Article Text

Abstract
Background Physical activity on prescription schemes (PARS) are health promotion programmes that have been implemented in various countries. The aim of this study was to outline the differences in the design of PARS in different countries. This study also explored the differences in the adherence rate to PARS and the self-reported level of physical activity between PARS users in different countries.
Method A systematic literature review and meta-analyses were conducted. We searched PubMed and EBASCO in July 2015 and updated our search in September 2015. Studies that reported adherence to the programme and self-reported level of physical activity, published in the English language in a peer-reviewed journal since 2000, were included. The difference in the pooled adherence rate after finishing the PARS programme and the adherence rate before or during the PARS programme was 17% (95% CI 9% to 24%). The difference in the pooled physical activity was 0.93 unit score (95 CI −3.57 to 1.71). For the adherence rate, a meta-regression was conducted.
Results In total, 37 studies conducted in 11 different countries met the inclusion criteria. Among them, 31 reported the adherence rate, while the level of physical activity was reported in 17 studies. Results from meta-analyses show that PARS had an effect on the adherence rate of physical activity, while the results from the meta-regressions show that programme characteristics such as type of chronic disease and the follow-up period influenced the adherence rate.
Conclusions The effects of PARS on adherence and self-reported physical activity were influenced by programme characteristics and also by the design of the study. Future studies on the effectiveness of PARS should use a prospective longitudinal design and combine quantitative and qualitative data. Furthermore, future evaluation studies should distinguish between evaluating the adherence rate and the self-reported physical activity among participants with different chronic diseases.
- PARS
- health promotion
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This the first study that examines the differences in programme characteristics related to physical activity on prescription schemes (PARS) in different countries. The effectiveness of PARS in different countries is examined using meta-analyses and meta-regression.
To examine the effectiveness of PARS, we used two effect size measures: the adherence rate and the self-reported level of physical activity.
To assess the effectiveness of PARS, this study also applied meta-regression that included programme characteristics as covariates.
The selection of abstracts included only English language studies. There are evidence that some studies exist in the Dutch and Swedish languages also.
It was impossible to perform a meta-regression on the self-reported level of physical activity.
Introduction
Physical activity on prescription schemes (PARS) are health promotion programmes delivered through primary healthcare institutions with the aim to increase physical activity among at-risk population groups.1–4 In a nutshell, within the PARS programme the health professional (general practitioner (GP) or nurse) gives a prescription to the eligible person.1 ,5 With this prescription, the person is referred to an exercise professional (physiotherapist) who organises a physical activity programme. Eligible people include those with metabolic disorders such as obesity, overweight, high cholesterol, a diagnosis of cardiovascular diseases, mental health problems, orthopaedic problems, sometimes also respiratory diseases and some types of cancer.1 ,6 The programme is sometimes free of charge but sometimes some payment is required as well, depending on the country where the programme is delivered.1 ,7 ,8 It is usually offered at a local community leisure facility and is provided by a physiotherapist or health professional. The goal of the programme is to provide a tailor-made easy accessible scheme of physical activity that suits the person and her/his medical needs.9 In this way, people with similar needs receive professional help in exercising and also a chance to perform the activities and share experiences with people who have similar needs.
In Europe, PARS programmes were first introduced in the UK during the 1990s.9 In 2002/2003, Sweden, Denmark, Norway and Finland introduced similar schemes7 ,10 ,11 and later on Netherlands, Germany (as a part of the ‘healthy’ Germany programme),8 ,12 Belgium,13 Spain and Portugal14 did the same. Outside Europe, PARS programmes exist in the USA, Canada, New Zealand and Australia.15–17 However, the name of the PARS programme, design and implementation vary between countries but sometimes also within a country.
The UK programme is known as PARS but also as exercise on prescription, while in Sweden the programme is usually referred to as physical activity on prescription (PAP).10 Other synonyms include exercise on referral scheme (ERS), exercise is medicine or green prescriptions.18 In some countries, the programme is known as ERS (applied in the UK and Denmark) whereas in some other countries it is known as PARS (applied in Sweden, Finland and New Zealand).5 ,19 Nevertheless, nowadays, researchers use these terms interchangeably.1 ,20 ,21
Regarding the design of PARS, differences are also observed between countries and also within a country. For example, the UK PARS programmes were developed at a national level, following the recommendation of the National Institute for Health and Clinical Excellence (NICE). NICE defined the requirements or general standards for PARS but each local community is allowed to develop its own unique programme. In 1994, the number of different registered PARS in the UK was 200, while in 2001 the number was three times higher.2 They differ in the targeting of eligible groups, reasons for referral, type of physical activities that are provided and also in the way in which the programme is evaluated.22 In some cases, PARS programmes are accompanied by motivational training for participants.6 Differences are also observed between countries. For example, in some countries, like in Spain, the programme is delivered free of cost, while in other countries patients pay a fee.23 In the Netherlands, the programme is targeting people with health-related risk factors, such as obesity and diabetes, as well as those with low social economic status, whereas in Sweden only people with certain health risk factors are eligible.19
However, differences between countries have been examined only to a limited extent. Previous literature reviews have compared programmes in different countries, mostly in English-speaking countries.20 Programmes from non-English countries such as the Netherlands or Sweden have not been included.20 ,24 Evaluation studies, designed as randomised controlled trials (RCTs), prospective longitudinal studies or cohort studies6 ,22 ,25 ,26 focus on the effectiveness of PARS within the same country or even within the same local communities where they have been implemented.6 ,27 ,28 Those studies also identify three main obstacles related to the effectiveness of PARS, namely a lack of theoretical background for the intervention, low adherence rate among the participants in PARS and unclear evidence regarding the effectiveness of PARS on physical activity.1 ,6 ,29
Following the obstacles acknowledged by previous studies, the aim of this study was to outline the differences in design and effectiveness of PARS programmes in different countries. We particularly focused on the adherence rate and the self-reported level of physical activity. Those two dimensions have been used as measures of effectiveness in previous studies.25 ,30 Furthermore, we compared the design of PARS programmes in different countries. Comparing the design of PARS programmes from different countries can give better insight into how to improve the adherence rate among participants and how to increase the long-term effectiveness of PARS. For this purpose, we performed a systematic literature review and a meta-analysis. We use meta-analysis in order to assimilate the data from different sources and from different countries.31
Background
In 1978, the American College of Sports Medicine recommended that adults older than 18 years should be engaged in moderate physical activity at least 30 min per day.28 Following this recommendation, the British NICE and National Health Service (NHS) initiated health promotion interventions that aimed to increase the level of physical activity by facilitating access to leisure community centres.3 Such activities include community-based programmes for walking and cycling, pedometers and exercise on referral schemes.32 As mentioned in the ‘Introduction’ section, similar schemes have been developed in Sweden, Denmark, Finland and the Netherlands based on the same motivation, namely to increase physical activity among adults with a sedentary lifestyle.7 ,33 ,34 Contrary to the guidelines for developing health promotion interventions, PARS were not developed based on a particular theoretical background but rather on policy recommendations.30 This is one of the reasons that the design, implementation and evaluation differ between countries. Despite those differences, the previous literature has suggested several phases that describe the process of PARS.1 ,2 We present them in table 1.
Description of the PARS
In this study, we focus on the first phase—the design of the PARS programme and on some characteristics related to phases II and III. In particular, we focus on the following characteristics: reasons for referral, who can prescribe PARS, what kind of physical activity can be prescribed, the duration of the programme and patient payments. We also examine the adherence rate and self-reported level of physical activity, related to phase V.
Method
We conducted this review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) strategy.
Inclusion and exclusion criteria
We included studies that meet the following criteria:
Studies with the following designs-RCT, prospective longitudinal studies, cohort studies, mixed design and qualitative studies that examine PARS.
Studies that use as a population group adults older than 18 years.
Studies published in peer-reviewed journals in the English language after 2000.
Studies that report one of the following outcome measures: adherence rate and self-reported physical activity level.
We excluded studies that use PARS participants to check new theoretical approaches or check psychometric characteristics of instruments.36 We also excluded studies that are literature reviews. Also, we excluded studies that use data from other studies to model cost-effectiveness and studies that have been published as a report, opinion papers or national guideline. We also excluded studies that examine PARS characteristics from the physician's perspective. Furthermore, we excluded studies that just describe the design of the RCT related to PARS before those RCTs are conducted.
Searching strategy, study selection and data extraction
Relevant studies were collected using PubMed and EBESCO. For the identification of key words, we followed the strategy proposed by Pavey et al.25 The strategy is based on a scope research to identify relevant synonyms for PARS and then the synonyms were combined with the term primary care. We performed the literature search within both databases using the following chain of key words (the same chain is used in Pavey et al25): “((((exercise on referral) OR physical activity on prescription) OR exercise on prescription) AND primary care”.
An initial search within PubMed identified 669 studies. Applying filters for year of publication, population characteristics and language of publication, 556 studies were included. After checking the titles and abstracts, 69 studies that address PARS were identified. Among them, 8 were excluded as opinion papers,37–44 4 as literature review,4 ,25 ,45 ,46 4 were excluded because they only reported on the design of RCT studies (protocol),15 ,28 ,47–49 3 were excluded as reports,9 ,50 ,51 and 8 were excluded because they examined the physician’s opinion about PARS.52–59 After checking for the last inclusion criteria, nine were excluded.3 ,24 ,27 ,60–64 Through PubMed we identified 27 studies1 ,5 ,6 ,8 ,10 ,12 ,13 ,17 ,19–22 ,26 ,32 ,33 ,65–76 that satisfied all inclusion criteria and were in accordance with the exclusion criteria. We also performed a search using EBASCO (it includes also SocINDEX), and we identified 99 studies. Among them, 14 studies met the inclusion criteria. However, those studies were already identified via PubMed.
Besides the chain proposed by Pavey et al,9 ,25 we also performed a search using the chain of key words that incorporated all synonyms that we identified and that were related to PARS.
“((((((exercise on referral) OR physical activity on prescription) OR exercise on prescription) OR medicine is exercise) OR green prescription) AND health promotion) AND primary care”.
We also searched the databases PubMed and EBASCO using the second chain of key words that incorporate all synonyms that we have identified and that are related to PARS. Again, we were able to identify only 27 studies. After the initial selection of studies, we also checked their reference lists for additional literature. A publication from the reference list (bibliography) is included in the review after applying the same inclusion and exclusion criteria. Furthermore, we also did a forward-search by finding the authors who cite the included papers. For this purpose, we used Google Scholar. Also, we used literature review studies to check whether we include studies that have been identified in previous literature reviews. We did this in order to decrease publication bias.25
Through this additional search, we identified 10 additional studies that met our inclusion criteria.7 ,11 ,14 ,18 ,23 ,34 ,77–80 In total, we included 37 studies (see figure 1). The full strategy for PubMed is available in online supplementary files (see PubMed_searching_strategy).
supplementary data

Meta-analyses of adherence rate level among PARS participants. PARS, physical activity on prescription schemes.
Data extraction and analyses
Because we included studies with different designs, heterogeneous sample types and size and different outcome measures, we first extracted the data related to the characteristics of the included studies.31 Those were aims of the studies, designs of the studies, sample characteristics, response rates, follow-up periods, methods of data collection within the studies, primary and secondary outcome measures, and analyses applied, reported adherence rates and reported levels of physical activity. Those data are presented in detail in online supplementary appendix 1. We also used summary statistics to present some of those characteristics (see the ‘Results’ section, table 2).
Findings related to study characteristics
supplementary appendix
Data related to the design of PARS programmes include reasons for referral (such as sedentary behaviours or type of chronic disease), who can prescribe PARS (GP or other health professionals), where PARS is conducted (in a community leisure facility or at home), duration of the programme (number of weeks), type of physical activity that is applied (aerobics, swimming, walking, etc), participants costs and country where the programme is conducted were also extracted.22 Those data are also presented in the ‘Results’ section (table 3).
PARS characteristics in different countries
We also reported adherence rate and self-reported level of physical activity as measures of effectiveness. Adherence is defined as the patient's active choice to follow the medical recommendation instead of passive compliance. Adherence level is reported in almost all studies as the proportion of people who adhere to more than 80% of all PARS activities. After the PARS has ended, the adherence rate is measured as the proportion of people who continue with physical activity. The self-reported level of physical activity score is obtained from the 7-day Physical Activity Recall (PAR) questionnaire. It is measured at the beginning of PARS and after a certain period of time.
Furthermore, we evaluate the quality of the included studies using EPHPP ‘Quality Assessment Tool for Quantitative Studies’.81 This tool allows us to estimate three different quality categories: strong, moderate and weak quality. Also, we use the questionnaire suggested by Smith et al,82 which allows us to calculate a study quality score. The quality score is calculated as the percentage of total yes answers for each question.
Effect size calculation and meta-analyses
After the literature review, we performed a meta-analysis using the data from the different studies in the literature review. Meta-analysis is a two-stage process where effect size measures are first calculated for each of the included studies and then the weighted average of the effect size measure is estimated across the studies.31 Effect size measures include different statistics such as the coefficient of correlation and OR. In this study, we calculated two effect size measures. The first effect size measure was the difference in the proportion of people who adhere to physical activity after PARS and those who do not adhere. The most informative way is to compare individuals who adhere in the intervention group with those who adhere in the control group.1 However, in this study, we also included studies with a prospective design that follow the same group of individuals at different time points. In that case, we have compared the adherence rate of the same group of individuals after a certain period of time. To calculate the effect size based on the differences in proportions, we used the formula suggested by Field and Gillett.31 In case the adherence rate, after PARS is over, is reported at two moments—for example the proportion of people who continue with physical activity after 6 months and after 12 months—we used the adherence rate reported for the longer period of time. Some studies considered the intake rate—the proportion of people who are referred to PARS as a baseline adherence rate.22 In case the adherence rate was not reported, we also extracted baseline adherence. This means that we calculate the effect size measure as the standardised difference between the proportion of those who adhere (continue) with physical activity after finishing the PARS programme and the level of physical activity before the PARS programme. If information on physical activity before the programme was not available, we used information on the level of activity during the programme. In case the standardised difference is positive, we conclude that PARS had a positive effect on adherence. Additionally, we performed a meta-analysis including only the studies with a randomised clinical trial and compared the adherence rate of the intervention group with the adherence rate of the control group (see online supplementary appendix 2).
supplementary appendix
The second effect size measure was the standardised difference between the means in the level of the self-reported physical activity score at the beginning of PARS and after a certain follow-up period. This effect size measure is known as Cohen's d, and it is calculated based on the equation reported in other studies.31 In case the SD or mean was not reported, we calculated it from the CI. Also, when mean and SDs were reported for different subpopulation groups within the same study, we summarised results across all groups in accordance with reported standards.83 We analysed the data using a random-effect meta-analyses approach.31 By using a random-effect model, we took into account between and within study variance. For each effect size measure, we ran separate meta-analyses using the METAN command in STATA (Harris R, Bradburn M, Deeks J, et al. METAN: Stata module for fixed and random effects meta-analysis. Statistical Software Components 2010).
After the meta-analyses, we also performed meta-regression. We used each effect size measure as a dependent variable. As a covariate, we included a binary indicator whether the study originates from Australia, Canada, New Zealand, the USA or Europe. We used European countries as a reference category. Also, as a covariate, we included the follow-up period reported in the study. The follow-up period can influence the adherence rate: the adherence rate is lower with a longer follow-up period.25 ,83 We also included three binary indicators related to the main reasons for referral: sedentary lifestyle, having cardiovascular diseases, having diabetes and being overweight/obese. Previous studies have shown that the reason for referral can decrease the adherence rate among population groups such as overweight individuals.9 ,25 It is also known that a longer duration of PARS programme can improve the level of physical activity among participants. At the same time, a longer duration is associated with a lower adherence rate. Therefore, we also included programme duration as a covariate. The study quality score was also included as a covariate, since the quality of the study can influence both measures of effectiveness. We used a random-effect meta-regression. Heterogeneity between the studies was measured through the I2 statistic (with a value higher than 75% considered as large). The proportion of between study variance explained by the model is calculated through tau2 (Harris R, Bradburn M, Deeks J, et al. METAN: Stata module for fixed and random effects meta-analysis. Statistical Software Components 2010). Those results are presented in the ‘Results’ section (table 4).
Results from meta-regression using difference in proportion of adherence rate
Because we included studies with different characteristics—different study designs, sample sizes and applied methods—publication bias might be expected. To assess publication bias related to self-reported levels of physical activity (the standardised differences of two means), we used the Eggers test.84 This test measures the funnel plot asymmetry using linear regression in which standardised effect size measures (effect size divided by its own SE) is regressed against its precession (the inverse of effect size SE). If the intercept in this regression is significantly different from zero, this means that publication bias is present.
To assess publication bias related to the adherence rate as effect size (the difference between two proportions), we used the Begg and Mazumdar's rank correlation tests—a rank order correlation between the standardised effect size measure and its precession.
Results
Table 2 presents the characteristics of the included studies. The majority of the studies originate from the UK—13 (35.2%), while Canada, Denmark, Spain and the USA and are represented by 3 (8.1% of total included) studies. RCT as a study design is used in 24 (64.8% of the 37 included) studies. The average follow-up period in the included studies is 6 months. Only 16 (43.2% of included studies) studies report measures related to physical activity while the adherence rate is reported in 30 (81.1% of included studies) studies.
Table 3 presents the results related to the programme design in different countries. The duration of the programme varies per country. In Sweden, there is no limitation on programme duration, while in the UK the duration of the programme is the shortest and ranges from 8 to 16 weeks, and in Spain it is the longest ranging until 6 months. In all countries, the main reason for referral is a chronic disease and sedentary lifestyle. In Canada, the USA and Sweden, the programme is delivered as a facility based and a home-based activity whereas in other countries it is exclusively a facility-based and supervised activity. GPs are most often the prescribers (62%), although other health professionals are also included.
The results of the meta-analyses are presented in figures 1 and 2. The difference in the pooled adherence rate measured at the beginning of the PARS programme and the adherence rate measured after the PARS programme was 17% (95% CI 9% to 24%). The difference in the pooled physical activity measured by 7-day PAR at the beginning of PARS and after a certain follow-up period was 0.93 unit score (95 CI −3.57 to 1.71).
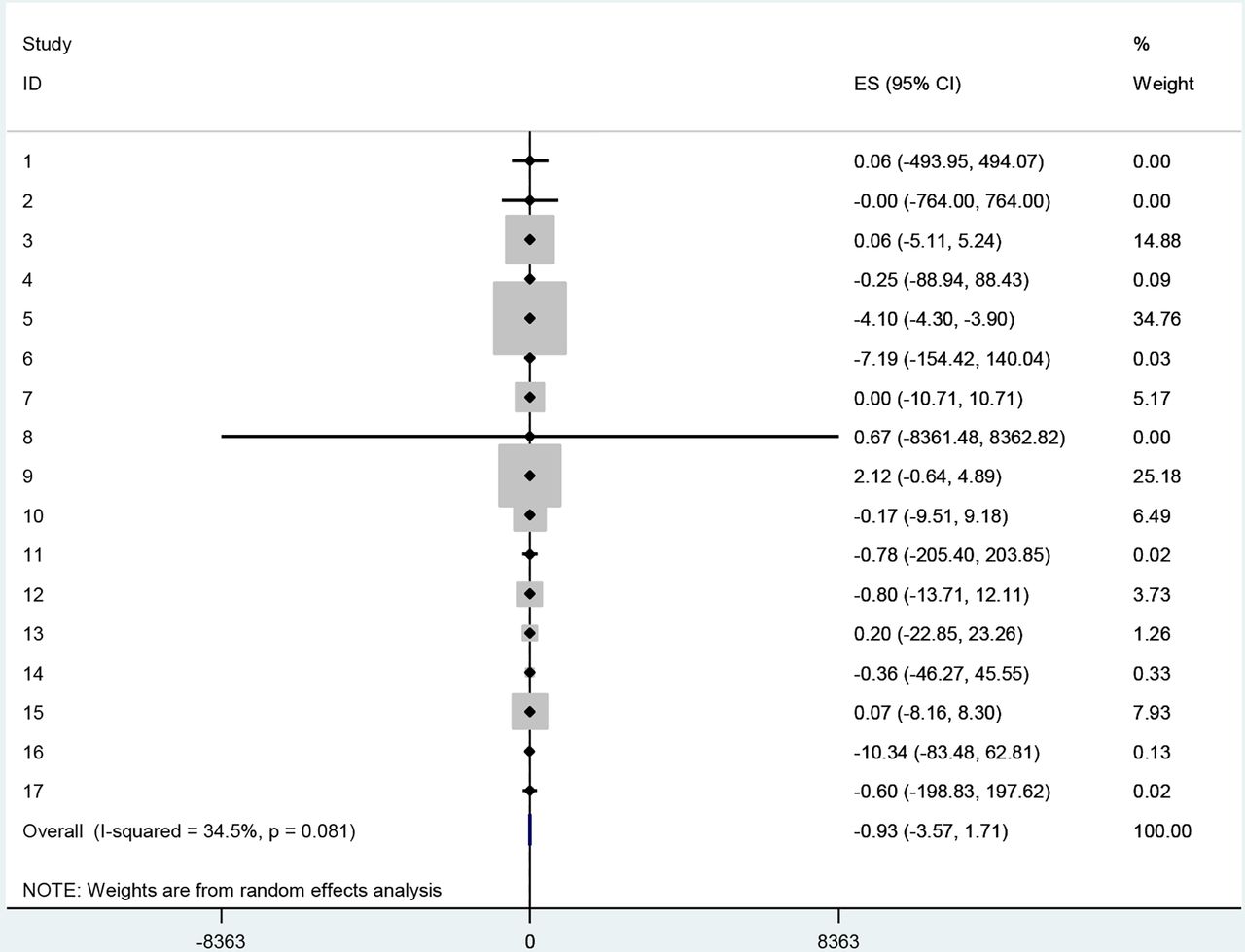
Meta-analyses of physical activity level among PARS participants. PARS, physical activity on prescription schemes.
Table 4 presents the results of the meta-regression with the adherence rate as the dependent variable. The results show that the effectiveness of PARS on the adherence rate is associated with the duration of the treatment. Furthermore, studies that include participants diagnosed with a sedentary lifestyle and diabetes also report a higher adherence rate. Obesity and cardiovascular diseases are not associated with a higher adherence rate. Studies that come from Australia, Canada and the USA have a lower effectiveness in increasing the adherence rate than studies originating from Europe.
Figure 3 presents the results from risk bias Begg and Mazumdar's rank correlation tests. Tests show that there is no correlation between the standardised effect size measure (difference in proportion related to adherence rate) and its precession. In other words, a test shows that there is no publication bias effect for this effect size measure.

{kind=link}
{kind=link}
{kind=link}
Funnel plot of effect size versus SE (random effects model).
Table 5 presents the results from Eggers test.84 The results of the Egger test show that publication bias is present (p<0.06).
Egger's test
Discussion
Our results from the literature review show that characteristics of the PARS programme are associated with self-reported levels of physical activity. For example, a longer duration of the PARS programme in some parts of the UK is associated with a higher level of self-reported physical activity (see online supplementary appendix 1). Studies included in this literature review show the large heterogeneity in design characteristics between countries. The main differences are related to the duration of the programme, reasons for referral and patient payments. One explanation for this can be the different positions that primary healthcare providers have within healthcare systems. It is also seen that PARS characteristics such as charges participants have to pay depend on the policy design of PARS. These differences are also observed within countries. One example is the duration of the programme: in the UK, it can take 8 but also 26 weeks. Those variations are related to the UK national policy that tries to embed PARS within the local community, and therefore each community can design its own interventions. Results from a previous literature review suggest that the effectiveness of PARS increases with the duration period.46 However, results related to meta-regression in this study show that the duration of the programme is not related to the adherence rate.
Another peculiarity of the design of PARS programmes is that in some countries, health status is not the only reason for referral but sociodemographic characteristics play a role as well. This is, for example, the case in the Netherlands where PARS is adapted to minorities and in Canada where particular attention is paid to women. Our results related to the literature review and different programme characteristics show that heterogeneity in the target groups for the PARS programme can lead to bias in the estimate of effectiveness. Publications that target particular groups with a unique reason for referral report greater effectiveness of PARS than publications that include heterogeneous groups of participants. Although PARS is intended to provide better access to physical leisure centres for certain population groups, small fees that are charged in some countries do not affect financial accessibility (see online supplementary appendix 1 and table 3). This is observed in the Netherlands, the UK and Sweden. In the Netherlands, PARS participants pay a small fee of ∼21 euro, but if they participate in more than 80% of the meetings, they receive 10 euro back. In this way, small fees are used to increase the intrinsic motivation and consequently influence adherence among the participants. However, those observations are based on the literature review. The information regarding patient payments are not included in meta-regression. Furthermore, some studies from the literature review report that the lack of time is more important for the success of PARS than the participation fee. This is of particular importance for middle-aged adults and female participants.21 ,22 ,85 One way to save the invested time is the implementation of the programme in a home-based environment such as walking programmes in Sweden.21
The importance of design characteristics for the effectiveness of PARS programmes is also confirmed in the meta-regression. We were able to apply meta-regression using the difference in the adherence rate as an outcome measure since only 17 publications report the level of physical activity at different points in time. Although the basic meta-analyses show positive effects of PARS on self-reported level of physical activity, those results are limited by the low number of included studies and the short follow-up period. Our results on the adherence rate show that a longer follow-up period is associated with greater effectiveness. From the perspective of participants, the follow-up period is seen as a continuation of the programme, since during this period they stay in touch with healthcare professionals and other participants. Furthermore, the reason for referral also plays a role in the effectiveness of PARS related to the adherence rate. While some reasons for referral like diabetes mellitus are positively associated with an increased adherence rate, others like being obese are not. This is of particular importance since obese people represent one of the main target groups for PARS. One of the explanations is that the lack of self-esteem among obese people is a barrier to participate in group activities.
Findings from this study are in accordance with previous studies.9 ,86 However, this study goes one step beyond that. It shows that the effectiveness of the PARS programme should be evaluated taking into account specific dimensions of design and implementation. For example, providing access to a physical leisure centre is important but not a sufficient step to increase physical activity. Even, with tailor-made programmes, targeting specific population groups such as women and older adults is just one step in providing a successful programme. Other steps include making a difference between diagnostic categories. Although the main purpose of the programme was to target people with a sedentary lifestyle and obesity, it seems that programmes delivered in community leisure centres are not effective for those groups. Results from Sweden where the programme is implemented in home surroundings and from the Netherlands where the programme addresses specific cultural needs of participants provide more successful stories than PARS programmes which include different population groups with different reasons for referral and different sociodemographic characteristics.12 ,19 Also, a distinction should be made in recommendations about PARS programmes for people diagnosed with certain diseases. For example, in this study, we include publications on the evaluation of PARS programmes among patients with cancer and stroke, although such programmes are rather rare. The evaluation of PARS programmes applied to those specific groups should be different from the evaluation of PARS programmes applied as a prevention strategy for a more general population.
Our results are bounded by certain limitations. One of the limitations of this study is that only one person was involved in the study selection and data extraction. The majority of the studies included in the literature review come from English-speaking countries with RCT as the dominant research design. An exception is Sweden, where the majority of the studies are based on a longitudinal prospective design.19 ,20 ,33 RCT is the most prevalent study design reported in 65% of the publications included in this study. Although RCT is considered to be a ‘golden standard’ in the evaluation of health promotion interventions, it is frequently limited by a short-time follow-up period. In this study, the average reported follow-up is 6 months. Previous studies have already outlined that the effectiveness of health promotion programmes that aim to change participants’ behaviour should be examined over a longer period of time.25 Quasi-experimental designs within RCT also prevent the examination of the effectiveness of PARS in real circumstances.22 Another limitation of this study is related to the reported outcome measures. We have focused in particular on the adherence rate and on self-reported physical activity. Adherence to the prescribed programme and the self-reported level of physical activity are complex and, to some extent, arbitrary concepts. Adherence to the prescribed programme is also related to information that the patient has about the programme, the perceived benefits from the programme, patient characteristics, social support and relation with the health professionals.87 ,88 The self-reported level of physical activity is also a subjective measure that depends on the participant's perception.45 Another limitation is related to high heterogeneity in effect size measures. When we used the adherence rate as an effect size measure, heterogeneity among the studies was high. In order to address this, we applied a random-effect model. Heterogeneity in effect size may have different causes. We explored whether this heterogeneity was related to the design of the study, the length of the follow-up period or the country where the study was conducted. We performed meta-analyses using only studies with a randomised design, studies with a programme duration longer than 12 weeks and studies using data from Europe. Only when the duration of the programme was longer than 12 weeks, heterogeneity was lower. On the basis of these results, it is likely that different factors cause heterogeneity in effect size. Furthermore, evaluation of health promotion programmes should also include cost-effectiveness measures.26 This was not possible since only studies from the UK report on the cost-effectiveness of PARS, calculated from a societal perspective.
Conclusions
For the future evaluation of PARS programmes, more objective measures that include longer follow-up periods should be included. Furthermore, the evaluation of the programme should be compared with programmes with similar designs taking into account the included target population and reasons for referral. Including information related to participants’ direct and indirect costs (travel costs) should also improve the quality of the evaluation process.
For the PARS programme, targeting particular groups, taking into account their preferences and providing programmes during a longer period of time even with small participants fees, seems to lead to greater effectiveness of the programme than implementation within a general population group.
References
Footnotes
Contributors JA developed the study design, carried out the literature search and analysis, drafted and improved the manuscript, approved the final version and agreed to be accountable for her contribution. WG contributed to the development of the study design, reviewed the literature search and analysis, reviewed and commented on the preliminary drafts and final version of the paper, approved the final version and agreed to be accountable for his contribution.
Funding This paper arises from the project Pro-Health65+, which has received funding from the European Union, in the framework of the Health Programme (2008–2013).
Disclaimer The content of this paper represents the views of the author and it is his sole responsibility; it can in no way be taken to reflect the views of the European Commission and/or the Executive Agency for Health and Consumers or any other body of the European Union. The European Commission and/or the Executive Agency do(es) not accept responsibility for any use that may be made of the information it contains.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data are available by emailing: j.arsenijevic@maastrichtuniversity.nl