Article Text

Abstract
Purpose This cohort study was established to investigate the effects of unilateral and bilateral oophorectomy on the ageing processes in women.
Participants We used the records-linkage system of the Rochester Epidemiology Project (REP, http://www.rochesterproject.org) to identify 570 women who underwent unilateral oophorectomy and 1653 women who underwent bilateral oophorectomy in Olmsted County, Minnesota from 1988 through 2007 (20 years). Each woman was matched by age (±1 year) to a population-based referent woman who had not undergone any oophorectomy (570 referent women) or bilateral oophorectomy (1653 referent women). These four cohorts are being followed to assess morbidity and mortality and to study imaging and biological markers related to ageing.
Findings to date An extensive medical record abstraction using the REP has been completed for each woman to obtain demographic, reproductive and adult life characteristics and extensive clinical information about the surgical procedure and subsequent oestrogen replacement therapy (or other sex steroid therapy). The cohorts have been used to date to study the accumulation of multiple chronic conditions following bilateral oophorectomy in women with or without chronic conditions at the time of the oophorectomy (or index date). From the cohorts, we have also derived a sample of 128 pairs of women for a case–control study linking adverse childhood or adult experiences to the risk of bilateral oophorectomy.
Future plans We hypothesise that the abrupt hormonal changes caused by bilateral oophorectomy in younger women have a major effect on the ageing processes across the full body. Therefore, we plan to investigate the risk of a wide range of chronic conditions following bilateral oophorectomy. Specific studies are underway for kidney diseases, psychiatric diseases and neurological diseases. In addition, we plan to invite a subsample of women from the bilateral oophorectomy cohort to participate in an in-person study involving brain imaging and the collection of biomarkers.
- unilateral oophorectomy
- bilateral oophorectomy
- cohort study
- aging
- morbidity
- mortality
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The four cohorts of women in the Mayo Clinic Cohort Study of Oophorectomy and Aging-2 are population-based and nested within a medical records-linkage system.
Possible recall bias and left censoring of information are minimised by design because all data were obtained from medical records included in a records-linkage system.
Participation was high (approximately 97%) because almost all women gave general authorisation to use their medical records for research, and all women were included regardless of socioeconomic status, insurance status and healthcare delivery setting.
When detecting chronic conditions using diagnostic codes, we may have undercounted or misclassified certain conditions that did not receive adequate coding as part of routine medical care.
Our study involved oophorectomies that occurred over 20 years, and the surgical and medical practices have changed over time.
Introduction
Since 2001, our group has worked extensively on a cohort study that we will refer to as the Mayo Clinic Cohort Study of Oophorectomy and Aging-1 (MOA-1) addressing the long-term outcomes among women who underwent unilateral or bilateral oophorectomy in Olmsted County, Minnesota from 1950 through 1987. Several publications have reported the key findings regarding morbidity and mortality after oophorectomy.1–7 However, the MOA-1 study had some important limitations. First, the information about medical conditions present at the time of oophorectomy was limited for both women with oophorectomy and referent women. Second, the timing of oophorectomy in relation to menopause remained uncertain for some women, and the information about hormonal treatment after oophorectomy was limited. Third, the medical records of referent women were not abstracted systematically to obtain detailed demographic, social, reproductive, familial and adult life characteristics. Finally, the oophorectomies occurred from 1950 through 1987, reflecting the surgical and medical practices of that period; therefore, the findings may not apply directly to more recent practices.
To address the limitations of the MOA-1 study and to provide an independent replication of our findings in a more recent sample, we established the MOA-2 study that is described in this publication. The overall aim of this profile is to describe the demographic and clinical characteristics of the women who underwent unilateral or bilateral oophorectomy in MOA-2 (we will use the term surgery to indicate either unilateral or bilateral oophorectomy). Analyses related to some outcomes of the MOA-2 study have been reported elsewhere,8 9 and extensive additional analyses will be reported in future articles. MOA-2 is long-term and involves a broad range of outcomes across multiple areas of medicine (eg, cardiology, nephrology, neurology and psychiatry). In addition, MOA-2 should contribute greatly to ageing research.
Cohort description
Composition of the four cohorts
Figure 1 shows the timeline of the MOA-1 and MOA-2 studies in terms of recruitment of incident surgeries and length of follow-up. MOA-1 included both a cohort of women who underwent unilateral oophorectomy and a cohort of women who underwent bilateral oophorectomy from 1950 through 1987 and two corresponding cohorts of age-matched referent women. The follow-up so far is through 2014 (possible follow-up of 27 to 64 years). MOA-2 included both a cohort of women who underwent unilateral oophorectomy and a cohort of women who underwent bilateral oophorectomy from 1988 through 2007 and two corresponding cohorts of age-matched referent women. The follow-up so far is through 2014 (possible follow-up of 7 to 26 years; figure 1). All four cohorts were representative of the geographically defined population of Olmsted County, Minnesota (USA). All data collection was through the records-linkage system of the Rochester Epidemiology Project (REP) that has been described extensively elsewhere.10–13 In brief, the REP covers the entire population of Olmsted County since 1966 (approximately 69 000 women in 2010).12 Although the MOA-1 cohorts are more mature, the MOA-2 cohorts are more informative because they have more complete documentation.
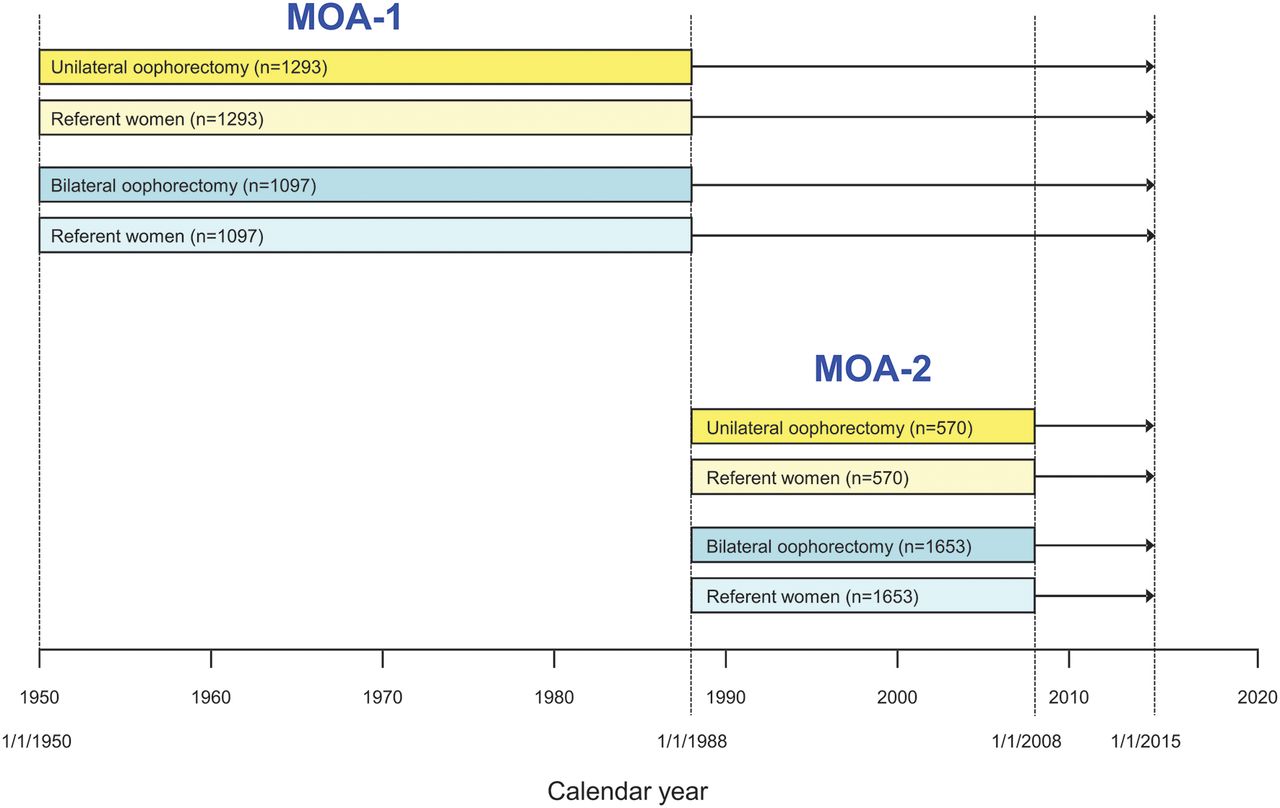
Time frame of the Mayo Clinic Cohort Study of Oophorectomy and Aging-1 (MOA-1) and of the Mayo Clinic Cohort Study of Oophorectomy and Aging-2 (MOA-2, current study) as of 31 December 2014 (time used in the most recent published analyses). Passive follow-up through the Rochester Epidemiology Project records-linkage system is available for women in the MOA-1 cohorts through 31 December 2014; however, the published papers refer to a shorter follow-up (eg, staggered contacts from 2001 through 2006).1–7 We plan to continue to follow the women in MOA-2 in the future.
We used the electronic indexes of the REP to identify women who received a procedure code from the International Classification of Diseases, ninth revision (ICD-9) for either unilateral (65.3x and 65.4x) or bilateral (65.5x and 65.6x) oophorectomy between 1 January 1988 and 31 December 2007. The complete medical records of all of these women were reviewed by a physician (LGR) or a trained study nurse to abstract details about the surgery and about the pathology of the ovaries removed. The final classification of women by oophorectomy status was based on the findings at medical record review.
Unilateral oophorectomy study
We included women who underwent unilateral oophorectomy before the onset of menopause and before reaching age 50 years, regardless of a possible concurrent or prior hysterectomy. However, we excluded women who underwent unilateral oophorectomy before the age of 10 years, for ovarian cancer (primary or metastatic), or for the treatment of another oestrogen-sensitive malignancy (usually breast cancer), and women with a high risk of ovarian cancer as judged by the gynaecologist or confirmed by genetic testing. Women with an ovarian cancer unrecognised at the time of the surgery but discovered at pathological examination were included. For each woman included in the unilateral oophorectomy cohort, we defined the date of the surgical procedure as the index date, and we selected via simple random sampling a woman from the Olmsted County population who was born in the same year (±1 year) and had not undergone unilateral or bilateral oophorectomy before the index date. All women who met these criteria were considered eligible regardless of menopausal status, of any existing chronic condition or risk factors and of prior hysterectomy. Potential referent women who underwent unilateral or bilateral oophorectomy after the index date are included in our primary analyses of outcomes but are censored at the surgery date in sensitivity analyses. In addition, because of the historical recruitment of the cohort, women were allowed to be included in both the oophorectomy and the referent cohort if they met the inclusion criteria. Figure 2 shows a flow chart of the inclusion of women in the unilateral oophorectomy and referent cohorts and of the follow-up through 2014.

{kind=link}
{kind=link}
Flow chart of the four MOA-2 cohorts as of 31 December 2014 (time used in the most recent published analyses): (1) women who underwent unilateral oophorectomy and (2) their corresponding matched referent women; (3) women who underwent bilateral oophorectomy and (4) their corresponding matched referent women. *A total of 72 women with unilateral oophorectomy had subsequent removal of their remaining ovary before age 50 years from 1988 through 2007, and were included both in the unilateral oophorectomy cohort and in the bilateral oophorectomy cohort. †Causes of death are available for 15 of 16 deceased women with unilateral oophorectomy, for 11 of 16 deceased matched referent women, for 57 of 64 deceased women with bilateral oophorectomy and for 54 of 60 deceased matched referent women. ‡Survivors were followed up to the most recent contact with the system or to 31 December 2014. ¶Women lost to follow-up did not receive care within the system during the last 3 years of study (1 January 2012 to 31 December 2014) and were censored at the last recorded contact. We plan to continue to follow the women in MOA-2 in the future. ICD-9, International Classification of Diseases, ninth revision.
Bilateral oophorectomy study
We included women who underwent bilateral oophorectomy or a second unilateral oophorectomy before the onset of menopause and before reaching the age of 50 years, regardless of a possible concurrent or prior hysterectomy. Although hysterectomy results in the cessation of menses, sometimes referred to as surgical menopause, and may shorten the time to ovarian insufficiency,14–16 women who underwent prior hysterectomy with ovarian conservation were included because hysterectomy was not considered an immediate cause of ovarian insufficiency. However, we excluded women who underwent oophorectomy before the age of 10 years, for ovarian cancer (primary or metastatic) or for the treatment of another oestrogen-sensitive malignancy (usually breast cancer), and women with a high risk of ovarian cancer as judged by the gynaecologist or confirmed by genetic testing. Women with an ovarian cancer unrecognised at the time of the surgery but discovered at pathological examination were included. Age-matched referent women who had not undergone bilateral oophorectomy before the index date (date of bilateral oophorectomy in the matched woman) were randomly selected from the same Olmsted County population, regardless of menopausal status, of any existing chronic condition or risk factors, of prior hysterectomy and of prior unilateral oophorectomy. Potential referent women who underwent bilateral oophorectomy after the index date are included in our primary analyses of outcomes but are censored at the surgery date in sensitivity analyses. In addition, because of the historical recruitment of the cohort, women were allowed to be included in both the oophorectomy and the referent cohort if they met the inclusion criteria. Figure 2 shows a flow chart of the inclusion of women in the bilateral oophorectomy and referent cohorts and of the follow-up through 2014.
Validity of the surgical codes in the REP
Of 1739 surgeries coded as bilateral oophorectomy, 16 (0.9%) were found at record abstraction to have been unilateral rather than bilateral oophorectomy. Similarly, of 625 surgeries coded as unilateral oophorectomy, four (0.6%) were found at record abstraction to have been bilateral rather than unilateral oophorectomy, and 58 (9.3%) were found at abstraction to have been a second unilateral oophorectomy. All women who were erroneously coded were assigned to the appropriate cohort. A total of 72 women with unilateral oophorectomy had subsequent removal of their remaining ovary before age 50 years from 1988 through 2007 and were thus included in both cohorts.
Of 1686 women who were considered as candidate referent women for the bilateral oophorectomy cohort study, 33 (2.0%) were excluded because they were found at record abstraction to have undergone bilateral oophorectomy outside of the REP system before the index date (negative predictive value=98.0%). Similarly, of 576 women who were considered as candidate referent women for the unilateral oophorectomy cohort, only six (1.0%) were excluded because they were discovered to have undergone unilateral or bilateral oophorectomy outside of the REP system before the index date (negative predictive value=99.0%).
Characteristics present at or before the surgery or the index date
A physician (LGR) and a trained nurse abstractor reviewed the complete medical records of all women who received a surgical code for unilateral or bilateral oophorectomy. For those women confirmed to have undergone surgery, detailed information about surgical characteristics was abstracted (eg, indication for the surgery, pathology of the removed ovaries and pathology of the removed uterus, if applicable). In addition, for women both with and without oophorectomy, an extensive series of demographic, social, reproductive and adult life characteristics and information about family history of cancer were abstracted and recorded using an electronic data entry application. The application provided real-time data checks (eg, range of valid values), and comprehensive data checks were performed regularly during abstraction. To increase the consistency of the data collected, the two data abstractors followed a manual of instructions providing definitions and examples for the variables of interest, with iterative updates based on use. In this profile, we report a series of analyses pertaining to characteristics present at or before the surgery or index date that have not been previously published. Women had a median of 22.8 years of medical record information before the index date (interquartile interval, 10.9–34.1).
Table 1 shows the distributions of demographic and social characteristics for our four MOA-2 cohorts at surgery or index date. Women who underwent unilateral oophorectomy were younger (60.2% <40 years) than women who underwent bilateral oophorectomy (20.8% <40 years). Interestingly, 17.0% of women underwent unilateral oophorectomy before age 30 years. Women who underwent either unilateral or bilateral oophorectomy had fewer years of education than referent women. In addition, women who underwent bilateral oophorectomy were more commonly white than referent women of the same age. However, the numbers for non-white women were small (table 1).
Demographic and social characteristics of women who underwent unilateral or bilateral oophorectomy and their matched referent women
Table 2 shows the surgical characteristics and the findings at pathology of the women who underwent unilateral or bilateral oophorectomy. In the unilateral oophorectomy cohort, the right and left ovaries were removed with similar frequency, and the most common condition cited as the indication for oophorectomy was a benign tumour (59.5%) followed by a cyst or endometriosis (25.6%). However, 10.7% of the women did not have any specified ovarian condition (no ovarian indication). A previously unrecognised ovarian cancer was found at pathological examination of the ovary removed in 11 women (1.9%). For approximately half of the women (46.5%), the unilateral oophorectomy was performed in conjunction with hysterectomy (or after a prior hysterectomy), and the most common indication for the concurrent hysterectomy was bleeding (21.8%) followed by pain (18.8%). The most common pathology of the removed uterus was fibroids or polyps (21.9%) followed by normal pathology (11.8%).
Surgical characteristics and findings at pathology of women who underwent unilateral or bilateral oophorectomy
In the bilateral oophorectomy cohort, most of the women had both ovaries removed at the same time (90.9%), and the most common indication listed in the medical record was a benign tumour (23.1%) followed by a cyst or endometriosis (17.2%). However, 59.2% of the women did not have any specified ovarian condition (no ovarian indication). Women without a benign ovarian condition were historically considered to have ‘prophylactic’, ‘elective’ or ‘incidental’ bilateral oophorectomy. Interestingly, a previously undiagnosed (or unsuspected) ovarian cancer was found at pathological examination of the ovaries removed in 25 women (1.5%). For almost all women (98.5%), bilateral oophorectomy was performed in conjunction with hysterectomy (or after a prior hysterectomy). The most common indication for concurrent hysterectomy was bleeding (50.5%) followed by pain (35.7%). The most common pathology of the removed uterus was fibroids or polyps (56.7%) followed by normal pathology (20.0%).
Variables collected during follow-up
The follow-up of the four cohorts has been completed for a median of 14.2 years (interquartile interval, 9.7–19.2) and is ongoing using both manual abstraction of medical record information and electronic extraction of diagnostic codes stored in the REP indexes. Manual abstraction of medical records was used to collect information about use of oestrogen therapy and other sex steroid therapies during follow-up. Details were collected about timing of onset of therapy, dose and route of administration (eg, oral vs transdermal) and duration of use. In addition, manual abstraction was used to document gynaecological surgeries that followed the index date and to collect information about cigarette smoking and timing of menopause or of symptoms of ovarian insufficiency (when applicable) during follow-up. The manual abstraction of medical records was facilitated by using an electronic data entry application and a manual of instructions, as described earlier.
Findings to date
Characteristics present at surgery or index date
An assessment of the most important medical conditions present at the index date in women who underwent bilateral oophorectomy and their matched referent women was obtained using electronic extraction of the ICD-8 or ICD-9 diagnostic codes from the REP indexes. To reduce false-positive diagnoses, we required two diagnostic codes in the same category separated by more than 30 days. For codes before 1994, we required the two codes to be separated by at least 1 year, because the coding was less detailed for that period.17 18 These ICD codes were used to define the 20 chronic conditions recommended by the US Department of Health and Human Services (DHHS) to study multimorbidity.19 20 However, we excluded HIV infections, autism spectrum disorders and hepatitis from the DHHS list and added anxiety disorders as detailed elsewhere (total of 18 selected conditions).17 18 21 Case–control analyses of the 18 selected chronic conditions present at index date in the bilateral oophorectomy study have been reported elsewhere.8
From the bilateral oophorectomy cohort study, we derived a series of 128 women who underwent oophorectomy (cases) and their corresponding 128 age-matched controls (±1 year) to include in a case–control study. The final sample included all of the 128 matched case–control pairs for which both women had medical record information dating back to age 15 years or earlier. The historical medical records were accessible via the REP. We observed an association of bilateral oophorectomy performed before age 46 years with verbal or emotional abuse, physical abuse, any abuse (verbal or emotional, physical or sexual) and with substance abuse in the household experienced during childhood (before age 19 years). In women who underwent the oophorectomy before age 40 years, we also observed a strong association with prior physical abuse experienced during adulthood.22 23
Variables collected during follow-up
Since the women in MOA-2 were relatively young at the time of the present analyses, the primary outcomes considered so far were related to morbidity. However, with the passage of time, these cohorts will mature, allowing us to study longer-term morbidity and mortality. Our results for medical conditions that developed de novo after oophorectomy or index date have been reported elsewhere,8 9 and additional findings will be reported in future publications. The de novo morbidity that developed after the surgery or index date for a median follow-up of approximately 14 years was obtained from the REP indexes by using electronic diagnostic codes for 18 selected conditions (through 31 December 2014). The rule of two diagnostic codes in the same category over a specified time interval was used for outcome conditions as was used for conditions before the index date. However, if a woman died, one diagnostic code listed anywhere on the death certificate was sufficient (including underlying, intermediate or immediate cause of death and other conditions present at death).1 The time of onset of a given condition was the time when a person received the second of the two codes for the same condition (meeting the time gap criteria outlined above) or the time of death, if the condition was first coded at the time of death.
As of July 2017, two papers were published. In a first paper, bilateral oophorectomy performed before age 50 years was associated with a higher risk of multimorbidity (defined using 18 common chronic conditions),21 even after adjustment for medical conditions present at baseline and for several possible confounders.8 However, the association was reduced among women who received oestrogen therapy after the oophorectomy. The associations were more extreme among women who underwent bilateral oophorectomy before age 46 years.8 The accumulation of multimorbidity is considered a clinical marker of accelerated ageing.8 24 In a follow-up paper, we repeated the analyses after restricting the sample to women who did not have any of the 18 chronic conditions at the oophorectomy or index date.9 Bilateral oophorectomy remained associated with a higher risk of multimorbidity, and the findings were similar for women with or without an ovarian indication for oophorectomy. Our findings provide strong observational evidence that bilateral oophorectomy is causally linked to accelerated ageing.9 24
Future plans for passive follow-up of the bilateral oophorectomy cohort
Women included in the four MOA-2 cohorts have been and continue to be followed passively through the REP records-linkage system.10–13 The data for this cohort were collected and will continue to be collected from two sources: (1) manual abstraction of the complete medical records of all women in the cohort and (2) electronic extraction of diagnostic codes or other variables from the REP electronic indexes. We have collected and will collect both characteristics present at or before the index date and outcomes during follow-up. Our hypothesis is that the abrupt hormonal changes caused by bilateral oophorectomy in younger women have a major effect on the ageing processes across the entire body. Therefore, we plan to investigate the risk of a wide range of conditions across multiple areas of medicine following bilateral oophorectomy.
Specific studies are underway for kidney diseases, psychiatric diseases and neurological diseases. For these studies, we screened the indexes for a broad list of codes to select women for whom a complete medical record abstraction was needed. This two-phase case finding approach allowed for a more precise definition of the outcome diseases and for the use of specified diagnostic criteria.
Given that the practice of prophylactic bilateral oophorectomy in women who do not have a clear indication has become historically accepted and persists despite strong evidence against it, the primary objective of our study is to provide new evidence against the unjustified practice.25–27 However, we will also document outcomes of bilateral oophorectomy that can be interpreted as beneficial such as the reduction of the risk of cancer. For example, in our study of accelerated accumulation of multimorbidity, the risk of cancer of all types was reduced in women who underwent bilateral oophorectomy at age 45 years or younger (the difference was not statistically significant).8
Future plans for in-person follow-up of the bilateral oophorectomy cohort
To better understand the mechanisms linking the abrupt hormonal changes caused by bilateral oophorectomy to accelerated ageing at the cellular, tissue, organ and system level, we plan to add an in-person component to the study. In particular, we will invite a subsample of women from the bilateral oophorectomy cohort and the age-matched referent cohort to participate in an in-person study involving brain imaging and the collection of blood and other tissue specimens to study biomarkers of ageing (eg, DNA methylation, telomere length and mitochondrial function).24 We plan to start the contacts for this in-person study in the second half of 2018, and further details will be provided in future publications.
Because of the recent findings from our case–control study linking bilateral oophorectomy to adverse childhood or adult experiences in a subsample of MOA-2, we plan to expand the medical record abstraction for these variables to all women in the cohort.22 23 We plan to include adverse childhood or adult experiences as possible confounding or effect modifying variables in future analyses.
Future plans for the unilateral oophorectomy cohort
Since the women in the unilateral oophorectomy cohort and the corresponding referent cohort were relatively young at the index date, and the sample size of these two cohorts was smaller than for bilateral oophorectomy, a long-term follow-up is needed for the analyses to have adequate statistical power. In the shorter-term, we plan to use these cohorts to determine whether unilateral oophorectomy with or without hysterectomy may cause an earlier age at onset of menopause (or of ovarian insufficiency for women who also underwent hysterectomy).5 14 28
Outcomes and power considerations
Similar to other projects with a broad research agenda, MOA-2 will support studies in several areas of medicine. The sample size was determined by the size of the population included in the REP, and the time window of recruitment of women was designed to avoid overlap with MOA-1. Therefore, the power to test specific hypotheses varies depending on the outcome of interest. The power will also vary with time; as of 2014, the median follow-up was already longer than 14 years. For some outcomes, we will need to wait for the cohorts to mature. On the other hand, for some projects, we will be able to restrict the sample to a smaller segment of the overall study, as was done for the case–control study of adverse childhood or adult experiences.22
Strengths and limitations
Strengths
Some methodological features distinguish the MOA-2 study from several previous studies that addressed related questions.29–33 First, information about menopause timing and type and about preceding risk factors and conditions present at the index date was abstracted from the medical records included in a records-linkage system. Similarly, the outcome conditions under study and the use of oestrogen or other sex steroid hormones during follow-up were electronically extracted from the REP indexes or manually abstracted from the complete records, without direct involvement of the women included in the study. By avoiding the self-report of past events by the women, recall bias was minimised. In addition, access to decades of historical medical records before the index date eliminated the need to rely on the often limited information recorded by the treating surgeon at the time of the oophorectomy.
Second, women were followed continuously both before and after the oophorectomy or index date. Therefore, there was no time gap between the oophorectomy and recruitment into the study (left censoring was minimised by design). Third, because the data collection was historical, women did not need to provide a study-specific informed consent but only a general research authorisation (as per Minnesota legal requirements), thus minimising non-participation (approximately 97% participation of women in the REP).11 12 By contrast, the planned future studies involving the in-person participation of a subset of women will require signed informed consent.
Fourth, our referent women comprised a population-based sample rather than women who underwent hysterectomy with ovarian conservation.29 30 We chose not to use hysterectomy with ovarian conservation as a referent group because hysterectomy itself may modify the risk of morbidity and mortality.8 14 28 31 34 Fifth, information about the use of oestrogen, progestogens, testosterone or other sex steroid therapies was based on written prescriptions and clinical notes about use (rather than simply on pharmacy records of dispensed medicines). Sixth, our cohorts included all age and race/ethnicity groups regardless of socioeconomic status (SES), insurance status and healthcare delivery setting.12 Finally, comparative analyses of results from MOA-1 and MOA-2 may be useful to address the effects of birth cohort and of changes in surgical practice (eg, type of surgery or anaesthesia) or changes in clinical practice (eg, dose and route of hormonal administration).
Limitations
First, the oophorectomies used to define our cohorts took place over 20 years, from 1988 through 2007, and surgical practices and oestrogen use have changed over time. Second, our study focused on a single geographically defined US population, and the observed associations may differ in other populations in the USA and worldwide. However, the demographic and socioeconomic characteristics of our population are similar to those of the upper Midwest and of a large segment of the entire US population,13 and replication of this study in other populations in the USA and worldwide will allow for useful comparisons.
Third, in using the REP indexes to detect chronic conditions occurring before or after the index date, we may underestimate the rates of certain conditions that are in early clinical stage or do not uniformly come to medical attention early, such as dementia and cognitive disorders. Fourth, the ICD codes used to define the conditions are assigned during the course of routine medical care and are subject to misclassification. We attempt to reduce the risk of false-positive diagnoses by including only those women who received at least two codes for a given condition separated by more than 30 days, as was done in other studies.18 35
Fifth, women with ovarian cancer discovered only at pathological examination of the removed ovaries were included in the study because undetected ovarian cancer may have occurred also in referent women. Sixth, SES is probably a major confounder in analyses linking bilateral oophorectomy to adverse medical outcomes and multimorbidity. Given that income is not collected by the care providers participating in the REP, in the analyses reported so far, we have adjusted for SES by using race and education.8 9 In future analyses, we plan to consider adding an indirect measure of income to further reduce any residual confounding by SES. We plan to link the address of women at the index date with a census block group in Olmsted County and to impute income using the 2000 US census data. A similar strategy was used in a recent study in the REP.36
Seventh, analyses comparing women with bilateral oophorectomy who received or did not receive adequate hormonal treatment after the surgery may be confounded by conditions that influenced the decision to treat or not to treat (indications and counterindications). In the absence of a randomised study, we will consider these potential confounders in multivariable models.
Finally, we intended to exclude women who underwent bilateral oophorectomy because of high genetic risk of ovarian cancer only when the risk was judged to be high by the gynaecologist or was confirmed by genetic testing. However, in the time period covered by the study, genetic testing was rarely performed; therefore, we cannot exclude that some of the women included did carry one of the known high-risk genetic variants.
Acknowledgments
The authors would like to thank Ms Deborah C Olson for her abstraction of information from medical records and Ms Robin M Adams for her assistance in typing and formatting the manuscript.
References
Footnotes
Contributors WAR, CYS, BRG and LTS were involved in the conception and design of the study. LGR collected a large segment of the data via medical record abstraction. WAR, CYS and BRG conducted the data analyses. WAR drafted the manuscript. All authors contributed to the interpretation of the data and provided critical revisions of the manuscript. All authors also approved the final version to be published.
Funding The MOA-2 study used the resources of the Rochester Epidemiology Project, which is supported by the National Institute on Aging of the National Institutes of Health (grants R01 AG034676 and R01 AG052425). This study was also supported by funds from the Mayo Clinic Research Committee (WAR). WAR was partly supported by the National Institutes of Health (P50 AG044170, U01 AG006786 and P01 AG004875). VMM was partly supported by the National Institutes of Health (P50 AG044170).
Disclaimer The content of this article is solely the responsibility of the authors and does not necessarily represent the official view of the National Institutes of Health.
Competing interests None declared.
Ethics approval All study procedures and ethical aspects were approved by the institutional review boards of both Mayo Clinic and Olmsted Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Investigators interested in using the four cohorts to test specific hypotheses can contact Dr Rocca via email (rocca@mayo.edu). The correspondence should include a brief outline of the intended project (not longer than a page).
Collaborators Information about the Rochester Epidemiology Project is available through our website http://www.rochesterproject.org. Like other large cohort studies nested within a records-linkage system, the use of the data is complex. We encourage investigators interested in using the four cohorts to test specific hypotheses to develop a collaboration with our research team. Queries should be sent via email to Dr Rocca (rocca@mayo.edu) with a one-page outline of the intended project.