Article Text

Abstract
Introduction Although premature infants and their parents are discharged earlier to inhomecare programmes, how to optimally support parents during this transition remains unknown. The aim of this study is to compare the effects of early inhomecare (PreHomeCare) including video consultations and mobile applications with those of inhospital consultations regarding breast feeding, parental confidence and parent–infant interactions.
Methods and analysis A randomised controlled intervention study will be conducted in four neonatal departments offering PreHomeCare (ie, premature infant inhomecare) in Denmark. Parents of hospitalised premature infants who fulfil the inclusion criteria for PreHomeCare will be randomised during hospitalisation to either the intervention (n=80) or control group (n=80) using 1:1 block randomisation. During PreHomeCare, the intervention group will receive a smartphone application with a video system and an infant scale, and the control group will receive usual care (ie, hospital consultations). Additionally, both groups will have planned nurse consultations two to three times a week: the intervention group through video consultations and the control group through inhospital consultations. Data collection will occur at inclusion/baseline, at the end of PreHomeCare and 1 month after discharge using questionnaires and hospital records. The primary outcome is the proportion of exclusively breastfed infants 1 month after discharge/end of PreHomeCare, the secondary outcomes are parent–infant interactions measured by the Mother and baby interaction scale and family confidence in caring for infants measured by the Karitane Parenting Confidence Scale. The process evaluation will consist of two qualitative studies: a field study and an interview study. Data collection will initially involve field observations of three scheduled video consultations with six families from the intervention group. These families will also be interviewed 1 month after PreHomeCare has ended.
Ethics and dissemination The project has been approved by the Regional Ethics Committee and the Danish Data Protection Agency.
Trial registration number NCT02581800.
- Early in-homecare
- Breast feeding
- Premature infant
- early discharge
- parent/infant relation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Preterm birth rates have been increasing in almost all countries worldwide,1 and ∼15 million infants around the world are born prematurely each year. Premature birth is defined as a delivery that occurs before a gestation age (GA) of 37 weeks.2 In Denmark, ∼6.4% of all live infants are born prematurely.3 Premature infants are characterised by organ underdevelopment, which increases the need for treatment associated with breathing, circulatory and gastrointestinal function, temperature regulation and infections; in most cases, these needs require admission to the neonatal ward.2 While health professionals care for the infant (depending on the severity of the infants' condition), parents often experience anxiety, depression, decreased parenting confidence and self-efficacy and impaired parent–child interactions related to feelings resulting from the premature infant's condition.4 Parental anxiety related to uncertainty about their infant's health has been shown to affect infant development and growth and perceptions of future infant vulnerability.4 Furthermore, parental anxiety seems to be a significant predictor of cognitive and behavioural outcomes in later life.5
Breast feeding or bottle nutrition is initiated during hospitalisations, and as the premature infant grows and develops, the parents gradually assume responsibility for the provision of primary care. It is important for premature infants to receive breast milk because it provides pronounced health benefits.6 Mothers are encouraged to express breast milk approximately every third hour to feed their infant in order to stimulate the breast and prepare for when the infant is ready to breastfeed. Despite these recommendations, at discharge, premature infants are not breast fed to the same extent as term infants. Among other factors, a low GA, mother's lack of privacy during breast feeding, mother's level of stress and the lack of use of baby-friendly initiatives in neonatal wards seem to limit breast feeding success.6 A previous study showed positive effects of test weighing on establishing earlier exclusive breast feeding.7 Additionally, a newly published study found that the proportion of breast feeding decreases from 68% at discharge to ∼40% around 1-month post discharge from the neonatal ward.8 A Cochrane review further demonstrated that any form of extra support can increase the duration of exclusive breast feeding in term infants.9 These findings indicate that there may be a need to create an environment that supports maternal breast feeding of premature infants. In a recent study, parents of premature infants reported that they did not feel that the infant was theirs before returning home.10
Towards the end of their hospital stay, most premature infants will be physiologically stable, although some will still require tube feeding.11 At this point, in most hospitals in Denmark, families are provided the opportunity to participate in early inhomecare programmes to bring their infant home as well as to receive relevant education. These programmes are designed to bridge the gap in the transition from hospital to home and provide parents and infants the ability to be alone and become familiarised with each other outside of the hospital setting.10 ,12 Early inhomecare with tube feeding performed by parents10 ,11 ,13–16 is becoming the standard of care in most Danish hospitals. Qualitative studies have described how the transition to early inhomecare is a difficult experience for new parents, particularly in the first weeks and months after discharge.2 ,4 Although parents in this phase have been looking forward to returning home, they often feel insecure and concerned about their infant's health and well-being.17 At the same time, they want to have control over the situation and function as normal parents regarding their infant.18 In a recent study, parents received knowledge and education4 to accommodate this difficult transition. The families expressed the importance of being assigned to the same nurse throughout the entire process2 and of receiving unidirectional and additional guidance. Early inhome programmes can address parent–child interactions,19 which have been shown to have a significant effect on infant development,4 and could also support mothers in successful breast feeding.
Early inhomecare programmes have previously been followed by support20 from home visits and/or hospital consultations two to three times a week or by the use of telemedicine communication.16 ,21 The effects of home visits and/or hospital consultation support include the prolonged provision of breast milk,22 a lower risk of infections during tube feeding20 and higher parental satisfaction;14 furthermore, early inhomecare for premature infants results in fewer readmissions, less unscheduled support and shorter lengths of hospitalisation.14 A new Cochrane review and a randomised study on these programmes were not able to find significant differences in exclusive or partial breast feeding.11 ,20 Moreover, no differences in parental anxiety or confidence were found; however, mothers in early inhomecare programmes felt better prepared to take care of their infants.11 Although home visit support shows promising results, it requires comprehensive nurse resources and can therefore be an expensive and resource-demanding approach.23 To date, no studies have offered round-the-clock home visit support. A randomised controlled effect study from Sweden that used less resource-demanding video consultations showed that families welcomed this option and that the need for home visits was reduced.16 ,24 These findings indicate that telemedicine may be a viable option to address the need for support in the early inhomecare period. Furthermore, using an application to collect daily data has great potential in telemedicine.16 The use of technology provides parents the opportunity to be at home and still be in close contact with hospital staff,16 ,21 ,23–26 and it gives hospital staff the opportunity to provide equal care to all parents regardless of their distance from the hospital. The concerns raised about the use of technology have been that it affects the communication between parents and nurses27 and that the occurrence of frozen screens may affect video communications.28 Telemedicine is a very new and unexplored field in the neonatal setting, and there is a lack of knowledge of its effects on breast feeding, parental confidence and parent–infant interactions as well as a lack of experience with the use of video consultations and smartphone applications. The aim of this study is to examine the effect (1) and evaluate the process (2) of early inhomecare (PreHomeCare) with video consultations and mobile applications compared with the effect of inhospital consultations. The hypothesis is that the intervention will positively influence the continuation of breast feeding by providing1 easily accessible knowledge about breast feeding (application),2 available guidance at all hours from a nurse (video consultation) and3 home weighing of the infant (weight). Effect study (1): The objective is to test the effects of video consultations and the mobile application on the proportion of exclusive breastfeeding mothers, parent–infant interactions and parental confidence with premature infants after the PreHomeCare programme. Process evaluation studies (2): The objectives are to explore nurses' communication (regarding nursing practice, dialogue and information) during the parent–nurse interactions in the video consultations and to explore how parents of premature infants experience PreHomeCare and the use of technology.
PreHomeCare study
Method
Mixed methods study design
The effects and process of the project will be evaluated using the framework outlined by the intervention mapping approach.29 The study will apply a mixed methods design comprising a randomised controlled intervention study with two parallel arms for the evaluation of effects, targeting the primary study population and two qualitative studies for the process evaluation of the intervention: a field study and an interview study, primarily targeting the secondary study population of nurses involved in the intervention.
The primary study population of early discharged parents with premature infants will be randomised into two groups: the intervention group, which will receive the smartphone application and video consultations in the PreHomeCare programme, and a control group, which will receive usual care (hospital consultations) in the PreHomeCare programme (see figure 1).

Project overview.
Setting
There are 19 neonatal wards in Denmark, and this study is being conducted in four of them (in different geographical parts of Denmark). Study inclusion began in November 2015. These wards all receive premature infants from GA week 27/28 and correspond to a level IIIa ward.30
PreHomeCare: The care in these neonatal wards is provided by registered nurses (RN) who are trained in caring for premature infants. All nurses can participate in the early inhomecare programme, as all are familiar with and trained in this type of care; however, 3–4 nurses on each ward have special interests in early inhomecare. These nurses are the most experienced in this field and work in practice and in experience sharing and will thus serve as the nurses responsible for the project. The wards assign the families a contact nurse who follow the family through the admission and early inhomecare.
The criteria to participate in early inhomecare are that the infant has a GA ≥34+0 at the start of inhomecare, does not have apnoea, maintains a normal body temperature, gains weight, receives tube feeding, has started breast feeding/bottle nutrition and does not need medical treatment. The goals of early inhomecare are to strengthen the parent–child relationship, support the parents' skills, ease the transition to home and support mothers in practicing exclusive breast feeding.
When the family returns home in early inhomecare (usual care), they attend 2–3 planned visits to the hospital to talk with a nurse, primarily the contact nurse. The content of this discussion pertains to the nutrition plan, infant's actual weight, bottle/breast feeding progression, family life, infant's general well-being, expression of breast milk, use of nipple shields and tube feeding, among other topics.
Study status
As of September, 50 infants/parents from the participating neonatal wards had been enrolled in the study. We expect to finish enrolment in 2018.
Inclusion and exclusion criteria
Parents who have hospitalised infants born before 37 weeks' gestation who fulfil the criteria for early inhomecare, who speak Danish or English, understand the Danish text in the application and have Wi-Fi/LTE/HSDPA in their home (programme phones provide LTE/HSDPA) will be invited to participate.
The exclusion criteria are infants who do not meet the criteria for early inhomecare or parents who require additional parent–infant observations regarding attachment or eye contact or have low parenting skills based on an individual assessment of the nurses or doctors.
Plan for randomisation
The parents will be informed about the PreHomeCare programme by the nurses on admission to the neonatal ward. When the infant starts breast feeding or bottle feeding, the parents will be informed verbally and in writing about the project if they are interested in going home. After obtaining written consent from the parents and consent for their infant's participation, they will be randomised to either the intervention or control group using fixed block randomisation in a 1:1 ratio per site (at the individual level) using a website-generated randomisation procedure. At inclusion, the nurses will have access to the website to obtain the randomisation result. The inclusion and exclusion of participants will follow the Consolidated Standards of Reporting Trials (CONSORT) statement,31 see figure 2.
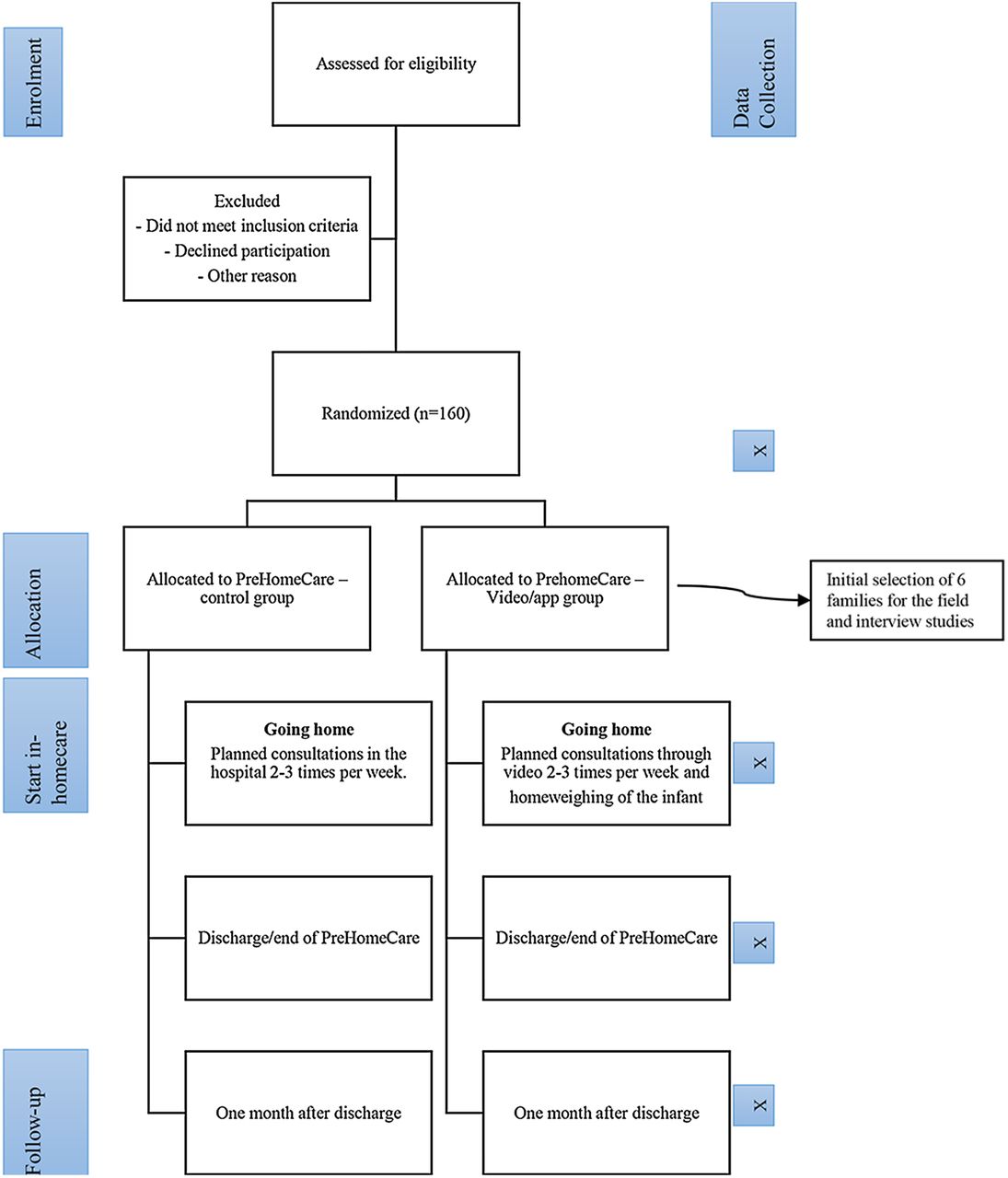
Flowchart of PreHome.
Programme implementation and monitoring procedures
The secondary study population primarily consists of nurses. To ensure a standardised implementation of the programme, the protocols will outline how the programme should be delivered. An instruction manual for the nurses has been developed in Danish32 to ensure that the application is easy to understand and use. The manual contains instructions and pictures of the application to guide the user. All four participating wards have three or four project nurses (the nurses with a special interest in early inhomecare) who have received training in the use of the smartphone application, video consultations and the manual. The remaining staffs at the neonatal wards have received training at staff meetings and bedside.
All the project nurses on the wards have quarterly meetings with the project sponsor/investigator to discuss study challenges, study progress, programme delivery and data collection.
Procedure
The intervention group will receive the smartphone application at inclusion, the manual32 with instructions for its use and training in how to use the application in the hospital. When the families return home, they will use the application, attend the planned video consultations 2–3 times a week and have the ability to call the neonatal ward 24 hours a day, 7 days a week, until the infant receives full nutrition from the breast or bottle and gains weight (minimum 20–25 g/day), see figure 3. Parents will borrow a baby scale to weigh the baby at home. All equipment (phone, weighting scale) will be provided from the neonatal department throughout the project.

{kind=link}
{kind=link}
{kind=link}
Parents’ and nurses.
The mobile application and video conference system, Præmatur Lifeline Viewcare A/S Herlev,33 were developed through clinical and parental evaluation and aim to provide the parents a secure and safe early inhomecare experience. The application addresses the parents' wish to have access to guidance around the clock and consists of three components: (1) usable knowledge (breast feeding, breast feeding position, infant signals, skin-to-skin contact, physiotherapy and so on), (2) video contact/participatory guidance, through which parents can contact the ward and (3) data registration (nutrition, vitamins and weight), including the ability to receive reminders, access patient history and share reports (notes, nutrition and weight) with the hospital. The digital solution activates knowledge through the search options and info icons included in the application.
The control group will be offered hospital consultations (usual care) 2–3 times a week (for 1–2 hours) and the opportunity to call the neonatal ward 24 hours a day, 7 days a week, until the infant receives full nutrition from the breast or bottle and gains weight (minimum 20–25 g/day). The parents will record the infant's nutrition between hospital visits on paper.
Both groups will learn to insert the feeding tube, receive training in first aid before PreHomeCare and will borrow breast pumps (if needed) as part of the PreHomeCare programme. All parents will receive leaflets and verbal information concerning the care of the infant. The overlap between the intervention and control groups while at the ward is not expected to have any implications on the results. If an infant requires medical and/or other services during the PreHomeCare programme, these services will be offered regardless of randomisation group.
Power calculation and sample size
The main hypothesis is that a larger proportion of breastfeeding women from the intervention group will continue breast feeding at least 1 month after discharge. Prior research6–9 suggests that the intervention will be able to increase the proportion of exclusively breastfed infants by providing easily accessible knowledge about breast feeding, guidance at all hours from a nurse and the ability to weigh the infant at home. Applying a significance level of 5% for a two-sided two sample proportion test, a sample size of 80 in each group would lead to a power of 80% to detect a difference of 55% versus 41.5% of breastfeeding women in the two groups after 4 weeks, assuming that 68% of mothers were breast feeding at discharge.8
Concerning the scores on the Mother and baby interaction scale (MABISC) and the Karitane parenting confidence scale (KPCS),34 ,35 small differences between two points in the scores can be detected with a power of 80% based on power calculations for a two sample t-test (data for the calculations are based on previous publications using the MABISC and KPCS). The inclusion period is expected to be 2 years based on the sample size calculations, a participation rate of 0.7 and a withdrawal rate of 0.1, resulting in the inclusion of a minimum of 160 premature infants.
Variables and data collection
The primary outcome is the proportion of exclusive breastfeeding mothers 1 month after discharge/end of the PreHomeCare programme and is defined as infants feeding directly at/from the breast or receiving mother's expressed milk in a bottle based on the definition provided by the WHO36 (see table 1).
Data collection
The secondary outcomes are parent–baby interactions according to the MABISC,35 parents' feeling of confidence determined by the KPCS34 and active knowledge of the premature infant 1 month after discharge/end of the PreHomeCare programme. The MABISC measures the mother–child relationship using 10 items scored on a five-point Likert scale (never, not often, occasionally, most of the time, always). The KPCS measures the parenting confidence of the infants' parents using 12 items rated on a 4-point Likert scale (no, hardly ever; no, not very often; yes, some of the time; yes, most of the time) (see table 1).
The secondary variables include data on the infant, parents' socio-demographic characteristics, breast feeding experience, experience with the PreHomeCare programme and number of contacts with the hospital after discharge (see table 1).
Data collection will be completed using a self-reported questionnaire that will be emailed to the mothers and completed electronically by the mother with assistance from the father or another close relative using the online survey programme SurveyXact.37 Data will be collected equally in both groups. To minimise the number of those lost to follow-up, an email (and a text message) will be sent twice as a reminder. No gifts or cash incentives will be used to motivate participation.
Survey data will be obtained at four time points: inclusion, discharge/end of the PreHomeCare programme, 1 month after discharge and 1 year after discharge. The questionnaires will be distributed by the principal investigator.
The questionnaire contains 50–70 items. The validity and reliability of the study will be enhanced by using validated questions. Questions will be added for topics in which we have not found validated items, namely, to evaluate the use of the equipment (scale, smartphone, application) (table 1). All questions including the self-constructed ones were assessed for face validity. The self-reported questionnaire was pretested among 10 different parents to identify the duration of the questionnaire, any ambiguities and difficult or poorly worded questions by debriefing with the respondents;38 the questionnaire was then revised and finally tested again in two rounds.
Data on the infant will be gathered from hospital records and from application data by the nurses. These data will be registered in electronic case report forms (eCRFs) in an online Clinical Trial Management System39 by the responsible nurses. The data collection time points are depicted in table 1.
Statistical analysis
Quantitative data will be analysed using STATA/IC V.14.0 (Stata Corp CP, Texas, USA) software. The reporting of results will follow the guidelines of the CONSORT statement.31
The results of the intervention and control group will be compared and analysed following the ‘intention to treat’ principle and randomisation will remain intact. The study has a cluster structure with care in different hospitals, and this clustering will be considered when data are analysed (use of a random effects model is a possibility). Data will initially be analysed with univariate analysis using a 2×2 contingency table (χ2 test and Fisher's exact test). Multivariate regression models will be used to adjust for confounders and other statistically significant explanatory variables. However, the initial randomisation should reduce the overall risk of confounding. The effect of the intervention according to the proportion of infants exclusively breast fed will be analysed using linear regression models. The MABISC and KPCS will be analysed using paired and unpaired t-tests. The number of readmissions will be evaluated using Poisson regression and will be further assessed by Kaplan-Meier curves as time to first readmission. A significance level of 0.05 will be applied in all analyses.
Process evaluation study design
Field observation study
The aim of this field study is to explore the nurses' communication (nursing practice, dialogue and information) through passive participant observation of the video consultations while in the parents' home.41 As the transition from hospital to home can be a vulnerable period for parents, they may require guidance. The field observation method was chosen to explore nursing practices and will be based on Spradley's methodology regarding ‘participant observation’.41 The observations will occur in the parents' homes and will focus on the nurse's communication and interaction with the parents on screen to gain insight into how video communication affects their dialogue.
Interview study
A qualitative evaluation will be conducted to explore how parents of premature infants experience the PreHomeCare programme and the use of technology, that is, applications and video consultations, and the baby scale. As parents describe the transition from hospital to home as being difficult, and as they have reported feeling insecure, a qualitative interview study was chosen to gain in-depth knowledge of the parents' perspectives of PreHomeCare. The study will be planned and conducted with inspiration from Kvale and Brinkmann′s methodology.42 The interview study will explore PreHomeCare from the parents' perspective by uncovering the meaning contained in their experiences.
Data collection
Six families will initially be selected from the intervention group to be the subjects of the field observations. In accordance with the qualitative tradition, the exact number of participants cannot be determined in advance. The data collection will continue until saturation has been reached, that is, until no new information is obtained.43 The selected parents will be informed about the aim of the study after randomisation. To ensure variation in the sample, the respondents will be strategically selected based on the premature infants' GA at birth (GA is related to the length of hospitalisation). The observations will occur in the parents' home during the three scheduled video consultations. The observer will stand to the side during the video consultations in the parents' home and will conduct an informal follow-up with the parents. Through ‘passive participant observation’ of the situation (video consultations), the people (parents, infants and nurse(s)) and the physical setting can be openly observed. Field notes will be recorded according to an observation guide inspired by the theory of ‘active listening’.44 Thus, concrete descriptions of what is said and done, the tone of voice, the researcher's impressions and the assumptions of the communication between nurse(s) and parents will be documented.41 After the observations, the field notes will be written in prose.
Parents in the field observation study will be interviewed45 ∼1 month after the end of the PreHomeCare programme, as the parents are expected to have reflected on the programme by this time point. As fathers and mothers may experience PreHomeCare differently, clarifying questions will be addressed to each parent using a semistructured interview guide. The interview will occur in the parents' home or in a place of the parent's preference. The primary aim of the interview will be to explore the main question: ‘how did you experience PreHomeCare?’ with a particular focus on what was especially meaningful for the parents. The interviewer will listen with an open mind and ask clarifying questions to gain as close an understanding as possible of the parents' everyday life experiences with PreHomeCare and the technology. Immediately after the interviews, the mood and other impressions will be noted, and the taped interviews42 will be transcribed verbatim.
Data analysis of the qualitative substudies
The transcripts of the interview data will be analysed using qualitative content analysis.46 This process includes open coding in which notes and headings are written in the text and are subsequently grouped into meaning units. Codes are compared with identify differences and similarities and are then transformed into categories and subcategories. Finally, the underlying meanings will be interpreted and formed into themes, either at the manifest or the latent level. Considering the first author's background in the neonatal ward, objectivity during data analysis will be gained through an awareness of the author's preunderstanding and through critical reflections to maintain an open mind throughout the analysis process.42 The supervisors, AN and HK, will be involved in the analysis and interpretation of the data. The first author will do the primary coding. Subsequently, MHP, AN and HK will conduct the analysis and discuss the codes, emerging categories and subcategories with each other until consensus is reached.
Ethical considerations, registration number and name of trial registry
This project is registered with Clinicaltrials.gov; Clinical.gov ID NCT02581800.
Parents will be informed about the project verbally and in writing; the purpose of the study, the right to withdraw and the confidentiality of the data will be explained by project nurses, and informed consent will be obtained before inclusion. The parents will have a minimum of 1 day to decide whether they wish to participate. Confidentiality will be guaranteed, and participation is voluntary. The participants will be informed that the results of the interviews and field study will be included in publications. The data will be safely stored, and only MHP will have access to the final study data set. Positive as well as negative results of the effect (1) and process evaluation (2) will be published in separate manuscripts. The ethical aspects of the study follow the basic principles for research outlined in the Helsinki Declaration and the Northern Nurses' Federation (2003).
Perspectives
This study will lead to an improved understanding of the effect of the PreHomeCare programme and parents' experiences with it. Furthermore, it will provide insight into the factors needed to define clear goals regarding the quality of the treatment and care of premature infants in the end stages of their hospital admission/during PreHomeCare. The knowledge gained from this project is expected to be used to further develop care for premature infants. The increased effectiveness of infant care can address challenges in healthcare and help redistribute economic and professional health service resources. The parents/infants who reside further away from the hospital could be able to use this technology for different hospital follow-up visits.
This study will contribute new knowledge of whether video consultations (participatory guidance) and Smartphone applications (usable knowledge and data registration) address parental needs for support during early inhomecare.
Acknowledgments
We would like to thank the project nurses Birgit Hagelskær Dam (ICBLC), Catarina Krogh Andersen, Charlotte Maria Melgaard, Dorte Lissi Steen Hansen, Hanne Dalsgaard Loberg, Inge Nedergaard Henriksen, Inger Norup, Irene Dahlstrøm Larsen, Kirstine H Rotvig Erichsen, Merete van Deurs Petersen, Sille Nymann, Tina Thaulov Stoltenborg and Vibeke Fris Kyndesen (ICBLC) and all other staff at Næstved, Roskilde and Viborg neonatal departments for their daily work, engagement and involvement in the project. Furthermore, we would like to thank the nurse managers, Hanne Schjøning, Lis Dueholm, Birthe Kruuse, Karin Hallum (ICBLC) and Annemi Frandsen, the doctors, Gholamreza Krog Dayani, Hristo Stantchev and Jens Peter Nielsen, and the other ward staff for making the project possible and ensuring the organisational framework to support the project.
References
Footnotes
Contributors MHP conceived the study and drafted the project description and protocol under supervision from associate professors HK and AN. RD served as the statistical supervisor. HS contributed with comments on the study protocol and project description as well as by assuming medical responsibility. MHP obtained funding for this PhD project. All authors contributed to the final manuscript, and all authors can be held accountable for the accuracy and integrity of any part of the work. All authors have read and approved the final manuscript.
Funding This PhD project is financed by Aarhus University, the Danish foundation TrygFonden, the Health Foundation, Danish Nurses' Organization, Region Zealand Health Scientific Research Foundation and the local research foundation of NSR hospital.
Competing interests None declared.
Ethical approval This project has been approved by the Regional Ethics Committee (Region Zealand, Denmark), registration number: SJ-431, and the Danish Data Protection Agency, registration number: REG-113-2014.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.