Article Text

Abstract
Objectives There is a shortage of doctors working in rural areas all over the world, especially in low-income and middle-income countries. The choice to practise medicine in a rural area is influenced by many factors. Motivation developed as a medical student is one key determinant of this choice. This study explores influences on medical students' motivation to practise in rural areas of low-income and middle-income countries following graduation.
Design A systematic review was conducted to identify influences on medical students' motivation to work in rural areas in low-income and middle-income countries. Papers reporting influences on motivation were included, and content analysis was conducted to select the articles. Articles not published in English were excluded from this review.
Results A rural background (ie, being brought up in a rural area), training in rural areas with a community-based curriculum, early exposure to the community during medical training and rural location of medical school motivate medical students to work in rural areas. Perceived lack of infrastructure, high workload, poor hospital management and isolation are among the health facility factors that demotivate medical students for medical practice in rural areas.
Conclusions Medical school selection criteria focusing on a rural background factor and medical education curriculum focusing on rural area are more relevant factors in low-income and middle-income countries. The factors identified in this review may assist the planners, medical educators and policymakers in low-income and middle-income countries in designing relevant interventions to positively influence rural choices where the shortage of rural physicians is an ongoing and increasing concern.
- MEDICAL EDUCATION & TRAINING
- medical students
- rural health
- Motivation
- low and middle income countries
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study focuses on the motivating factors among medical students, unlike most studies, which focus on medical doctors and specialists.
Using a conceptual framework based on a problem tree approach structured the findings and discussion.
This study is relevant for all low-income and middle-income countries that face challenges in recruiting medical doctors to work in rural areas.
The inclusion of English language articles only in this review may have resulted in missing some possibly important papers published in other languages.
The conclusion is based on low-quality evidence only, as studies with moderate and high evidence were not found in the literature search.
Introduction
Approximately half of the world's population resides in rural areas, while <25% of physicians provide services to rural communities.1 Poor access to health workers impacts more than one billion people,1 with communities in Africa and Southeast Asia experiencing the most significant disadvantage.2 Unequal distribution of healthcare workers between urban and rural areas leads to poorer health among rural people.3 ,4 This in turn affects the health and development-related indicators of the countries.5
In a cross-sectional study in 2012, 9 out of 10 students in Nepal intended to work in Nepal after graduation from medical school, but only 1 out of 10 were interested in possibly working in rural areas.6 In similar studies since 2010 in other countries, career intentions in rural locations among medical students are reported to be very low in Bangladesh,7 sub-Saharan Africa8 and South Africa.9 Studies from India and Ethiopia show slightly higher rates with about one out of five medical students showing career interest in rural locations after graduation.10 ,11
Decisions made by new doctors about where to establish their careers are influenced by a range of personal, economic, familial, cultural and environmental factors.12 Medical training, local and national policy, and factors related to the location of the health facility also play a role in career decisions.13 Decisions about practice location are made during medical training.14 ,15 Experiences during medical school have a powerful influence over many students' choices.16
Many determinants contribute to medical graduates' choices relating to career locations.17 It is an important and difficult decision for many medical graduates about where to start their career. The choice influences future career choices and opportunities, as well as family and social life.18 Understanding what motivates the medical students at the time they are making this choice will assist medical educators, researchers and policymakers to more effectively structure their educational experiences and establish appropriate motivations that encourage more medical graduates to practise in rural settings.19 ,20 The WHO has recommended a set of interventions to increase the access of health workers in rural areas globally.5
Relevant reviews can be found regarding the medical students' motivation to work in rural areas of high-income countries. The factors identified in reviews from high-income countries include the rural background of the medical student and the medical school selection criteria to select the students with rural background as motivators for future rural practice.15 ,21–27 Rural areas of high-income countries are different from rural areas of low-income and middle-income countries (LMICs) and differ by income groups of countries, yet the motivation for working in rural areas is a challenge faced by all countries.
No review focusing on medical students' motivation to work in rural areas in LMICs was found in a thorough literature search. The current study sought to review the literature to identify factors influencing medical students' motivation to practise in rural areas following graduation.
Methods
Study design
A literature review was conducted in PUBMED, COCHRANE library, SCOPUS, EMBASE, ERIC and Google Scholar databases in 2016 by two independent researchers.
Conceptual framework
The Bland model,28 illustrating the student characteristics and school characteristics that influence the choice of medical specialty, was used as a reference to prepare a problem tree, which was used to develop a conceptual framework for content analysis, where motivation among the students is a dependent variable influenced by these factors. Individual, work, social and environmental factors interact to influence motivation. These factors guided the construction of the broad categories of a problem tree for medical students' motivation (figure 1).29 ,30

Conceptual framework.
Search strategy
Keywords and Medical Subject Headings (MeSH) were used for each of the three concepts of interest.
Medical students: ‘medical students’ OR ‘undergraduate medical students’.
Motivation: ‘motivation’ OR ‘career choice’ OR ‘intention’.
Location: ‘rural areas’ OR ‘underserved area’ OR ‘remote area’ OR ‘rural practice’.
We used the search strategy (undergraduate medical student) OR (medical student) AND (motivation) OR (career choice) OR (intention) AND (rural area) OR (remote area) OR (Rural practice) for PubMed search.
Inclusion and exclusion criteria
The inclusion criteria were set to include all articles that were published between 2000 and July 2016 in peer-reviewed journals and reported factors influencing medical students' motivation to work in rural areas. Definitions of ‘rural area’ differ from author to author and from country to country.31–33 For this study, the author's use of the terms ‘rural area’ or ‘underserved area’ were accepted. Studies reporting practice in LMICs were included. Articles from high-income countries and articles not published in English were excluded.
Outcome measurement
The outcome of interest in this review is the motivation of medical students to work in rural areas following graduation.
Data extraction
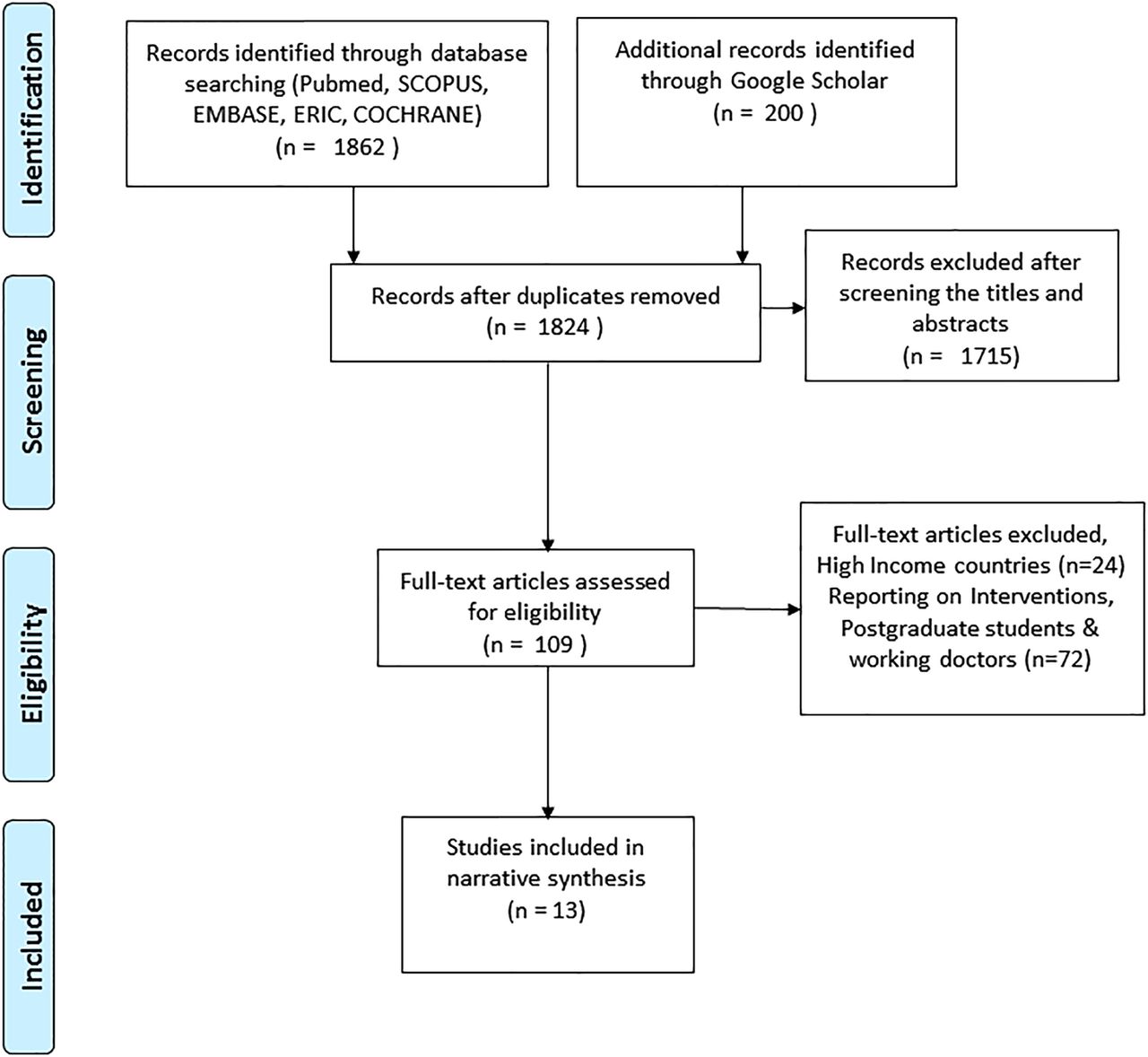
Following identification of articles from the databases and removal of duplicates, titles and abstracts were screened against the inclusion and exclusion criteria. A content analysis was then undertaken with the papers satisfying the inclusion criteria. Where the review of the full text revealed a paper that did not meet inclusion criteria, it was excluded from further analysis. The title and abstract screening and content analysis were performed by two independent reviewers. The complete article selection process is reported using the PRISMA flow chart (figure 2). The PRISMA checklist was used to guide the report writing of the systematic review.34 The reported factors influencing medical students to practise in rural areas were extracted using data extraction forms.

{kind=link}
{kind=link}
Articles selection process.
Synthesis of results
Based on the conceptual framework (figure 1), motivational factors extracted from the papers in this review were grouped into five categories: (1) health facility-related factors; (2) personal and lifestyle factors; (3) medical training and curriculum factors; (4) medical school factors; and (5) policy-related factors.
Quality assessment
The quality of evidence was assessed using the Grading of Recommendations: Assessment, Development and Evaluation (GRADE) approach for observational studies.35 The articles in this review were independently assessed for quality by two reviewers and then an agreement was reached on the final quality category.
Results
The initial database search identified 1862 articles, and following the removal of duplicates and a title and abstract scan, 109 articles were included in the full-text review. A further 96 papers were excluded following a full-text review (24 papers from a high-income countries study and 72 papers not fitting the inclusion criteria).
Thirteen studies were included in this review. The review included eight cross-sectional studies, two qualitative studies, two mixed (qualitative and quantitative) studies and one discrete choice experiment. There were two articles from upper middle-income, three articles from lower middle-income countries, seven articles from low-income countries and one article covering lower middle-income and upper middle-income countries.36 The characteristics of the 13 included articles can be found in table 1.
Characteristics of articles reporting factors influencing motivation of medical students to work in rural areas following graduation
A summary of the factors influencing the motivation of medical students to work in rural areas after graduation is listed in table 2.
Summary of articles reporting factors influencing motivation of medical students to work in rural areas following graduation
Health facility-related factors
Health facility-related motivating factors and impediments to rural practice were found in seven articles. Motivating factors for rural practice included medical students from Uganda expecting that communication with patients in rural areas would be easier, better teamwork, friendly environment.37 They also expected that staff would be more supportive38 and that there would be more career development opportunities37 in rural areas than in urban areas. The students perceived that financial incentives6 in Nepal or higher salaries38 ,39 in Botswana and India and provision of good housing39 ,40 in Ghana and India for rural locations acted to motivate their decision to work in rural areas. Impediments to rural practice are reported from studies in low-income countries as perceived lack of infrastructure, equipment, supplies and communication facilities within the rural health facility.37–42 In Botswana, the expected weak referral system in health and poorly functioning health facility were reported as impediments to future rural practice.38 In Malawi, expectations of a high after-hours workload in rural health facilities, trade-off to administrative works over clinical work, lack of opportunities for private practice and high community expectations of physicians were the impediments to practising in rural areas.41 Poor hospital management in rural areas was a perceived impediment to rural medical practice among the students in Uganda and Ghana.37 ,40 Limited professional development opportunities,38 ,39 ,42 professional career stagnation38 and lack of opportunities for higher education and support39 ,42 were perceived as impediments among students for a future career in rural locations in Botswana, India and Nepal.42 Rurally located health facilities are considered unsafe during political instability by medical students in Nepal and Uganda.37 ,42
Personal and lifestyle factors
Personal and lifestyle-related motivating factors and impediments to rural practice were found in 11 articles. Personal and lifestyle motivating factors include findings from Nepal and South Africa, where male students are more likely than female students to practise in rural areas.6 ,9 ,43 ,44 Rural background of the student, such as being born in a village, was a motivating factor reported from Botswana and Ethiopia.10 ,38 Completing their elementary school in rural area in Ghana, Nepal, influenced medical students for future rural practice.6 ,43 ,45 Having lived in a rural community was a motivating factor for students to return to rural areas for medical practice in Ghana.37 ,45 Perceived proximity to family when working in a rural area was a motivating factor for practice in rural areas by students in Botswana.38
Students with a paramedical background prior to medical school, completing their high school at an older age and lower grades in medical school were some characteristics found to be linked with working in rural areas of Nepal.43 Students perceived diverse work experience as positive motivators for medical practice in rural areas in Botswana.38 Medical students from a lower socioeconomic status in Ghana are more motivated to work in rural areas following graduation. The reason for this, according to the author of the study, is due to a greater understanding of poverty that motivates them to help the poor.45 In Malawi, medical students' personal values motivate them to serve in rural areas, considering rural service as a part of their duty as a citizen.41
Impediments include the needs of the spouse and families for better education for children, perceived to be available in the cities and not rural areas, as reported from Ghana.40 The perceived lack of proper housing in a Malawian study,41 perceived lack of recreation and entertainment facilities for themselves and the families and the perception of being isolated from friends and family circles in Botswana and Uganda,37 ,38 along with high travel costs associated with travel to and from the rural areas, are impediments to medical practice in rural areas of Ghana and Uganda.37 ,40 Students from families with high income were found as a negative predictor for future career location as rural areas in Nepal.6
Medical training and curriculum factors
Medical training and curriculum-related motivating factors and impediments to rural practice were found in two articles. Medical training and curriculum-related factors from a low-income country, Uganda, show that a community-based medical curriculum motivates and prepares a medical student for future practice in rural areas. These factors include rural posting and training in rural areas.37 Students in Nepal perceive that training in resource-constrained settings of rural areas as a medical student prepares them for medical practice in those areas.42
Medical school-related factors
Medical school-related motivating factors and impediments to rural practice were found in three articles. Medical school selection criteria to select students from a rural background was a positive influence to motivate students to rural practice in the future in the Philippines, South Africa and Sudan.46
Medical school-related impediments include high tuition fees paid for education in Nepal which is associated with no interest in working in rural areas.6 ,42
Policy-related factors
Policy-related factors are reported in two articles in this review. In Nepal, government scholarship schemes provided to students with a rural background have been reported as a positive factor to influence their motivation. Students who receive these scholarships are obliged to serve in a rural area for a certain number of years.6 Shorter contracts in rural areas were also considered as a potential motivator for rural areas by medical students after graduation in Ghana.40
Discussion
The conceptual framework illustrates the influence of each of the five categories of factors on the motivation of the medical students to practise in rural areas after graduation (figure 1). The health facility-related factors (which are generally related to the development of the national health system) identified in this study are acting mostly as impediments for medical students to work in rural areas due to perceived shortcomings in the rural health facilities. Lack of equipment and supplies, lack of peer support, poor hospital management, and added burden of administration and high expectation from the community is perceived to have a very strong discouraging effect among the medical students involved. These are found in studies from all low-income countries and in one out of five studies from middle-income countries.
Rural areas may differ from country to country; however, studies suggest that the rural background of a medical student in any country motivates them to work in the rural area of that country. The choices of the individuals are influenced by the personal circumstances of one's marriage, spouse's choice, family needs and lifestyle choice for living, housing and recreation. The personal factors identified in this review are mostly impediments that drive individuals away from practising in rural areas. Personal experiences and exposure to rural areas is likely to motivate the individual to enjoy rural lifestyles and thus work in rural areas. Perceived friendly environment and perceived better patient relations motivate students towards working in rural areas.
Relevant factors for medical students are the medical training and curriculum factors. Community-based education gives a positive motivation to the student towards rural communities. Rural trainings are expected to bring the student closer to the community. The community-based education curriculum builds on the personal factor of rural experience, hence motivating medical students to undertake future medical practice in rural areas as mentioned earlier. There is a need for more research in LMICs on how the community-based medical education and rural-based medical training can motivate medical students to further their medical practice in rural areas.
Closely linked to the education and curriculum factor is the medical school factor. Since the medical school plays an important role from selection of the candidates to implementing its curriculum to producing a doctor, the use of appropriate selection criteria is very important. The schools with criteria to select students with a rural background, experience and education could motivate medical students to serve in rural areas after graduation. The criterion ensuring inclusion of underserved communities is seen as a potential solution to increase a more even distribution of doctors in rural areas.46 This can be seen as an important and feasible factor to consider when designing any interventions to increase the number of medical doctors in rural areas of LMICs. Training the students in rural settings adds to the rural interest of the student. Availability of training locations in low-income countries is an issue that also may need to be explored. While factors like community-based education and rural training are being discussed, attention should also be paid to the reality that the health facility in rural areas of low-income countries lacks even the basic infrastructure. Training in rural health facilities may motivate the students to pursue careers in rural locations. However, countries may also need to invest in the development of rural health facilities.
A medical school-related impediment to rural practice is the high tuition fees paid at private medical schools. National policies that provide financial support for medical education in return for service in rural areas can influence students' choices towards rural practices. They voluntarily opt for the schemes in order to start their medical education. Short contracts could also work in favour of motivating rural practice. Taking into account country-specific relevant factors, policy interventions may be designed as outlined by the WHO,5 to increase medical doctors in rural areas through the motivation of the medical students.
The basic factors linked with physical development like infrastructure and health facilities are more reported as impediments to rural practice in the future from low-income countries compared with middle-income countries.
Relationship between the factors
All five categories of factors are linked with the income level of the country. There is most likely an interplay between the factors that contribute to the overall shortage of the health workforce in rural areas of LMICs. Addressing factors individually as well as looking across the factors is important. Strategies that address multiple influences would be useful. Rural background is the most commonly reported factor in this review and in some high-income countries, some preference has been given to rural students for medical school admission.47–49 Medical school factors that include consideration of student admission, curriculum geared towards rural areas and rural exposure during placement have been reported in the literature for high-income countries as important.23 ,26 ,50–54 Although the literature we found on LMICs had only a limited focus on medical school factors, potentially developing strategies to create graduates who are more confident and committed to working in resource-limited rural areas could be helpful. A sequence of interventions from selective admission for students with a rural background, community-based medical education and clinical training in rural areas during undergraduate medical education is seen to increase rural practice motivation among medical students.26 Establishing medical schools in rural areas could be adopted by governments to potentially increase rural motivation among the medical students.55 The health facility factors appear to be an important influence in low-income countries, where the disparities between urban and rural facilities are greatest. Communities, medical schools and governments all need to work together to develop the health infrastructure and staffing of facilities in rural areas. High tuition fees in medical schools reported from low-income countries could be linked with the policy intervention of providing scholarships to medical students. This may address the obstacle of high tuition fees to support students from rural areas to attend medical school. A policy of financial aid to students during medical education has been used as a successful strategy in high-income countries.56 ,57 These factors may need further investigation in terms of motivation to work in rural areas following graduation.
Quality of included studies
Since the available studies are either cross-sectional, mixed methods or qualitative, the studies included in this systematic review are of either low quality or very low quality as classified by the GRADE approach35 for observational studies. However, since these are the only studies that are found for review, the findings may still be valid to summarise the factors influencing medical students' motivation to practise in rural areas of LMICs. Intervention studies, cohort and case–control studies may have generated higher quality of evidence in this subject matter.
Limitations of the study
The search strategy to include only English language could have resulted in missing some relevant articles in other languages. The choice of key words and their combinations may have limited the search results to the identified studies in this review. Since only observational studies were found, there were no studies that were of moderate or high quality of evidence according to the GRADE approach.
Conclusions
The current review suggests that among the powerful motivators for rural practice following graduation is rural background. Selecting medical students from rural backgrounds seems an important area for low-income countries. Together, rural background and community-based medical education perhaps act to increase student exposure to the needs of rural communities and the personal benefits of rural practice. Low-income countries could also consider ensuring a minimum infrastructure of health facilities in rural areas in addition to addressing other important factors. An understanding of the factors influencing medical graduates in LMICs is, however, limited. Further identification of locally relevant factors may be useful to design country-specific interventions.
Acknowledgments
The authors would like to acknowledge the resources and guidance received from the Royal Tropical Institute, Netherlands for writing this paper. The authors acknowledge the support received from Hellen Gelband and Dr Sarity Dodson to improve the English language in the paper.
References
Footnotes
Contributors SSB, PACZ, PKP and AJS all contributed to the conception of the study. SSB, PACZ and AJS analysed and interpreted the data of the work. Drafting of the manuscript and revising it critically for the important intellectual content was done by SSB and PACZ. Manuscript preparation, editing and finalising of the version to be published is the work of SSB, PACZ, PKP and AJS. All authors agree to be accountable for all aspects of the work related to the integrity of the work.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.