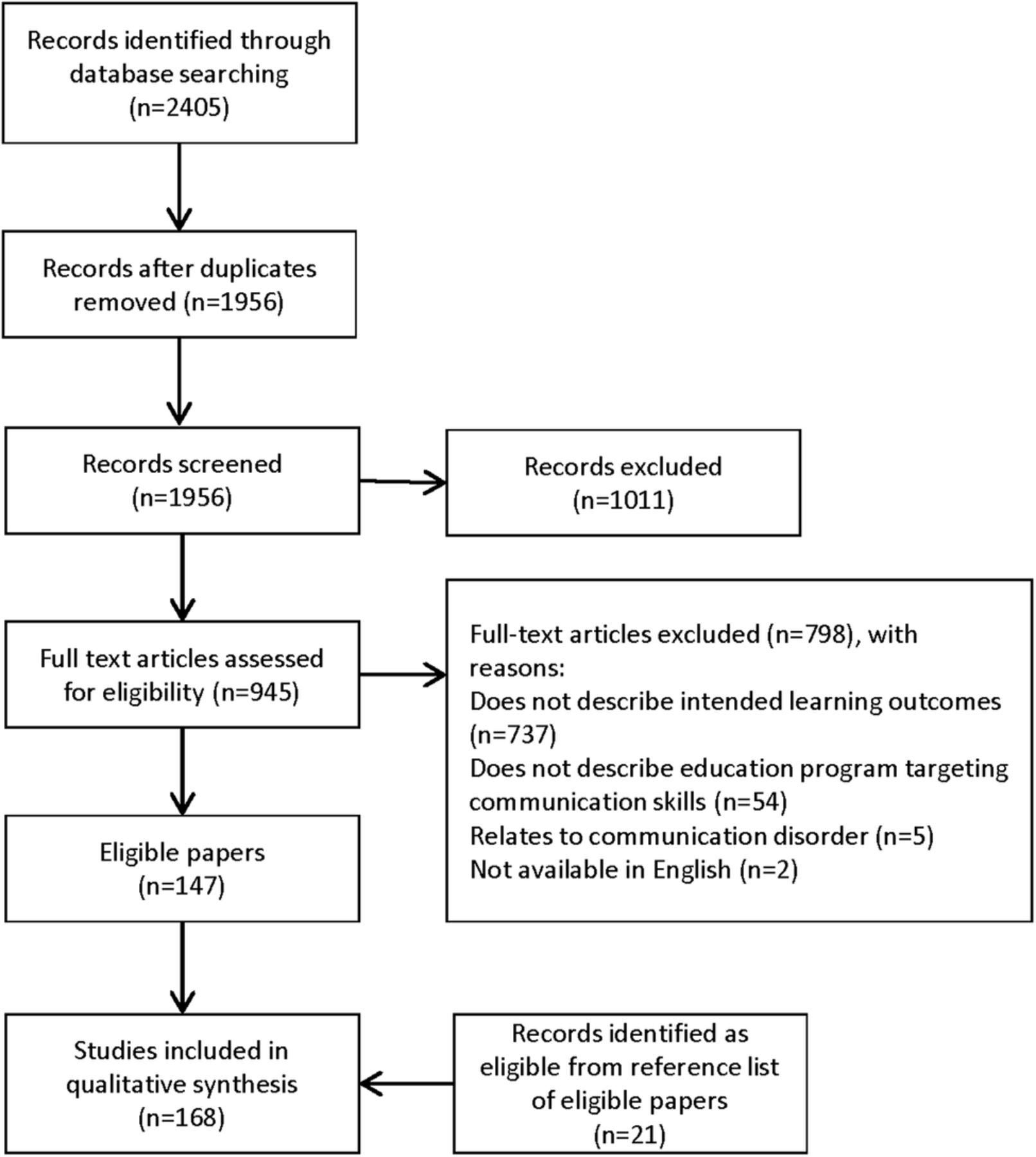
A total of 168 papers were included for review (figure 2). Full reference details of eligible papers are presented in online supplementary appendix B; further details are available on request from the primary author. A summary is presented below and in table 3.
Data extraction

Flow of papers into the review.
supplementary appendix
The highest proportion of included papers was primary research (64%). There was a variety of study designs including randomised controlled trials investigating change in behaviour and posteducation learner evaluations. The majority of papers were published between 2010 and August 2016 (46%), originated from the USA (56%), described communication teaching in medicine (55%) and in qualified health professionals (56%). Learners in oncology (10%) outnumbered learners in other fields of practice. Learners in second year were most common in the prequalification population (8%). Many papers did not report a theoretical perspective of their work (58%); of those that did, the most common perspective reported was patient-centred care principles (7%).
Many included papers (40%) did not report any specific communication models that informed teaching. If cited, the most frequent models were the Kalamazoo Consensus Statement (7%), Calgary-Cambridge Referenced Observation Guides (5%) and the Three Functions of the Medical Interview (5%); a variety of other communication models were reported <4% of the time. Other factors that informed educational design were stakeholder engagement, with 51% of reports documenting turning to clinicians, researchers and the literature to design the learning outcomes of their programmes. Only 5% reported engaging patients as stakeholders in the development of programmes.
A total of 1669 learning outcomes for communication skills education were extracted from eligible papers; duplicated learning outcomes were deleted, reducing the list to 1073.
Stage 2: qualitative synthesis
The 1073 learning outcomes identified in stage 1 were condensed to a final set of 205 learning outcomes (figure 3). The learning outcomes are presented in themes of ‘knowledge’, ‘content’, ‘process’ and ‘perceptual’ skills. Three of these themes are based on the seminal work of Kurtz, Silverman and Draper.45 The research group added a fourth theme, knowledge (see table 4 for detailed definitions and other terms used in the final learning outcomes document). ‘Knowledge’ learning outcomes made up 20% of the final list of learning outcomes. They relate to knowledge of the characteristics and modes of communication in healthcare and how emotions and relationships affect communication in healthcare. Learning outcomes within the ‘content’ and ‘process’ themes dominate the literature and therefore are represented heavily in the final set (36% and 35%, respectively). These learning outcomes include the important ‘what’ and ‘how’ of communication skills.46 The learning outcomes within the content domain have been presented in the chronological sequence of a healthcare interaction for ease of representation.47 ,48 Learning outcomes under the ‘perceptual’ skill theme made up 9% of learning outcomes in the final results. This final list of learning outcomes covers a wide range of skills proposed for communication teaching and is presented in online supplementary appendix C.
Final learning outcomes: themes and definitions
{kind=link}
{kind=link}
{kind=link}
Flow of learning outcome (LO) refinement.
supplementary appendix
Discussion
The aim was to identify and analyse communication skills learning outcomes via a systematic review and present results in a synthesised list for consideration and use by educators and researchers across the health professions. From 168 included papers, 205 learning outcomes for communication skills evolved through qualitative synthesis. As far as we are aware, no previous review has reported on a comprehensive systematic literature review to identify learning outcomes for communication skills and presented them for uptake across the health professions.
What did we learn about communication skills learning outcomes?
Patients are less likely to be involved in education design
Patient-centred communication is considered fundamental to effective healthcare delivery, but these principles are not consistently used as a basis for communication skills teaching, with only 7% of papers reporting patient-centred care as an underpinning theoretical perspective. In addition, only 5% of papers reported engaging patients in any aspect of educational design. Although valued in health professions education, patient engagement is not well defined.49 Regan de Bere and Nunn50 have proposed ideas for the future pedagogy of patient (and public) involvement in health profession education. It seems appropriate that future communication skills educational design follows this lead and engages patients (and public) in the design of teaching and learning to explore what patients expect from health professionals, in terms of communication, as well as to acknowledge patients and patient-centred care as a unifying focus in health professions education.50
Knowledge and perceptual skills are less common
Unlike the learning outcomes reported in the HPCCC, this paper includes learning outcomes relating to behaviour and knowledge. Knowledge forms part of the initial phases of scaffolding for learning and assessment,51 and in learning theories describing skill development, a learner usually needs to know the terms and context of behaviour before they learn the behaviour itself.52 In the past, knowledge-based learning outcomes have been criticised for being overemphasised in approaches to educational design, at the expense of behavioural learning outcomes.18 In the communication skills literature, perhaps the emphasis has swung too far away from the knowledge agenda with most publications only reporting behavioural learning outcomes. The presented list brings communication skills in line with other skills teaching, by acknowledging the integration of knowledge and behaviour in ‘technical’ skill development.28
Learning outcomes under the perceptual skill theme made up only 9% of learning outcomes in the final results. These learning outcomes relate to awareness and evaluation of self, others and context, which are considered important in reflective, self-regulating health professionals.34 ,53 Despite ample literature promoting reflective practice in the health professions education field in general,54 published programmes on communication skill development seem less focused on incorporating learning objectives to target these evaluative skills. The low level of reporting of perceptual skill objectives may reflect the challenge in defining these skills so that they are objective and measurable. Healthcare communication is unique, complex and nuanced, and therefore objectivity when defining these desired communication skills can be elusive.26 However, clearly articulating these important skills is key to defining learning goals for performance development.
Language can be modified for greater application
During the qualitative synthesis process, the research group identified many of the learning outcomes that were specific to communication with a patient but that could equally apply to other communication interactions. The term ‘patient’ appeared in many included learning outcomes and was replaced in the refined list with the term ‘healthcare seeker’. The term healthcare seeker was more broadly applicable across healthcare contexts and acknowledged the active role that an individual can have in regard to his/her health. While the original learning outcome may have referred to communication between a health professional and care seeker, in some instances we found that learning outcomes could be easily reshaped to apply to communication with a different ‘communication partner’ entirely (eg, colleague or student). This parallel between skills in a therapeutic interaction and a collegial or educational interaction has been identified by others.55 ,56
The research team also replaced all profession-specific terms identifying the target learner (eg, dentist) with the term ‘health professional’ as most learning outcomes had potential application to a variety of professions. The identification of these common learning outcomes may provide a platform for interprofessional education and facilitate a shift from ‘siloed’ health professional education to ‘collaborative’ practice, and education, within which communication is considered an essential common skill.57
Learning objectives are often unclear or absent
Previous reviews reporting communication skills in medical education have criticised the quality of published learning outcomes, reporting that they were unclear or absent in many papers on communication education.47 ,58 This was reflected in the current review with only 208 papers, of the 945 full text screened, reporting specific learning outcomes for the education described. Like Cegala and Lenzmeier Broz,47 the authors acknowledge that the word count of many journals limits the inclusion of exhaustive lists of learning outcomes. However, even when learning outcomes were reported, they often targeted two to three constructs per statement, included value-laden words such as ‘good’ (eg, use good non-verbals) and many were ambiguous in their intention (eg, be able to apply the necessary communication skills adequately in a simulation). During stage 2 qualitative synthesis, the use of the decision guide focused attention on the design features of useful learning outcomes and guided the synthesis process. For example, many learning outcomes such as ‘show empathy’ were not accompanied by a descriptor or defined example; this rendered them neither useful, nor measurable or transparent (see figure 1, decision guide). For learning outcomes such as this, we made the decision to combine all learning outcomes describing ‘empathic’ behaviour under a single learning outcome ‘demonstrate empathy in the following ways’: after which a list of observable behaviours were assembled (see item no. 136 in online supplementary appendix C). This method of illustrating these ‘slippery’ learning outcomes, with observable behaviours, aimed to shape the learning outcome into a useful, measurable and transparent structure that would guide educators and learners.
Study strengths and limitations
This paper has a number of limitations. By casting a wide net in this literature review, we drew from the worldwide interest in this topic. In targeting a breadth of perspectives, we identified diverse studies, from educators across professions, which informed the results. A side effect of the broad search was the challenge of dealing with a large amount of data. Multiple stages of thematic analysis and refinement were required to create a manageable data set. The process of refinement necessarily included removal or rewording of items. We cannot be sure that this has not led to omissions in the final set of learning outcomes. However, the iterative nature of the qualitative synthesis process meant that all attempts were made to produce a representative list. Although these results represent a wide range of literature, they do not include input from other key stakeholders (ie, care seekers, representatives from different healthcare professions, learners and educators). Therefore, we do not claim that this is a complete list of learning outcomes illustrative of all stakeholders' needs. By focusing on specific communication skills education, we may have excluded communication learning outcomes in patient safety or clinical reasoning education programmes. In addition, we excluded papers reporting on communication disorders or English language fluency which may have also provided relevant learning outcomes.
Implications for practice and future research
This work provides educators and learners with a comprehensive set of learning outcomes for educational design and goal setting in healthcare communication. Aligning with a social constructionist perspective, we invite stakeholders to take these learning objectives and reinterpret them based on their context. This work may prompt educators to reflect on how knowledge and perceptual skills are taught in domains such as communication and to encourage educators to be cognisant of the quality of the learning outcomes they design.
Further research is required to interrogate these learning outcomes for accuracy and completeness by engaging with stakeholders (including care seekers) to align targets for learning with targets for practice. Future research might also explore the parallels between communication skills needed in care seeker interactions and those required for other healthcare conversations (eg, between healthcare professionals, trainees or policymakers). Perhaps by positioning communication skills as skills that are required with any ‘communication partner’, we can equalise the gravitas generally afforded to ‘doctor–patient’ communication in this field of literature.
Conclusions
This paper presents a synthesis of the vast literature in communication skills teaching and a list of 205 learning outcomes. These learning outcomes have been categorised into four domains and provide educators from across the healthcare professions with a basis from which to develop learning goals and programmes relevant to their setting.
Acknowledgments
The authors acknowledge Dr Fiona Kent for her contribution to the qualitative synthesis phase of this review.
References
Footnotes
Contributors CD, EM and JLK designed the work. CD conducted the systematic review search and data extraction in stage 1. All authors (CD, EM, JLK, DN and RW-K) were involved in qualitative synthesis and analysis in stage 2. CD drafted the first version of the manuscript. All authors reviewed and revised the manuscript and approved the final version.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.