Article Text

Abstract
Objectives Psychosocial stressors such as depression and stress, intimate partner violence (IPV) and alcohol use have been linked to preterm and small-for-gestational-age (SGA) births in general populations. The prevalence of psychosocial stressors and alcohol abuse is high in many HIV-infected (HIV+) populations. Our objective was to evaluate the effects of psychosocial stressors and alcohol abuse on birth outcomes in HIV-infected women.
Methods Antenatal depression and non-specific psychological distress, periconception IPV and alcohol consumption were measured during the second trimester among HIV+ women initiating antiretroviral treatment with efavirenz + emtricitibine + tenofovir in Cape Town, South Africa. Log binomial regression models were used to estimate the risk ratios (RR) and 95% CIs of the effects of psychosocial stressors and periconception alcohol consumption on birth outcomes: SGA (birth weight <10th centile for gestational age) and preterm (<37 weeks) births.
Results Of the 571 mother–infant pairs, 26% of women reported hazardous alcohol consumption (Alcohol Use Disorders Identification Test-C score ≥3) periconception periods, 11% reported depressive symptoms, 7% reported non-specific psychological distress and 15% reported experiencing physical or psychological IPV. 14% of infants were born preterm and 12% were SGA. Infants born to women reporting hazardous drinking were twice (adjusted RR 2.00 (95% CI 1.13 to 3.54)) as likely to be SGA compared with women reporting low alcohol intake. Alcohol consumption did not have a significant effect on the incidence of preterm birth. Depressive symptoms, non-specific psychological distress, physical and psychological IPV did not increase the risk of SGA or preterm birth significantly.
Conclusions The observed elevated risk of SGA births associated with periconception alcohol consumption underscores the urgent need to reduce alcohol consumption among women of childbearing age. Interventions targeting modifiable risk factors of adverse birth outcomes need to be integrated into HIV prevention and maternal child health programmes to improve the long-term health of HIV-exposed children.
Trial registration number NCT01933477; Pre-results.
- birth weight
- preterm
- SGA
- depression
- alcohol
- stress
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
There are few data evaluating the effects of maternal psychosocial stressors and alcohol consumption on birth outcomes of HIV-infected pregnant women.
Psychosocial stressors, alcohol consumption and birth outcomes were measured prospectively as part of a rigorously conducted randomised trial.
Maternal self-report on psychosocial stressors and alcohol consumption is amenable to measurement error.
The findings of this study will be relevant in designing interventions to reduce adverse birth outcomes in HIV-infected women but may not be generalisable to other populations.
Introduction
The burden of adverse pregnancy outcomes such as preterm and small-for-gestational-age (SGA) births is high among HIV-infected women.1 ,2 Infants born preterm and SGA face a significantly higher risk of growth faltering and mortality in childhood.3 ,4 These infants also experience the poorest neurodevelopmental outcomes.5 ,6 The high incidence of adverse pregnancy outcomes in HIV-infected women is partly attributed to HIV infection and the use of antiretroviral treatment (ART) in pregnancy to prevent mother-to-child transmission.7 ,8 To develop targeted interventions for reduction of adverse birth outcomes in HIV-infected populations, in addition to understanding the effects of ART on intrauterine growth and length of gestation, the role of classic risk factors for preterm and SGA births needs to be elucidated.
Research in the general population reported harmful effects of prenatal depression, stress, intimate partner violence (IPV) and alcohol consumption during pregnancy on birth outcomes.9–11 Alcohol passed through the placenta is known to cause oxidative stress in the developing fetus leading to growth restrictions.12 Depression, stress and IPV can directly increase adverse birth outcomes by dysregulation of the hypothalamic–pituitary–adrenocortical axis, increasing levels of stress hormones which cause placental hypoperfusion leading to growth restriction and shortening of gestational age.13 ,14 Antenatal depression, stress and IPV can also influence birth outcomes indirectly via poor nutrition, hygiene and healthcare seeking (figure 1).15 ,16

Hypothesised direct and indirect pathways of effects of maternal mental health stressors on birth outcomes. (Figure drawn based on mechanisms described by Diego et al,13 Wadhwa et al,14 Neggers et al15 and Zuckerman et al16). ART, antiretroviral treatment; IPV, intimate partner violence; SGA, small for gestational age.
Recent studies in HIV-infected populations reported antenatal depression and stress to be associated with poor adherence to ART, and poor HIV-related clinical, immunologic and virologic outcomes, which can potentially increase the incidence of adverse pregnancy outcomes.17–20 Although the prevalence of psychosocial stressors and alcohol abuse is high in many HIV-infected populations,21–23 their effects on birth outcomes have not yet been studied. In the present study, we examined the association of antenatal depression, non-specific psychological distress, IPV and alcohol abuse with preterm and SGA births in a cohort of HIV-infected pregnant women, the majority of whom initiated ART under the Option B+ guidelines in South Africa.
Methods
This prospective cohort study is part of the larger Maternal and Child Health (MCH)-ART study, an ongoing trial evaluating optimal strategies for providing ART services during the postpartum period.24 From March 2013 to June 2014, a cohort of 628 HIV-positive (HIV+) pregnant women were enrolled from the Gugulethu Midwife Obstetric Unit (MOU) in Cape Town, South Africa, and attended up to three antenatal study visits. Pregnant women, aged 18 years or older, were recruited in the parent study if they were eligible to initiate ART with efavirenz + emtricitibine + tenofovir based on the current national guidelines. Until June 2013, ART eligibility was assessed based on CD4 cell count or clinical staging. After June 2013, all women were considered eligible for lifelong ART irrespective of their CD4 cell count or clinical stage (Option B+). Women were eligible to participate in the study if they planned to stay in the city until delivery and during the postpartum period.
Women received clinical care during pregnancy through routine HIV services delivered by the clinic staff at the MOU. Data and blood samples for research were collected by study staff at study visits separate from routine care. Information on socio-demographic characteristics, and blood samples to measure CD4 count, viral load and haemoglobin level were collected at the first antenatal visit. At all antenatal visits, a nurse midwife collected information on medical and obstetric history and conducted physical examinations. Data on maternal psychosocial stressors: depression, non-specific psychological distress, IPV and alcohol consumption were collected at the first antenatal study visit following enrolment. Birth weight was measured by the nurse midwife attending women at delivery and was abstracted from medical records by research staff. Gestational age was calculated based on ultrasonogram assessments, except for a few subjects (1%) for whom reported date of last menstrual period at first antenatal visit was used.
Using the recently published Intergrowth-21st standard,25 newborns were grouped based on their weight for gestational age into SGA and appropriate for gestational age (AGA). SGA was defined as birth weight <10th centile for gestational age; AGA was defined as birth weight ≥10th centile for gestational age. Preterm birth was defined as birth before 37 completed weeks.
Depressive symptoms during the week preceding the interview were measured with the Edinburgh Postnatal Depression Scale (EPDS).26 The 10-item questionnaire was summed to a continuous score where higher scores indicated greater frequency of depressive symptoms. A dichotomous depression symptoms (probable and major) variable was defined as EPDS score ≥13. The Kessler-10 scale (K-10) was used to measure non-specific psychological distress during the month preceding the interview.27 A continuous K-10 score was calculated by summing individual-item responses such that a higher score indicated greater frequency of symptoms of psychological distress. Ordinal categories of the K-10 scores were used to define well (<20), mild (20–24), moderate (25–29) and severe (≥30) psychological distress. Alcohol consumption during the year preceding pregnancy recognition was assessed using the Alcohol Use Disorders Identification Test (AUDIT).28 Alcohol consumption during pregnancy was assessed using a later AUDIT administered in the third trimester. AUDIT-C scores were calculated by summing individual item responses across the first three AUDIT items, where higher scores indicate more problematic alcohol use. Hazardous alcohol consumption was defined as AUDIT-C score ≥3.29 Information on IPV during the year preceding pregnancy recognition was collected using the violence against women (VAW) tool developed by the WHO.30
We used log binomial regression models to estimate the risk ratios (RR) and 95% CIs of the effects of maternal stressors on adverse pregnancy outcomes.31 Estimates of the effects of each stressor on SGA and preterm birth were obtained from separate models. To control for confounding, multivariable models were adjusted for socioeconomic status, maternal age, height, haemoglobin level, parity, CD4 cell count and HIV RNA viral load at study entry. We used missing indicator terms in the multivariate models for covariates with missing data.32 All statistical analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
All mothers provided written informed consent to enrol themselves and their infants in the study. The trial was registered at ClinicalTrials.gov as NCT01933477.
Results
Of the 628 women enrolled in the study, data were available on 601 live births and a total of 571 birth outcomes were included in the analyses. We excluded 10 infants (1.7%) due to missing birth weight data, 5 (1%) due to missing gestational age data, 14 (2.3%) due to missing gender data and 1 infant with implausible gestational age and birth weight combinations.
Table 1 shows the maternal characteristics at study entry. The mean age of pregnant women was 28 years and the majority (82%) had had at least one prior pregnancy and 40% were married or cohabiting at study enrolment. About 26% of the mothers had completed secondary education and 38% were employed. More than half of the pregnant women had viral load <3 log10 copies/mL and about 47% had a CD4 cell count >350 cells/µL at enrolment. The majority (73%) of the pregnant women initiated ART under Option B+ guidelines at a median gestational age of 21 weeks (IQR 16–26 weeks). Between study enrolment and the first postpartum visit, 70% of the women reported no missed doses of ART and the majority (26%) of the remaining women reported up to three missed doses of ART per month.
Characteristics of study participants at enrolment (N=571)
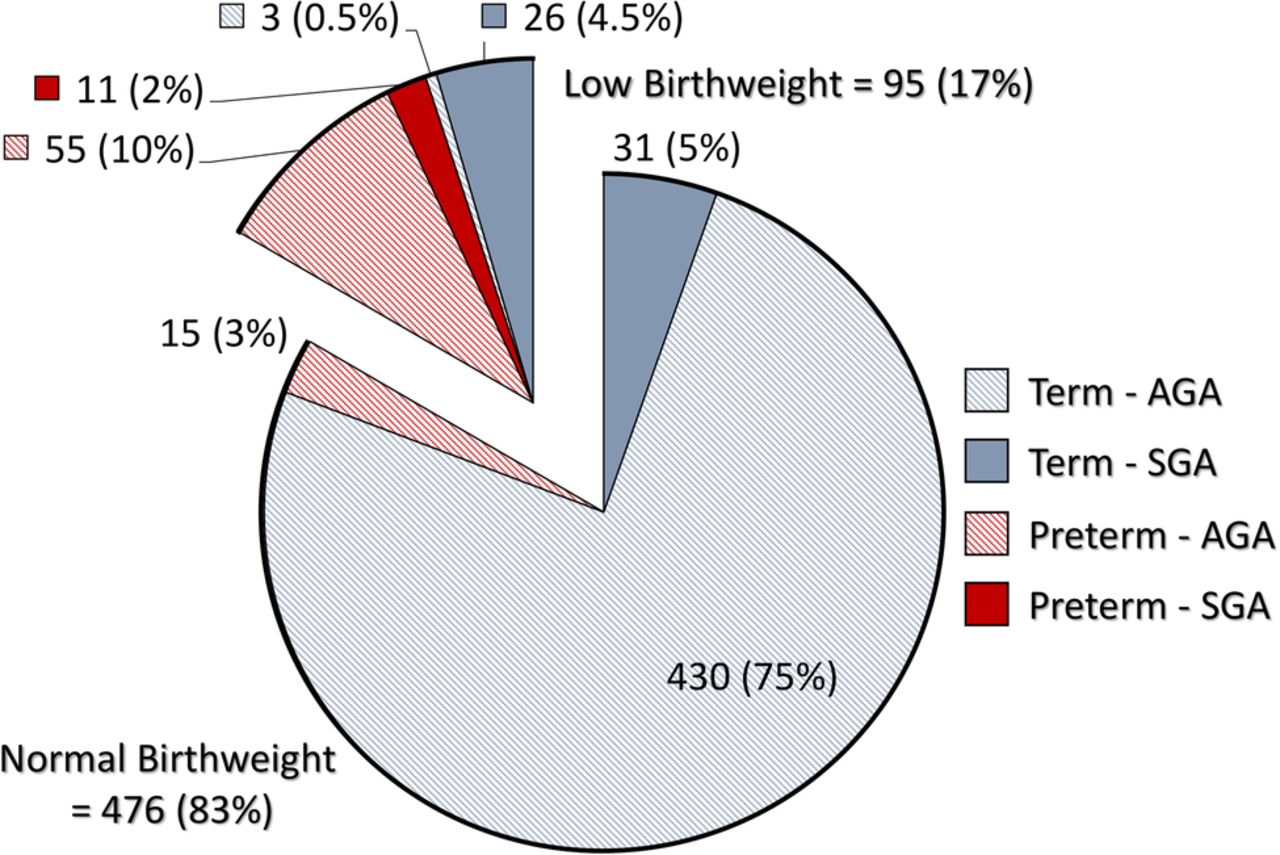
Of the 571 infants included in the analyses, 81 (14%) were preterm and 68 (12%) were SGA (table 1). Seventeen per cent (95) of the infants were born with low birth weight (LBW) (<2500 g). Of this group, the majority (55, 10% of total) were preterm-AGA and 26 (4.5% of total) were term-SGA. Of the 430 (75%) normal birthweight infants, 3% were preterm-AGA and 5% were term-SGA (figure 2).

Distribution of preterm and SGA in low birthweight and normal birthweight infants. AGA, appropriate for gestational age; SGA, small for gestational age.
Figure 3 shows the prevalence of psychosocial stressors experienced by the pregnant women included in our study. More than a quarter of the women (26%) reported hazardous alcohol drinking during the year prior to pregnancy recognition. Of them, the majority (65%) reported having ≥5 standard drinks/day and 32% reported having ≥3 standard drinks/day (data not shown). Fewer women (9%) reported hazardous alcohol consumption in a third trimester interview which asked about alcohol consumption following recognition of pregnancy (data not shown). On the basis of the EPDS scale, 62 women (11%) had reported depressive symptoms (probable and major) during the preceding week; of them, 7% had symptoms consistent with major depression. Only 7% of the pregnant women reported non-specific psychological distress (mild, moderate and severe) during the preceding month on the K-10 scale. About 15% of the pregnant women reported having experienced physical or psychological IPV and 2% reported having experienced sexual IPV during the year prior to pregnancy recognition.

{kind=link}
{kind=link}
{kind=link}
Prevalence of psychosocial stressors and alcohol consumption in study population.
The RRs for SGA and preterm birth are given in table 2. Infants born to pregnant women who reported hazardous drinking were twice as likely to be SGA compared with women reporting low alcohol intake in the periconception period (adjusted RR 2.00 (95% CI 1.13 to 3.54)). Hazardous alcohol drinking did not increase the incidence of preterm birth (adjusted RR 0.89 (95% CI 0.51 to 1.53)). Women reporting hazardous drinking during pregnancy assessed in the third trimester also experienced elevated risk of SGA (adjusted RR 1.62 (95% CI 0.68 to 3.84)) and preterm birth (adjusted RR 1.13 (95% CI 0.48 to 2.65)) but these risk elevations were not statistically significant (see online supplementary table S1).
Crude and adjusted estimates of effect of psychosocial factors and alcohol use on small-for-gestational-age (SGA) and preterm births
supplementary table
Crude and adjusted estimates of effect of intimate partner violence and alcohol use on SGA and preterm births. (exposures measured during third trimester)
Compared with pregnant women reporting no depressive symptoms, women reporting depressive symptoms in the second trimester had a risk ratio of 1.52 (95% CI 0.70 to 3.29) for SGA birth. Depressive symptoms in the second trimester also did not increase the incidence of preterm birth. Women reporting non-specific psychological distress on the K-10 scale were not at a higher risk of delivering an SGA baby. A statistically non-significant elevation of risk of preterm birth was observed among women reporting moderate distress. A small statistically non-significant elevation of risk of SGA was observed among women reporting physical and psychological IPV in the year preceding pregnancy recognition.
Discussion
Our study evaluated the associations of maternal psychosocial stressors and alcohol abuse with preterm and SGA births among infants born to HIV-infected pregnant women initiating ART, in a semiurban South African setting with high prevalence of alcohol use and moderate prevalence of mental health stressors.33 ,34 Pregnant women in our study experienced a high incidence of preterm and moderate incidence of SGA births. We noted a twofold increase in the risk of SGA births among women reporting hazardous alcohol use during the periconception period. We did not observe any significantly increased risk of preterm and SGA births associated with maternal psychosocial stressors.
Our study sample had a lower incidence of SGA (12 vs 23%) and a higher incidence of preterm births, <37 weeks (14 vs 8%) compared with the national average for South Africa.35 Low incidence of SGA in a population with high incidence of preterm births is expected. Since the period of rapid intrauterine growth is cut short for preterm infants, they are less likely to be growth restricted and diagnosed SGA using a conventional birth weight standard.36 The high preterm rate in our study population has been found to be associated with HIV infection but not with the timing or duration of ART use during pregnancy.37 Pregnant women in our study did not receive any protease inhibitor as part of their ART regimen which has been consistently linked with elevated risk of preterm birth in previous studies.38 ,39
Our observation that psychosocial stressors do not increase preterm and SGA births conforms with several prior studies reporting no effects of psychosocial stressors on adverse birth outcomes.40 The majority of the studies that demonstrated significant effects reported negative effects of depression and IPV on SGA and negative effects of stress on preterm births.41 ,42 Due to the low incidence of SGA in our study population, our analyses may have been underpowered to detect any small effects of stressors on SGA. In addition, our study sample was part of an intervention study, and thus may have more homogeneous healthcare utilisation and adherence to ART during pregnancy. Owing to the homogeneity of the potential mediating factors, we may not have observed effects of stressors on birth outcomes via the indirect pathway (figure 1). A meta-analysis of studies of effects of depression on LBW and preterm births found significant effects in the studies conducted in low-income countries and among women from low socioeconomic background in developed countries.10 This observation supports the hypothesis that the negative effects of depression and other mental health stressors reported in prior studies are primarily mediated via indirect pathways. The reported negative effects in some studies may also be confounded to some degree as women from low socioeconomic conditions are prone to experiencing depressive symptoms, stress and IPV.40 ,43 Although the potential for residual confounding remains in observational studies, biases in our estimates are likely to be minimal, as they are adjusted for the known confounders including socioeconomic status.
Our observation of significant negative effects of periconception alcohol consumption on incidence of SGA births and no effect on incidence of preterm birth is in agreement with reports from developed countries44 with a few exceptions which reported protective effects of mild to moderate prenatal alcohol consumption on preterm birth.45 ,46 While the harmful role of alcohol consumption in pregnancy on fetal growth and the nervous system is well documented, data on the effects of periconception consumption is limited.47 ,48 Periconception alcohol consumption was demonstrated to be sufficient to programme growth restriction in late gestation and changes in placental structure in animal studies.49 A recent study conducted among a cohort of British women reported significant negative effects of periconception alcohol consumption on continuous birth weight centiles,50 which together with our findings on periconception consumption suggest that although many women modify their consumption behaviour following pregnancy recognition, the consequences of prior consumption may be persistent and irreversible. In places with a high prevalence of alcohol abuse and unplanned pregnancies (70% in our study population), the relatively small effect size observed magnified by a large number of pregnant women abusing alcohol can have considerable implications for the health of HIV-exposed uninfected infants via SGA births.
Our estimates for the effects of periconception alcohol consumption on SGA and preterm births may be an underestimate due to the measurement error introduced by the long exposure-measurement window (1 year preceding pregnancy recognition) and also the choice of reference category for the analyses. We chose women with AUDIT-C score <3 as the reference category in our analyses which included women reporting low alcohol consumption. We were not able to account for the variability in type of alcohol consumed, as the AUDIT does not include questions on alcohol type. We may have introduced selection bias as we excluded infants with missing gestational age, birth weight and gender data, leading to an underestimate of the true effect sizes for all exposure categories. Since the frequencies of outcome were small in subgroups, we were unable to stratify the analyses by LBW and estimate the exposure effects among infants who were preterm and SGA. Also, we could not assess effect modification by maternal HIV status, as we did not have comparable data from HIV-negative pregnant women. Our study population has a high participation rate (1% of eligible women refused after screening), which originates from a poverty-stricken township of Cape Town with a high burden of HIV. While the findings of our study are relevant in designing interventions to reduce adverse birth outcomes in many similar HIV-infected populations, these results may not be generalisable to other populations.
Our study is the first to evaluate the effects of maternal psychosocial stressors and alcohol consumption on birth outcomes of HIV-infected pregnant women using detailed and prospectively collected data. A large body of evidence supports that depression, stress and IPV affect the mother's ability to care for herself which has detrimental effects on the physical and mental development of infants.9 ,51–53 Although we did not observe any significant effects of maternal psychosocial stressors on birth outcomes, it is still important to screen and treat women for these conditions. Our finding on the effects of periconception alcohol consumption underscores the urgent need to reduce alcohol consumption among women of childbearing age. While efforts to prevent infant HIV infections have been increasingly successful, the high prevalence of adverse birth outcomes continues to threaten the health of the HIV-exposed children. Interventions targeting modifiable risk factors such as alcohol consumption incorporated into existing HIV prevention initiatives and maternal child health programmes are needed to further improve the survival and development potentials of these children.
Acknowledgments
We thank the mothers and infants, as well as the field research team including nurses, midwives, supervisors and laboratory personnel, who made this study possible.
References
Footnotes
Contributors AS conceptualised and conducted the data analysis, interpreted the results and wrote the first draft of the manuscript. EJA and LM are the principal investigators of the parent trial and contributed to the study design, implementation, analysis and interpretation of the data. KB and TKP participated in study implementation and data collection, contributed in data analysis and data interpretation and provided critical inputs on the manuscript. AZ and AR participated in the study implementation and supervision of data collection. All authors read and approved the final manuscript.
Funding This research was supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through the National Institute of Child Health and Human Development (NICHD), grant number 1R01HD074558. Additional funding comes from the Elizabeth Glaser Pediatric AIDS Foundation. AS was supported by the National Institute of Allergy & Infectious Diseases of the National Institutes of Health under award number T32AI114398.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Human Research Ethics Committee of the University of Cape Town, Faculty of Health Sciences and the Columbia University Medical Centre Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.