Article Text

Abstract
Objective To assess associations between dietary intake and carotid intima media thickness (CIMT) by carotid ultrasound (CUS), a surrogate marker of cardiovascular disease (CVD) risk, in those with type 2 diabetes.
Design Cross-sectional analysis of baseline data from 325 participants from three randomised controlled trials collected in the same way.
Setting Risk Factor Modification Centre, St. Michael's Hospital, Toronto, Canada.
Participants 325 participants with type 2 diabetes, taking oral antidiabetic agents, with an HbA1c between 6.5% and 8.0% at screening, without a recent cardiovascular event.
Main outcome measures CIMT by CUS and associations with dietary intake from 7-day food records, as well as anthropometric measures and fasting serum samples.
Results CIMT was significantly inversely associated with dietary pulse intake (β=−0.019, p=0.009), available carbohydrate (β=−0.004, p=0.008), glycaemic load (β=−0.001, p=0.007) and starch (β=−0.126, p=0.010), and directly associated with total (β=0.004, p=0.028) and saturated (β=0.012, p=0.006) fat intake in multivariate regression models adjusted for age, smoking, previous CVD event, blood pressure medication, antidiabetic medication and ultrasonographer.
Conclusions Lower CIMT was significantly associated with greater consumption of dietary pulses and carbohydrates and lower total and saturated fat intake, suggesting a potential role for diet in CVD risk management in type 2 diabetes. Randomised controlled trials are anticipated to explore these associations further.
Trial registration number NCT01063374.
- NUTRITION & DIETETICS
- DIABETES & ENDOCRINOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A strength of the study methods includes the use of carotid intima media thickness (CIMT) by carotid ultrasound, which is the recommended screening tool for assessing cardiovascular disease (CVD) risk by some CVD prevention clinical practice guidelines, considered a biomarker of atherosclerosis and is associated with overall CVD risk, particularly in those with type 2 diabetes.
The CIMT scans were all performed by one of two highly trained ultrasonographers using the same scanner at the same site and using the same reading protocol.
The dietary data are obtained from 7-day dietary food records in which participants were trained on how to complete by study dietitians and which at each visit were reviewed in detail by study dietitians in the presence of the participant.
A limitation of the analyses includes that they are conducted using CIMT results from only one CIMT scan obtained at baseline; however, studies have demonstrated mean max CIMT measurements to have good reproducibility, particularly using the method we adopted where measurements are made of 12 segments of the carotid artery.
Although at higher CVD risk, participants in this study had relatively well-controlled diabetes, blood pressure and low-density lipoprotein cholesterol, with the majority on blood pressure and cholesterol-lowering medication at baseline, therefore possibly limiting the ability to assess associations between risk factors for CVD and CIMT and dietary intake, as well as limiting application to those with uncontrolled risk factors.
Introduction
People with type 2 diabetes are at high risk of cardiovascular disease (CVD), the leading cause of death in this population.1 ,2 Risk assessment through atherosclerosis imaging includes the use of carotid intima media thickness (CIMT) by carotid ultrasound (CUS), the recommended screening tool for assessing CVD risk by some CVD prevention clinical practice guidelines.3 ,4 CIMT is considered a biomarker of atherosclerosis and is associated with overall CVD risk, particularly in those with type 2 diabetes.5 ,6 Observational studies have recently demonstrated that carotid atherosclerosis, assessed by CIMT, is associated with glycaemic status7–9 and intervention trials with antidiabetic agents have demonstrated reductions in CIMT both in those with and without diabetes.10–12 Some of these antidiabetic agents exert their effect postprandially, by reducing the postprandial blood glucose peak. Trials of insulin secretagogues (nateglinide and repaglinide) and the α-glucosidase inhibitor, acarbose, have demonstrated reductions in CIMT and identified markers of glycaemia (HbA1c and glucose peak) as determinants of changes in CIMT.10 ,13–15
In addition to antidiabetic drugs, dietary strategies continue to be sought as means to assist in diabetes management. However, few dietary intervention trials have explored the effect on CIMT. These have demonstrated regression of CIMT with a Mediterranean diet pattern.16 Dietary strategies that may be useful for diabetes management, including low-GI (low-glycaemic index) diets17 ,18 and those rich in dietary pulses,19 ,20 have demonstrated associations with improved CVD risk,21 thus warrant exploration of their effects on CIMT as a subclinical biomarker of CVD.
The objective of the present study was to determine the associations between dietary intake variables, particularly GI, and risk of CVD assessed by CIMT in participants with type 2 diabetes.
Methods
Participants
Details of the study protocol have been previously published.22 Participants recruited for a 3-year dietary intervention study had a diagnosis of type 2 diabetes >6 months prior to the start of the study, an HbA1c between 6.5% and 8.0% at screening, were on oral antidiabetic agents at a stable dose for ≥8 weeks, not on insulin, without gastrointestinal disease, clinically significant liver disease or history of cancer, except non-melanoma skin cancer, and had not had a major cardiovascular event or major surgery in the past 6 months. Participants also had a CUS scan at the Medical Imaging Department at Sunnybrook Health Sciences Centre to assess CIMT as part of screening criteria, where only those participants with a maximum CIMT ≥1.2 mm were eligible for the 3-year study. Those who did not meet this CIMT cut-point had the option to participate in one of two concurrent trials of shorter duration, the details of which have been published.23 ,24 This cross-sectional study was conducted on 325 study participants using baseline data from these three trials, all of which had the same inclusion criteria (with the exception of the additional criteria of a maximum CIMT ≥1.2 mm for the 3-year trial) and included 7-day food records, anthropometric measures, fasting blood samples and CIMT measures which were collected in the same way.
Written consent was obtained from all participants.
Design
In this cross-sectional analysis, data were obtained from baseline measures of study participants including CIMT data obtained from CUS scans completed at the Medical Imaging Department at the Sunnybrook Health Sciences Centre MRI research unit. One of two highly trained and certified sonographers performed CIMT measures using a Philips iU22 Ultrasound system (Philips Healthcare, Andover, Massachusetts, USA) with standardised CUS scanning and reading protocols.25 ,26 CIMT was measured with the subject recumbent, with the neck extended and rotated away from the side of interest. As previously described,22 imaging was performed on the right and left carotid arteries, with identification of the near wall (closest to the skin surface) and the far wall (farthest from the skin surface) of three arterial segments: the proximal 8 mm of the internal carotid artery, the carotid bifurcation beginning at the tip of the flow divider (site of the division of flow between the external carotid artery and internal carotid artery) and extending 8 mm proximally, and the common carotid artery 8–16 mm proximal to the flow divider, and measurements included posterior wall plaque, if present. The mean value of the 12 maximal CIMT measurements (mean maximum CIMT) was used as the outcome measure, which has demonstrated good reproducibility (interclass correlation coefficient (ICC) >0.8).27
For participant baseline data on risk factors, all three studies included two baseline clinic visits at the Risk Factor Modification Centre, St. Michael's Hospital and occurred within 1 month of each other. At the first, baseline anthropometric and fasting blood measures were obtained. Participants were given detailed instruction on how to complete a 7-day food record which was returned at the next visit. At the second baseline clinic visit, anthropometric and fasting blood measures were again obtained and each participant was randomised. Anthropometric data included body weight, seated blood pressure measured as the mean of triplicate measures made with an automatic sphygmomanometer (Omron HEM 907 XL, OMRON Healthcare, Burlington, Ontario, Canada), and waist (at the umbilicus, 2 inches above and lying down) and hip circumference. Blood measures included HbA1c, fasting glucose and fasting lipids. Data were also obtained on demographics including age, sex, estimated duration of diabetes, smoking and medication use.
For those who participated in more than one of the three studies (n=14), their first CUS and corresponding baseline study measurements were used in the present analyses.
Biochemical and dietary analyses
The HbA1c value was analysed within 24 hours using whole blood collected in EDTA Vacutainer tubes (Vacutainer; Becton, Dickinson and Co) in the hospital routine analytical laboratory by a turbidimetric inhibition latex immunoassay (TINIA Roche Diagnostics) with a coefficient of variation between assays of 3–4%. Blood glucose and serum lipid levels were also measured in the hospital routine analytical laboratory using a Random Access Analyzer and Beckman reagents (SYNCHRON LX Systems; Beckman Coulter), with a coefficient of variation of 1.6–2.3% for blood glucose level and 1.3–3.0% for total cholesterol (total-C), triglycerides, and high-density lipoprotein cholesterol (HDL-C) levels. The low-density lipoprotein cholesterol (LDL-C) level was calculated by the method of Friedewald et al28 (LDL-C level=total-C−[(triglycerides/5)×(HDL-C level)]).
Dietary assessments using participant completed 7-day food records were analysed using a computer program (ESHA Food Processor SQL V.10.9; ESHA, Salem, Oregon, USA) based on the USDA database,29 supplemented with data from the Canada Nutrient File,30 and with GI values from international GI tables31 using the bread scale (where bread=100; for the glucose scale, multiply by 0.71). Glycaemic load (GL) was calculated as GI*available carbohydrate÷100. Product data were updated with manufacturers' nutrient information and relevant foods were analysed by Covance Laboratories (3301 Kinsman Blvd, Madison Wiscosin, USA). Owing to interest in GI, in addition to general dietary variables, data on particularly low-GI foods, which we and others had previously demonstrated to have benefit in diabetes management,23 ,32 ,33 were extracted from the food records, including dietary pulses, temperate climate fruit and nut intake.
Statistical analyses
These are post hoc analyses performed on all baseline study participants who had a CUS scan (n=325). The original power calculation was based on the main intervention trial. However, we performed post hoc sample size calculations to assess our ability to detect associations of GI and CIMT. Given the slope of −0.210 for GI and CIMT, the SD of our log transformed GI of 0.075, the SD of our Box-Cox transformed CIMT of 0.229, and with 80% power and α=0.05, to detect an association, we would need a sample size of 1640. This may be a reflection of our lack of range of exposure levels of GI at baseline (range: 58–98 and IQR: 76–83, bread scale). We have also calculated a post hoc sample size for dietary pulses, as a particularly low-GI food which we previously demonstrated to have benefit on CVD risk factors in diabetes,23 given a slope of −0.025 for dietary pulses and CIMT, and an SD of our log transformed dietary pulses of 1.592, 254 participants would have been sufficient to detect an association at α=0.05, 1−β=0.80. Data are expressed as means±SD unless otherwise indicated. Multivariate mixed-effects regression models were conducted using SAS software, V.9.4 (SAS Institute: SAS/STAT Proprietary Software 9.4. Cary, NC: SAS Institute; 2002–2012.) to assess the association between dietary intake and CIMT. Dietary variables were energy adjusted by expressing intake as g/1000 kcal or as a percentage of energy. To adjust for energy in GI and GL analyses, total caloric intake was added to the models as a continuous variable. All dietary variables were analysed as continuous variables. Sensitivity analyses were performed where energy was alternatively adjusted for using the residual method. Since there are multiple potential confounders with CIMT, including age, sex, smoking, prior CVD event, cholesterol medication use, blood pressure medication use, duration of diabetes, type of antidiabetic medication and waist circumference, we included only those that were significantly associated with CIMT in our data set (at p<0.1). Therefore, the multivariate model was adjusted for age, smoking, previous CVD event, blood pressure medication and type of antidiabetic medication. Smoking was defined using three categories: current (current smoker or quit within the past year), former (quit between 1 and 15 years ago), and non-smoker (never smoked, or quit over 15 years ago) according to the WHO definitions of coronary heart disease (CHD) risk.34 Previous CVD event was defined as yes or no. Use of blood pressure-lowering medication was defined as user or non-user based on the baseline visits. Type of antidiabetic medication was defined as user of a sulfonylurea or thiazolidinediones or non-user since these have been demonstrated to have potential negative associations with CVD risk.13 ,35 ,36 Of the 325 participants with a CIMT measurement and who were randomised into one of the three studies, one participant did not attend their week 0 visit, thus did not have dietary data. Overall 10-year CVD risk was calculated using the Framingham risk score according to the 2008 Framingham cardiovascular risk equation.37 Ultrasonographer, another potential confounder, was treated as a random effect throughout analyses. CIMT was non-normally distributed, therefore was transformed using the Box-Cox transformation.38 The λ for CIMT was −1, thus, (CIMT−1−1)/−1 was used for the transformation. Dietary variables were transformed using the natural logarithm in models where the model fit improved (adjusted R-squared increased) in the adjusted model when being regressed against transformed CIMT. The transformed dietary variables include: GI, dietary pulses, temperate climate fruit, dietary fibre, viscous fibre, cereal fibre, starch, monounsaturated fatty acids, omega 3 fatty acids, dietary cholesterol and vegetable protein. Thus, these dietary variables were transformed as ln[g/1000 kcal (or %kcal) +1]. Probability values <0.05 were considered statistically significant.
Results
Characteristics of the 325 study participants are presented in table 1. The average mean maximum CIMT was 1.0±0.3 mm and maximum CIMT was 2.0±0.9 mm. The mean age for all participants was 60.3±8.7 years, 56% were male, the mean body mass index (BMI) was 30.3±5.7 kg/m2, and the mean waist circumference was 105.5±15.0 cm in females and 104.1±12.3 cm in males. Fifteen participants (4.6%) had a previous CVD event, 84.6% non-smokers, 10.2% former smokers and 5.2% were current smokers. Of the participants, 72.3% were taking cholesterol-lowering and 66.5% blood pressure-lowering medications.
Participants characteristics
CIMT and baseline dietary intake
The associations between CIMT and dietary variables using multivariate regression models are presented in table 2. CIMT was significantly inversely associated with GL (β=−0.001, p=0.007), dietary pulses (β=−0.019, p=0.009), available carbohydrate (β=−0.004, p=0.008) and starch (β=−0.126, p=0.010), and positively associated with total fat (β=0.004, p=0.028) and saturated fat (β=0.012, p=0.006), in multivariate models. Sensitivity analyses using the residual model for energy adjustment, revealed consistent results (data not shown).
Dietary intake and associations with carotid intima media thickness
CIMT and risk factors
CIMT was significantly positively associated with age (β=0.011, p<0.001; unadjusted), waist-to-hip ratio (β=0.529, p=0.019), systolic (β=0.004, p<0.001) and diastolic blood pressure (β=0.003, p=0.035), mean arterial pressure (β=0.005, p=0.002), pulse pressure (β=0.005, p<0.001), total:HDL-C ratio (β=0.027, p=0.020) and FRS (β=0.005, p<0.001), and inversely with pulse (as beats per minute) (β=−0.002, p=0.047) (table 3) in multivariate models. Non-smoking was associated with significantly lower CIMT when compared to current smokers (β=−0.160, p=0.003) and to former smokers (β=−0.094, p=0.004) (table 3).
Participant characteristics and associations with carotid intima media thickness
Post hoc explorations with CIMT
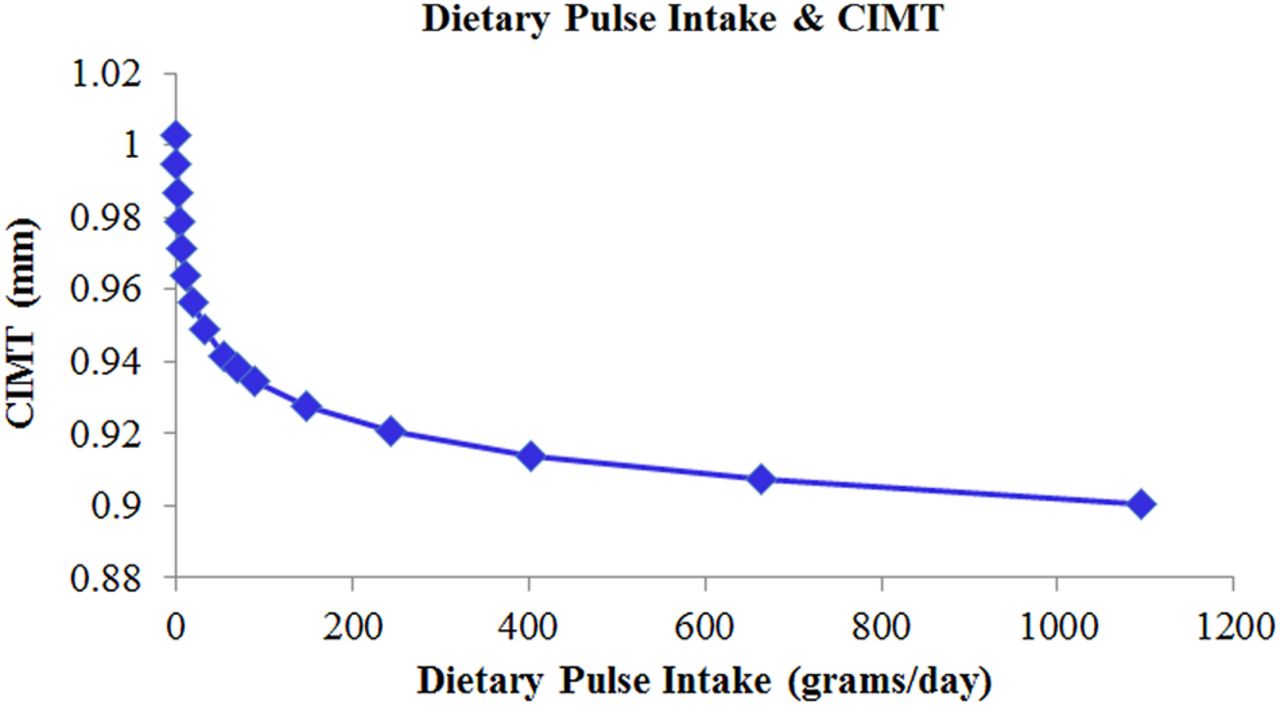
Further explorations were conducted using the multivariate model to predict how CIMT in a person consuming one serving of dietary pulses per day would compare to a person not consuming any. Data points were obtained by taking mean values for log dietary pulse intake in the regression equation (at 0 and 0.5 increments up to 5) and then back transforming the β estimates for the response variable (transformed CIMT). The predicted model of the association between CIMT and dietary pulse intake revealed a logarithmic association (figure 1) where approximately one ¾ cup Canadian serving/day (∼132 g/day)39 was associated with a 7.5% lower CIMT compared with no intake (0 g/day) (0.078 mm CIMT difference). The same was conducted for saturated fat which demonstrated a linear association where for every 1% of total calorie increase in saturated fat, CIMT was about 0.011 mm greater (see online supplementary figure S1).
{kind=link}
Model of association between dietary pulse intake and carotid intima media thickness (CIMT). The multivariate regression model is adjusted for age, smoking, previous cardiovascular disease (CVD) event, blood pressure medication, antidiabetic medication and ultrasonographer.
supplementary data
To explore the association with starch further, each major source of starch in the diet was assessed, including potato, pasta, rice, bread and pulses. Grams of starch from each carbohydrate source were calculated using the following foods: boiled white potato, cooked macaroni for pasta, long grain rice, white and whole wheat bread, and the average starch from three beans (chickpea, black bean and kidney bean) and lentils. Starch from each source was expressed as a percentage of total calories (%kcal) for each variable in the model. All other sources were pooled (other starch). All starch sources were added to the adjusted model and then removed as necessary using a backwards stepwise regression. Dietary pulse starch and rice starch were the only significant contributors to the negative association of starch with CIMT (p=0.048 and p=0.023, respectively) (table 4). Dietary pulse and rice intake were also highly positively correlated with each other (r=0.272, p<0.001).
Starch sources and association with carotid intima media thickness
Post hoc explorations were also conducted to assess associations between the metabolic profile of participants and all dietary variables (see online supplementary table S1). Of the dietary variables significantly associated with CIMT, greater intake of dietary pulses, carbohydrates, starch and GL and lower intake of fat and saturated fat were generally associated with lower body weight (r=−0.129, p=0.021; r=−0.210, p<0.001; r=−0.175, p=0.002; r=−0.157, p=0.005; r=0.202, p<0.001; r=0.321, p<0.001, respectively), systolic blood pressure (r=−0.145, p=0.009; r=−0.141, p=0.012; r=−0.130, p=0.020; r=−0.143, p=0.011; r=0.063, p=0.260; r=0.030, p=0.592, respectively), diastolic blood pressure (r=−0.172, p=0.002; r=−0.123, p=0.028; r=−0.135, p=0.016; r=−0.109, p=0.053; r=0.094, p=0.095; r=0.114, p=0.042), total-C (r=−0.118, p=0.036; r=−0.129, p=0.021; r=−0.160, p=0.004; r=−0.132, p=0.019; r=0.119, p=0.034; r=0.092, p=0.101) and LDL-C (r=−0.109, p=0.052; r=−0.128, 0.022; r=−0.151, p=0.007; r=−0.116, p=0.039; r=0.131, p=0.019; r=0.059, p=0.296) in adjusted Pearson correlations.
Discussion
Using CIMT as a predictive marker of CVD risk, we evaluated the associations with dietary intake in participants with type 2 diabetes. The objective of the main study from which these baseline data are taken is to assess the effect of a low-GI diet on markers of macrovascular disease, however, in the present cross-sectional analysis, there was no significant association between GI and CIMT. This may be because we were underpowered due to the small variance of measured GI in our population, no participant had a high-GI diet and the average GI was at the low end of the medium GI range, thus limiting our ability to assess any association. Although we found no association, low-GI diets have been demonstrated in systematic reviews and meta-analyses of randomised controlled trials to significantly reduce both total-C and LDL-C compared to high-GI diets,40 as well as to reduce oxidative stress and inflammation.41 Interestingly, in a recent randomised controlled trial of those with the metabolic syndrome randomised to receive either metformin or a low-GI diet for 8 weeks, both groups demonstrated significant improvements in metabolic syndrome components including body weight, blood pressure, cholesterol and glycaemia.42 Furthermore, the antidiabetic drug acarbose, which effectively converts the diet into a low-GI diet by delaying dietary carbohydrate absorption, has been associated with a reduced incidence of hypertension and CHD events in a small number of prediabetic participants in the Study to Prevent Non-Insulin-Dependent Diabetes Mellitus (STOP NIDDM) trial.43 Therefore, low-GI diets may have the potential to reduce CVD risk, particularly in those at high risk. Thus, further exploration into the potential benefit of low-GI diets on CVD risk is needed, particularly to assess change due to low-GI interventions.
GL was significantly associated negatively with CIMT which differs from what was expected. Systematic reviews and meta-analyses of previous studies have demonstrated a positive association between GL and CVD risk.17 ,18 However, GL is the product of GI and available carbohydrate. We found a strong significant negative association between available carbohydrates and CIMT, but no effect of GI. We found a strong positive association between total and saturated fat intake and CIMT, therefore the surprising negative association between GL and CIMT may just mean that a higher carbohydrate and GL diet is simply an indicator of a lower total and saturated fat diet that predictably was associated with lower CIMT.
Of the specific low-GI foods of interest assessed, dietary pulse intake was significantly inversely associated with CIMT. In the predicted model (figure 1) approximately one ¾ cup serving/day39 was associated with a 7.5% lower CIMT compared to no intake (0 g/day). Although associations with CIMT have not been assessed previously, dietary pulse intake has been associated with reduced risk of CHD and CVD,19 ,20 which supports the association found in the current study between dietary pulse intake and CIMT as a subclinical marker of CVD risk. Additionally, dietary pulses are part of a Mediterranean diet and this diet has been associated with improved CIMT in a number of studies,16 ,44–46 as was highlighted in a recent systematic review of dietary factors and CIMT by Petersen et al.47 We also found dietary pulse intake to be significantly associated with lower body weight, systolic and diastolic blood pressure, mean arterial pressure and cholesterol (see online supplementary table S1). A series of systematic reviews and meta-analyses have found dietary pulse intake to significantly improve body weight, blood pressure and cholesterol,48–50 therefore supporting the associations observed in this study. Each of these potential pathways has been associated with lower CVD risk. Additionally, dietary pulses are high in fibre, potassium and vegetable protein, and low in saturated fat, each of which has been demonstrated to lower blood pressure23 ,51 ,52 and improve cholesterol.48 Furthermore, although not explored in the current study, dietary pulses may also act through reduced inflammation, as supported by another recent systematic review and meta-analysis,53 which may also affect carotid plaque burden, since inflammation within atherosclerotic lesions increases the risk of plaque rupture and subsequent thromboembolism.54 The Mediterranean diets in the Prevención con Dieta Mediterránea (PREDIMED) study, which have been shown to be lower GI diets,55 were also found to downregulate cellular and circulating adhesion molecules and other inflammatory biomarkers.56 Since, dietary pulses are particularly low-GI foods, consuming a lower GI diet may also be beneficial for CVD risk. Our recent randomised controlled clinical trial in those with type 2 diabetes demonstrated that a low-GI diet with a particular emphasis on dietary pulses significantly lowered systolic blood pressure and heart rate, relative to a wheat fibre diet, both of which are negatively associated with CVD risk.23
Although the recent systematic review of dietary factors and CIMT by Petersen et al47 did not reveal any studies with results on dietary pulses, they did conclude from the observational studies retrieved, that greater intake of fruit, whole grains and fibre and a lower intake of saturated fat was associated with lower CIMT. From our analyses, we find support for the association between lower saturated fat intake and lower CIMT. A previous study demonstrated that for every 10 g/day (about 5% of calories) increase in saturated fat, CIMT is 0.03 mm greater.57 This is comparable to our analysis in which we found that for every 1% of total calorie increase in saturated fat, CIMT is about 0.011 mm greater (see online supplementary figure S1). The greater difference in CIMT for every 1% increase in saturated fat intake in our population compared to the previous study may be because of the higher risk of our population since they all had type 2 diabetes, were of greater age (60 vs 48 years) and greater BMI (30 vs 25 kg/m2). In recent years, new evidence from prospective studies has suggested that not all types of saturated fats play the same role in CVD development, including evidence that saturated fats from dairy products may play a protective role whereas those from other food sources may increase risk.58 ,59 Unfortunately, we were unable to explore different sources of saturated fat from our data. We did have data on protein from dairy sources which we explored post hoc and found had a significant positive association with CIMT (β=0.075, p=0.006; multivariate model). Further exploration into effects of different sources of saturated fat is warranted.
Although we did not analyse whole grains, we did find a significant negative association between dietary starch intake and CIMT. Furthermore, in the starch post hoc analyses exploring major sources of starch, dietary pulse starch and rice starch were the only significant contributors to the negative association of starch with CIMT (table 4) and since they were also highly positively correlated with each other, this may mean they are consumed together, for example, as lentils and rice, a common dish. This result further strengthens the findings for dietary pulses.
We did not find a significant association with CIMT and dietary fibre in the present analysis (β=−0.048, p=0.211). However, the recent systematic review highlighted that the PREDIMED study found a significantly lower CIMT with low (<25 g/day) versus high (>35 g/day) fibre intakes (−0.051 mm, 95% CI −0.094 to −0.009).60 When we explored dietary fibre based on intakes <25, 25–35 and >35 g/day, there was a trend for lower CIMT with increasing fibre intake, but this trend was not significant (p=0.119). Furthermore, when we adjusted for energy using the residual method, similar to the approach used in the PREDIMED study, there was again an inverse trend, although the difference between the highest and lowest fibre groups did not reach statistical significance (p=0.088) (see online supplementary table S2). Further exploration into any possible association between dietary fibre and CIMT is warranted, particularly since many studies have demonstrated an inverse association between dietary fibre intake and cardiovascular risk.61
Taken together, the results demonstrate that a higher carbohydrate diet may benefit CIMT, a marker of CVD risk. This is especially true for a diet with high-quality carbohydrate where the starch comes largely from dietary pulses, a particularly low-GI food, and which is also low in total fat, particularly saturated fat. The associations between these specific dietary variables and the metabolic profile of the participants reveal that they may act through better control of body weight, blood pressure and cholesterol.
Strengths and limitations of this study
A strength of the analyses is that the CIMT scans were all performed using the same scanner at the same site and using the same reading protocol. A further strength is the method of collection of dietary data. Although the majority of participants were overweight and may have underreported their intake,62 we took three important steps to minimise the impact of misreporting. First, we used prospectively collected 7-day food records: widely cited as the ‘gold standard’ of dietary measurement.63 Second, these records were reviewed by the study dietitian at the time of collection and in the presence of the participant and details clarified (eg, nature of the margarine). Third, for this analysis, a priori, we aimed to exclude participants reporting intakes below 500 and 800 calories or above 3500 or 4000 calories, respectively for women and men.63 No participant reported levels outside these cut-points, therefore we included all dietary records in our analyses. Finally, we have adjusted for energy in the regression models to dampen the effect of misestimation. We also found a correlation between calories and body weight (r=0.31, p<0.001; unadjusted). Therefore, we believe the dietary data are of reasonable quality. Limitations of these analyses include that they are conducted using CIMT results from only one CIMT scan obtained at baseline. However, studies have demonstrated mean max CIMT measurements to have good reproducibility, particularly using the method we adopted where measurements are made of 12 segments of the carotid artery.27 Furthermore, although CIMT has been associated with CVD5 ,6 a major limitation is that carotid plaque is a stronger predictor of CVD,64–66 although we did include posterior wall plaques in the CIMT measures, if present. Another limitation is possible residual confounding due to unmeasured or uncontrolled variables, although CIMT confounders were adjusted for in the analyses. The participants were also at high cardiovascular risk, thus application to a healthier cohort is limited. Furthermore, although at higher CVD risk, participants had relatively well-controlled diabetes (HbA1c, mean 7.1±0.5%), blood pressure (mean 122±11/72±8 mm Hg) and LDL-C (mean 2.2±0.8 mmol/L), with 67% on blood pressure medication and 72% on cholesterol-lowering medication at baseline, therefore possibly limiting the ability to assess associations between risk factors for CVD and CIMT and dietary intake, as well as limiting application to those with uncontrolled risk factors. Also, due to the good glycaemic control of the participants, this may explain why there were no associations found with either HbA1c or glucose and CIMT. Importantly, the cross-sectional design of the study is a limitation to establish causality due to the possibility of reverse causation bias. Longitudinal studies and randomised controlled trials are needed to confirm the observed associations.
Conclusion
Overall, greater consumption of dietary pulses, which are particularly low-GI foods, and available carbohydrates and lower saturated fat were significantly associated with lower baseline CIMT, as well as body weight, blood pressure and cholesterol, suggesting a potential role for diet in CVD risk reduction in type 2 diabetes. Properly designed randomised controlled trials are necessary to confirm if these dietary factors, including increased intake of dietary pulses and a reduction in saturated fat intake, are potential strategies to reduce CVD risk in those with type 2 diabetes. Furthermore, these types of trials will also be necessary to better assess if there is any effect of GI, where a low-GI diet is the result of healthy low-GI dietary advice. Thus the results of the main trial underway, which will allow for the assessment of changes resulting from a low-GI intervention, are greatly anticipated.
References
Footnotes
A version of the abstract was published in the 76th Scientific Sessions Abstract Book and the June 2016 supplement to the journal Diabetes.
Contributors DJAJ, LAL, RGJ, GEM, ARM, CWCK and JLS conceived the study and wrote the study protocol. LC, AM, CI, SM, SS-P, JC, OO, DP, RJdS, LSAA, BB, SBM, SKN, ARM and DJAJ contributed significantly to the acquisition of the data. LC, AM, CI, RGJ, SCP, GEM, ARM and DJAJ significantly contributed to the analyses of the data. LC and DJAJ drafted the manuscript and all authors revised the manuscript critically for important intellectual content. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work. DJAJ, LC, CI, RJD and SCP are the guarantors and take responsibility for the integrity of the data and the accuracy of the data analyses. The authors assume full responsibility for the accuracy and completeness of the ideas presented.
Funding This work was supported by the Canadian Institutes of Health Research (CIHR), as well as Loblaw, and Barilla. AM was supported by the Queen's University, School of Medicine JD Hatcher Summer Studentship Award. JLS was funded by a PSI Graham Farquharson Knowledge Translation Fellowship, Canadian Diabetes Association (CDA) Clinician Scientist award, CIHR INMD/CNS New Investigator Partnership Prize, and Banting & Best Diabetes Centre Sun Life Financial New Investigator Award. DJAJ was funded by the Government of Canada through the Canada Research Chair Endowment.
Disclaimer None of the funders had a role in the study design, collection, analysis or interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication. The researchers acted independently from the funders.
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare the following: LC has received research support from the Canadian Institutes of Health Research (CIHR). LC is a clinical research coordinator at Glycaemic Index Laboratories, Toronto, Ontario, Canada. RJdS is funded by a Canadian Institutes of Health Research (CIHR) Postdoctoral Fellowship Award and has received research support from the CIHR, the Calorie Control Council, the Canadian Foundation for Dietetic Research, and The Coca-Cola Company (investigator initiated, unrestricted grant). RJdS has served as an external resource person to the World Health Organization's Nutrition Guidelines Advisory Group on trans fats, saturated fats, and polyunsaturated fats. The WHO paid for his travel and accommodation to attend meetings from 2012–2016 to present and discuss this work. He has also done contract research for the Canadian Institutes of Health Research's Institute of Nutrition, Metabolism, and Diabetes, Health Canada, and the World Health Organization for which he received remuneration. He has held a grant from the Canadian Foundation for Dietetic Research as a principal investigator, and is a co-investigator on several funded team grants from Canadian Institutes of Health Research. RJdS received compensation for a lecture on dietary fat given at McMaster Pediatric Nutrition Days in 2016. LSAA has received an honorarium from the Nutrition Foundation of Italy (NFI) to co-organize a glycaemic index summit. ARM is currently consultant for Jansen/Johnson and Johnson. JLS has received research support from the Canadian Institutes of health Research (CIHR), Canadian Diabetes Association (CDA), PSI Foundation, Calorie Control Council, Banting and Best Diabetes Centre (BBDC), American Society for Nutrition (ASN), INC International Nut and Dried Fruit Council Foundation, National Dried Fruit Trade Association, The Coca-Cola Company (investigator initiated, unrestricted), Dr. Pepper Snapple Group (investigator initiated, unrestricted), and The Tate and Lyle Nutritional Research Fund at the University of Toronto. He has received speaker fees and/or honoraria from the Canadian Diabetes Association (CDA), Canadian Nutrition Society (CNS), University of Alabama at Birmingham, Dr. Pepper Snapple Group, Dairy Farmers of Canada, Nutrition Foundation of Italy (NFI), C3 Collaborating for Health, Sprim Brasil, WhiteWave Foods, Rippe Lifestyle, mdBriefcase, Alberta Milk, FoodMinds LLC, Memac Ogilvy & Mather LLC, PepsiCo, and Pulse Canada. He has ad hoc consulting arrangements with Winston & Strawn LLP, Perkins Coie LLP, and Tate & Lyle. He is a member of the European Fruit Juice Association Scientific Expert Panel. He is on the Clinical Practice Guidelines Expert Committees of the Canadian Diabetes Association (CDA), European Association for the study of Diabetes (EASD), and Canadian Cardiovascular Society (CCS), as well as an expert writing panel of the American Society for Nutrition (ASN). He serves as an unpaid scientific advisor for the Food, Nutrition, and Safety Program (FNSP) and the Technical Committee on Carbohydrates of the International Life Science Institute (ILSI) North America. He is a member of the International Carbohydrate Quality Consortium (ICQC), Executive Board Member of the Diabetes and Nutrition Study Group (DNSG) of the EASD, and Director of the Toronto 3D Knowledge Synthesis and Clinical Trials foundation. His wife is an employee of Unilever Canada. CWCK has received research grants, travel funding, consultant fees, honoraria, or has served on the scientific advisory board for Abbott Laboratories, Advanced Food Materials Network, Agriculture and Agri-Food Canada (AAFC), Almond Board of California, American Peanut Council, American Pistachio Growers, Barilla, Bayer, California Strawberry Commission, Calorie Control Council, Canadian Institutes of Health Research (CIHR), Canola Council of Canada, The Coca-Cola Company, Danone, General Mills, Hain Celestial, International Nut and Dried Fruit Council, International Tree Nut Council Nutrition Research and Education Foundation, Kellogg, Kraft, Loblaw Brands, Nutrition Foundation of Italy, Oldways Preservation Trust, Orafti, Paramount Farms, Peanut Institute, PepsiCo, Pulse Canada, Sabra Dipping Co., Saskatchewan Pulse Growers, Solae, Sun-Maid, Tate & Lyle, Unilever and White Wave Foods. He is on the Dietary Guidelines Committee for the Diabetes Nutrition Study Group of the European Association for the Study of Diabetes. DJAJ has received research grants from Saskatchewan Pulse Growers, the Agricultural Bioproducts Innovation Program through the Pulse Research Network, the Advanced Foods and Material Network, Loblaw Companies, Unilever, Barilla, the Almond Board of California, Agriculture and Agri-Food Canada, Pulse Canada, Kellogg's Company, Canada, Quaker Oats, Canada, Procter & Gamble Technical Centre ., Bayer Consumer Care, Springfield, NJ, Pepsi/Quaker, International Nut and Dried Fruit, Soy Foods Association of North America, the Coca-Cola Company (investigator initiated, unrestricted grant), Solae, Haine Celestial, the Sanitarium Company, Orafti, the International Tree Nut Council Nutrition Research and Education Foundation, the Peanut Institute, the Canola and Flax Councils of Canada, the Calorie Control Council (CCC), the CIHR, the Canada Foundation for Innovation and the Ontario Research Fund. He has been on the speaker's panel, served on the scientific advisory board and/or received travel support and/or honoraria from the Almond Board of California, Canadian Agriculture Policy Institute, Loblaw Companies, the Griffin Hospital (for the development of the NuVal scoring system, the Coca-Cola Company, EPICURE, Danone, Diet Quality Photo Navigation (DQPN), Saskatchewan Pulse Growers, Sanitarium Company, Orafti, the Almond Board of California, the American Peanut Council, the International Tree Nut Council Nutrition Research and Education Foundation, the Peanut Institute, Herbalife International, Pacific Health Laboratories, Nutritional Fundamental for Health, Barilla, Metagenics, Bayer Consumer Care, Unilever Canada and the Netherlands, Solae, Kellogg, Quaker Oats, Procter & Gamble, the Coca-Cola Company, the Griffin Hospital, Abbott Laboratories, the Canola Council of Canada, Dean Foods, the California Strawberry Commission, Haine Celestial, PepsiCo, the Alpro Foundation, Pioneer Hi-Bred International, DuPont Nutrition and Health, Spherix Consulting and WhiteWave Foods, the Advanced Foods and Material Network, the Canola and Flax Councils of Canada, the Nutritional Fundamentals for Health, AgriCulture and Agri-Food Canada, the Canadian Agri-Food Policy Institute, Pulse Canada, the Saskatchewan Pulse Growers, the Soy Foods Association of North America, the Nutrition Foundation of Italy (NFI), Nutrasource Diagnostics, the McDougall Program, the Toronto Knowledge Translation Group (St. Michael's Hospital), the Canadian College of Naturopathic Medicine, The Hospital for Sick Children, the Canadian Nutrition Society (CNS), the American Society of Nutrition (ASN), Arizona State University, Paolo Sorbini Foundation and the Institute of Nutrition, Metabolism and Diabetes. He received an honorarium from the US Department of Agriculture to present the 2013 W.O. Atwater Memorial Lecture. He received the 2013 Award for Excellence in Research from the International Nut and Dried Fruit Council. He received funding and travel support from the Canadian Society of Endocrinology and Metabolism to produce mini cases for the Canadian Diabetes Association (CDA). He is a member of the International Carbohydrate Quality Consortium (ICQC). His wife, ALJ, is a director and partner of Glycaemic Index Laboratories, and his sister received funding through a grant from the St. Michael's Hospital Foundation to develop a cookbook for one of his studies. AM, SM, SSP, JC, DP, OO, SBM, BB, SCP, LAL, RGJ and GM have no relevant conflicts of interest to declare.
Ethics approval St. Michael's Hospital ethics review board approved and provided oversight of this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests can be made to the corresponding author at nutritionproject@smh.ca.