Article Text

Abstract
Objective Describe and assess the impact of a pharmacist-led patient review programme on the management and control of type 2 diabetes (T2D).
Design Uncontrolled prospective cohort study with before and after intervention data collection.
Setting General practices within NHS Slough Clinical Commissioning Group (CCG).
Participants 5910 patients with T2D.
Interventions Pharmacists reviewed 5910 patients and worked with general practice teams to schedule any of the 9 key care processes recommended by the National Institute for Health and Care Excellence (NICE) that the patients were lacking, to optimise medication and to make other interventions such as providing lifestyle advice.
Main outcome measures The proportion of patients receiving the NICE-recommended 9 key care processes and proportion of patients whose glycated haemoglobin (HbA1c), blood pressure (BP) or total cholesterol (TC) readings were over target before and after the intervention period.
Results The proportion of patients receiving all of the NICE-recommended 9 key care processes increased from 46% at project outset in April 2013 to 58% on completion in April 2014 and the percentage of patients achieving HbA1c, BP and TC targets all increased (65% to 70%, 70% to 76%, 78% to 82%, respectively). Quality Outcomes Framework (QOF) data for Slough CCG showed the percentage of diabetic patients achieving target HbA1c, BP and TC readings increased from April 2013 to April 2014, but then diminished in the year after project completion.
Conclusions The pharmacist-led review increased the number of key care processes administered and improved diabetic control during the year of programme delivery. The improvement abated during the year after, suggesting that such programmes should be ongoing rather than fixed term. The programme combined the strategic drive and project facilitation skills of Slough CCG, the general practice teams' knowledge of their patients and the clinical and information technology skills of an experienced pharmacist team.
- diabetes
- pharmacist
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
An example of effective multidisciplinary team working, this project was able to deliver improved focus on type 2 diabetes (T2D) management in NHS Slough Clinical Commissioning Group (CCG) by combining the strategic drive and project facilitation skills of the CCG, the general practice teams' drive to deliver ever higher standards of service to their patients and the clinical and information technology system expertise of an experienced pharmacist team.
This project represents a good example of the aspirations of the joint working initiatives created by the Royal College of General Physicians and the Royal Pharmaceutical Society in order to identify areas where general practitioners and pharmacists can work together to improve the quality of patient care.
The key limitation when evaluating the outcomes of this project is that it represented just one element of the overall package of care received by the patients. However, within the outcomes reported, the increase in the number of patients receiving all nine of the NICE-recommended nine key care processes (from 48% to 58% of patients) can be more clearly attributed to the project, as the lists of missing care processes per each patient were generated by the pharmacists and then systematically worked through by the general practice teams.
While a clinical programme such as this carries associated financial costs, it is widely accepted that the financial costs of managing poorly controlled T2D patients (and the associated complications) far exceed the costs of managing well-controlled T2D patients.
Introduction
People in England can receive healthcare provided free at the point of delivery by the government-funded National Health Service (NHS). Patients register with a general practitioner (GP) practice which comprises of at least one GP and a wider team of healthcare professionals and administrative staff. Every GP practice (Practice) in England is a member of 1 of more than 200 Clinical Commissioning Groups (CCGs). CCGs are clinically led statutory bodies responsible for the planning and commissioning of healthcare services that meet the needs of the local population. Their success is measured by how much they improve health outcomes.
Type 2 diabetes (T2D) is a complex condition to manage. When T2D is not well managed, it is associated with considerable morbidity and serious complications, including heart disease, stroke, diabetic retinopathy, kidney disease and amputation—over time leading to disability and premature mortality.1 In addition to the clinical burden of T2D care, there are also substantial financial costs associated with it.1 Since 1996, the number of people diagnosed with diabetes in the UK has increased from 1.4 million to 2.9 million, and by 2025, it is estimated that there will be 5 million people with diabetes in the UK.2 To add to the growing burden of diabetes, an estimated 850 000 people in the UK are currently living with undiagnosed T2D and in diagnosed patients, by the time of diagnosis, ∼50% of T2D patients show signs of complications.2 Around £10 billion (or 10%) of the NHS budget is spent on diabetes. The total cost (direct care and indirect costs) associated with diabetes in the UK currently stands at £23.7 billion and is predicted to rise to £39.8 billion by 2035/2036.2
The prevalence of (diagnosed) T2D in NHS Slough CCG is higher than the national average and is increasing. According to the National Diabetes Audit 2012/2013, which was published during the project year, only a minority (40.0%) of T2D patients in NHS Slough CCG achieved all treatment targets recommended by the National Institute for Health and Clinical Excellence (NICE).3 This was consistent with the national picture. With too few patients achieving all treatment targets, the need for improvement was key to delivering better patient care.
The nine key care process that NICE recommends that each patient with diabetes should receive each year are:
Glycated haemoglobin (HbA1c) measurement, with a suggested target of 59 mmol/mol.
Blood pressure (BP) measurement, with a suggested target of 140/80 mm Hg.
Cholesterol level measurement, with a suggested target for total cholesterol (TC) of 5 mmol/L.
Retinal screening.
Foot checks.
Urinary albumin testing.
Serum creatinine testing.
Weight check.
Smoking status check.
Given the local picture regarding the quality of T2D management and the future projections of a substantial increase in T2D prevalence, NHS Slough CCG identified the improved management of T2D as a key strategic priority.4 Recently published studies demonstrate that pharmacist support can improve the safety of prescribing, improve the quality of care for long-term conditions and reduce readmissions rates.5–9 Within the UK, there is currently a policy drive to use clinical pharmacists more effectively in primary care.6
Based on this and with a need to deliver improvements in patient outcomes, NHS Slough CCG commissioned the services of an experienced clinical pharmacist team. Each pharmacist would become part of the general practice team at each site for the duration of the programme. Much of the published data on pharmacist intervention to improve the care for people with T2D are based on pharmacists working in Community Pharmacies or clinics rather than being integrated into general practice teams.10
Methods
Led by a senior pharmacist and a team of three clinical pharmacists, the clinical programme was delivered between April 2013 and April 2014. To ensure a high level of continuity within the work delivered, each of the 13 GP practices participating in the programme was assigned to 1 of the 3 clinical pharmacists, who worked with the same GP practices throughout the year. The programme consisted of three phases.
The first phase of the project involved data collection, analysis and work-stream prioritisation. The aim of this phase was to benchmark current achievements within T2D (and comorbidities) management, to engage with general practice teams and to allow the pharmacists to prioritise patient cohorts for review in line with relevant NICE and local guidance. Software was created to execute identical information searches on the clinical systems at each Practice at each phase of the project. Each practice gave permission for anonymised summary statistics from each phase of the project to be reported back to NHS Slough CCG. No patient-identifiable data were removed from each Practice. Key activities at phase I of the project included:
Identification of patients who were missing any of the NICE-recommended nine key care processes,
Referral of patients to receive any missing or outdated care processes,
Identification of patients for further review where HbA1c, BP and TC targets not achieved,
Educational sessions for practice personnel in optimising T2D management and control.
Following the analysis of practice performance in relation to the NICE-recommended nine key care processes in the financial year prior to project initiation in April 2013, the findings were discussed with key personnel within each GP practice. A tailored strategy to increase the percentage of patients receiving all of the NICE-recommended nine key care processes was designed and agreed with each Practice.
The second phase of the programme was designed to optimise treatment for those patients identified in phase I as having failed to achieve their HbA1c, BP and TC targets. The data from phase I combined with a detailed clinical review of each poorly controlled patient enabled the pharmacists to make recommendations to enhance treatment where appropriate. Recommendations for each individual patient were discussed at a multidisciplinary team meeting including the GP who was the project lead at each Practice, who then decided the most appropriate course of action to take with each patient. Recommendations made included but were not limited to drug initiations, dose changes, drug discontinuations, interventions regarding adherence to and persistence with treatment, lifestyle and diet advice, and referring to specialist care where complications were identified.
Each practice decided how different recommendations should be actioned. In some instances, the GP opted to action recommendations opportunistically when patients attended. However, recommendations were usually actioned proactively using a mix of clinic consultations, telephone consultations and letters to patients. Delivery of the agreed interventions was generally shared out between the general practice team and the pharmacist.
During phase III of the programme, each Practice received a follow-up visit from the pharmacist at 6 and 12 months post-phase II in order to evaluate the impact of interventions made during phases I and II. The aim of these visits was to assess the extent to which agreed recommendations had been implemented, to implement any outstanding actions, to identify further opportunities for improvement through reaudit and to maintain practice engagement in the project.
Results
During phase I, the pharmacist team identified 3211 patients missing at least 1 of the NICE-recommended 9 key care processes. A plan was agreed with each practice to ensure that the missing care processes were completed with each patient wherever possible.
Figure 1 shows that the proportion of patients receiving all of the NICE-recommended nine key care processes was increased from 46% at the beginning of the project to 58% at the end of the project, and that the proportion of patients receiving less than seven of the nine key care processes reduced from 21% to 15%.

NICE-recommended nine key care processes: achievement before and after project delivery.
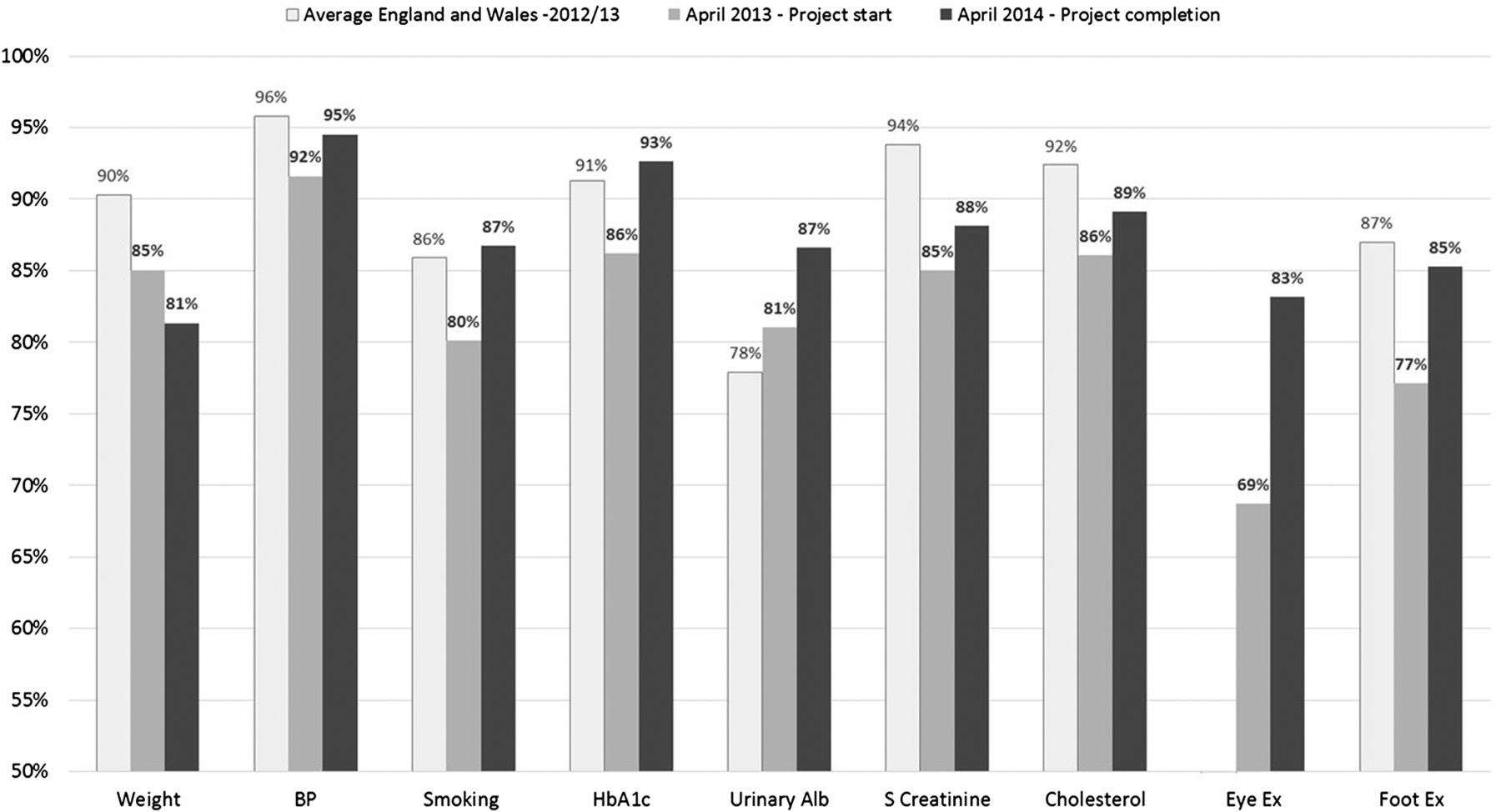
Figure 2 shows that in April 2013 at the project outset, the percentage of patients completing seven of the nine care processes (weight, BP, smoking status, HbA1c, serum creatinine, TC and foot examination) was below the England and Wales average. Only the percentage of patients with urinary albumin assessment was above the England and Wales average. Comparative data relating to eye examinations were not available. In April 2014, after the clinical programme was completed, the percentage of patients who had received eight of the nine care processes had improved in comparison to the previous year. In all except for the assessment of weight, there was an increase in the proportion of patients recorded as receiving each individual care process from project start to project completion (figure 2).
{kind=link}
{kind=link}
Achievement of the NICE-recommended nine key care processes before and after project delivery and against the 2012/2013 average for England and Wales:3 weight, blood pressure, smoking status, glycated haemoglobin, urinary albumin, serum creatinine, total cholesterol, eye check and foot check.
During phase I of the project, a total of 2984 of the 5910 patients were found by the pharmacist team to be at risk of poor T2D control as defined by their latest HbA1c, BP or TC readings being over the NICE recommended target. However, some readings were over 1-year-old, and where this was the case, the pharmacists worked with the Practices to try to arrange new tests. This was often achieved but at times not until late into the project, meaning that there were fewer actions or recommendations that the pharmacist could make for such patients within the project timeframe. Such patients had to be flagged for more detailed review by the Practice team on completion of out-of-date care processes.
The pharmacists were able to undertake a more detailed review of the notes of each patient whose latest overtarget HbA1c, BP or TC readings were less than a year old. Recommendations were made to the GP as to how treatment could be optimised for each such patient. In addition to arranging for these patients to have any missing care processes put in place as previously described, there were 1035 patients for whom opportunities to optimise medication were recommended to the GP.
Table 1 shows the number and proportion of patients whose latest HbA1c, BP or TC readings were overtarget at the start versus the end of the project. It can be seen that by the end of the project, a greater proportion of the population had an HbA1c, BP and/or TC reading in their record, and a lower percentage of the readings were overtarget.
Number and percentage of patients with glycated haemoglobin, blood pressure or total cholesterol readings at project start and end
The way that the project was designed meant that only those patients with an overtarget HbA1c, BP or TC reading taken within 12 months of project initiation were able to receive the most detailed review from the pharmacist team. Table 2 shows the number of patients with an overtarget HbA1c, BP or TC reading taken within 12 months of project initiation, who then had a further reading taken after they had been extensively reviewed by the pharmacist in collaboration with the GP at each practice.
Number of patients with up to date, overtarget glycated haemoglobin, blood pressure or total cholesterol readings at project outset, whose readings were repeated after project phase I
Table 3 contains data relating to the percentage of all diabetic patients across NHS Slough CCG whose HbA1c, BP and TC were overtarget in the financial year ending prior to project delivery starting (April 2013), at the financial year end which coincided with the completion of project delivery (April 2014) and at the financial year end 1 year after project delivery had completed (April 2015). These data were reported by practices via the Quality Outcomes Framework (QOF) reporting process.11
Quality Outcomes Framework data for NHS Slough Clinical Commissioning Group11
Table 3 shows that the percentage of patients whose HbA1c, BP and TC readings were overtarget were at their lowest levels on completion of the project before increasing again in the year after project delivery had completed.
Limitations and discussion
This pharmacist-led review programme of patients with T2D showed an increase in the percentage of patients who had all of the nine NICE-recommended nine key care processes completed and a decrease in the number of patients considered to be poorly controlled. This adds to the evidence for improvements in outcomes in T2D when pharmacists are involved.8 ,10
The findings of this study are distinguishable from much of the data previously published because the pharmacists involved were integrated into already existing general practice teams, which is the model currently being proposed by the Royal College of General Physicians and the Royal Pharmaceutical Society.5 The pharmacists were acting as clinicians, making patient-specific recommendations. They also used information technology (IT) skills to interrogate electronic medical records to identify the individuals with T2DM who were at greatest risk of complications and target the work of different members of the general practice team. This meant that resource was appropriately attributed to each patient based on need and based on the skills of each member of the team. Such an approach would be widely replicable because it does not require significant changes to patient pathways or the development of new providers but simply the inclusion of a new staff member with a different skill set into an already existing team.
The key limitation when evaluating the outcomes of this project is that it represented just one element of the overall package of care received by the patients between April 2013 and April 2014. It is therefore not possible to say exactly how many of the patients whose HbA1c, BP or TC levels came back into target range were as a direct result of the problem identification and the interventions delivered within this project, and how many would have come back into range if the project had not taken place. Potential confounding factors that were not controlled for include: local clinicians receiving training on the management of T2D from other sources, the marketing and subsequent prescribing of new treatments for T2D or improvements or changes to other commissioned services for T2D locally.
What is known is that a proportion of those patients who were well controlled at the project outset, or who appeared after the project outset, failed to achieve at least one of the HbA1c, BP or TC targets during the year of project delivery, because while tables 1 and 3 show a reduction in the proportion of poorly controlled patients across the CCG as a whole during the project delivery year, the reductions are not on the scale of those observed in the most extensively reviewed cohort of patients which were tracked in table 2.
Table 2 shows that where patients underwent a detailed review by the pharmacist in collaboration with the Practice team, 29–45.5% of their markers of poor control at project outset improved to the point of achieving target by the end of the project, yet table 1 shows that the overall numbers of patients whose latest reading were still overtarget at the end of the project had not reduced by the same proportions. There were three main reasons for this:
Because of the progressive nature of T2D when poorly managed, many patients whose T2D was well controlled at the project outset had become poorly controlled during the year of project delivery.
Some patients had outdated readings at the project outset which indicated good T2D control but which were updated during the course of project delivery and on occasion revealed that control had diminished.
The T2D population under review increased from 5910 to 6134 during the project year, bringing with it a proportion of patients with overtarget readings.
An analysis of QOF data (a national database, independent of this study) relating to time periods before, during and after project delivery was undertaken and is shown in table 3. Within the overall NHS Slough CCG population, the proportion of patients above the recommended targets for HbA1c, BP and TC were lower for all three parameters at the point of project completion than they had been in the QOF year preceding project delivery. The likelihood that this improvement was at least partially attributable to the project was perhaps further reinforced by the fact that the percentage of patients exceeding each of the three parameters once again increased in the year following project completion. This also suggests that a rolling programme would be more beneficial than a fixed term project, and emphasises the importance of building a strong educational legacy with the Practices so that they can continue to deliver a similar programme.
The increase in the percentage of patients receiving all nine of the NICE-recommended nine key care processes (from 48% to 58% of patients) can be more clearly attributed to the project, as the lists of missing care processes per each patient were generated by the pharmacists and then systematically worked through by the practices.
However difficult it is to isolate the impact of this ‘real life’ clinical programme, it did succeed in identifying and focusing attention and resource on the poorly controlled T2D patients within NHS Slough CCG between April 2013 and April 2014. Missing care processes were completed for those patients, who were also recommended for priority review by their practices with a host of treatment optimisation recommendations suggested by the pharmacists. Going forward, NHS Slough CCG is targeting further improvements in T2D control, and the learning and outcomes from this programme give confidence that improved outcomes could be achieved again, but that more consideration should be given as to how practices might be able to routinely incorporate more of the patient identification, monitoring and tracking into their day-to-day activities in order to derive more of a legacy effect if the service cannot be provided every year.
As an example of effective multidisciplinary team working, this programme was able to deliver improved focus on T2D management in NHS Slough CCG by combining the strategic drive and project facilitation skills of the CCG, the practices' drive to deliver ever higher standards of service to their patients and the clinical and IT system expertise of an experienced pharmacist team. It represents a good example of the aspirations of the joint working initiatives created by the Royal College of General Physicians and the Royal Pharmaceutical Society to identify areas where GPs and pharmacists can work together to improve patient care.5
While a clinical programme such as this carries associated financial costs, it is widely accepted that the financial costs of managing poorly controlled T2D patients (and the associated complications) far exceed the costs of managing well-controlled T2D patients.1 Therefore, a relatively modest investment in a clinical programme such as this may help to ensure that the NICE-recommended key care processes are completed, monitored and acted on in order to reduce morbidity, mortality and healthcare costs, while also improving Practice and CCG performance against the QOF.11
Footnotes
Contributors As the guarantor, TL conceived the study. AB and JG-D managed the data collection and presentation, while TL and NN monitored the conduct of the study and provided clinical interpretation and analysis of the results.
Funding It was conducted as an observational analysis of a pharmacist-led clinic programme which was funded by NHS Slough CCG and delivered in partnership with Interface Clinical Services, an independent clinical services provider.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.