Article Text

Abstract
Objectives The existing British National Patient Safety Agency (NPSA) safety guideline recommends testing the pH of nasogastric (NG) tube aspirates. Feeding is considered safe if a pH of 5.5 or lower has been observed; otherwise chest X-rays are recommended. Our previous research found that at 5.5, the pH test lacks sensitivity towards oesophageal placements, a major risk identified by feeding experts. The aim of this research is to use a decision analytic modelling approach to systematically assess the safety of the pH test under cut-offs 1–9.
Materials and methods We mapped out the care pathway according to the existing safety guideline where the pH test is used as a first-line test, followed by chest x-rays. Decision outcomes were scored on a 0–100 scale in terms of safety. Sensitivities and specificities of the pH test at each cut-off were extracted from our previous research. Aggregating outcome scores and probabilities resulted in weighted scores which enabled an analysis of the relative safety of the checking procedure under various pH cut-offs.
Results The pH test was the safest under cut-off 5 when there was ≥30% of NG tube misplacements. Under cut-off 5, respiratory feeding was excluded; oesophageal feeding was kept to a minimum to balance the need of chest X-rays for patients with a pH higher than 5. Routine chest X-rays were less safe than the pH test while to feed all without safety checks was the most risky.
Discussion The safety of the current checking procedure is sensitive to the choice of pH cut-offs, the impact of feeding delays, the accuracy of the pH in the oesophagus, as well as the extent of tube misplacements.
Conclusions The pH test with 5 as the cut-off was the safest overall. It is important to understand the local clinical environment so that appropriate choice of pH cut-offs can be made to maximise safety and to minimise the use of chest X-rays.
Trial registration number ISRCTN11170249; Pre-results.
- decision analysis
- ph monitoring
- nasogastric tube
- adult feeding
- diagnostics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitation of this study
A decision analytic approach was used to map out clinical pathways and to achieve synthesis of evidence from clinical studies, published literature and expert judgements.
The entire range of pH cut-offs was analysed in addition to the most frequently used ones between 4 and 6.
Two non-pH test strategies were analysed using the same framework: routine chest X-rays and feeding all patients without safety checks.
We did not consider financial costs in this analysis. The same framework can be expanded to incorporate additional dimensions of importance.
We focused only on the group of patients with successful aspirations. Unsuccessful aspiration does not change the relative safety of various pH cut-offs but is one reason for using chest X-rays. Our analysis assumed that chest X-rays were 100% accurate. However, reducing pH cut-offs will not increase misfeeding due to chest X-ray misinterpretations.
Introduction
Every year at least 1 million nasogastric (NG) tubes are being used in the UK1 and 1.5 billion worldwide.i Inadvertent tube placement outside the stomach has been classified as a ‘never event’ by NHS England.ii Nevertheless, incidents of tube misplacements remained common place. Reported rates of misplacement on insertion and tube migration after correct initial placement varied between 1.3% and 50% in adults.2 Misplacement into the respiratory tract occurs in 1%–3% of patients3 and can have catastrophic consequences, including death. Guidelines on nutrition support for adults issued by the National Institute for Health and Care Excellence recommend that the position of NG tubes be verified on initial placement and before each use.4 The British National Patient Safety Agency (NPSA) recommends testing the pH of tube aspirates.5–7 Feeding can only start if a pH at or below 5.5 has been established; otherwise chest X-rays, the gold-standard, should be used.
Commissioned by NPSA, we investigated evidence behind various bedside tests including pH, aspirate appearance, capnometry/colorimetric, auscultation (‘whoosh’ test) and magnetic guidance.8 The pH test has the best bedside usability and accuracy underpinned by a large body of clinical evidence. In addition to respiratory placements, oesophageal placements emerged as a major safety concern during our consultations with feeding experts.9 To address this and to remedy the lack of published studies in oesophageal pH from NG tubes, we carried out a literature review of pH distributions in patients with reflux. We found that reducing the cut-off from 5.5 to 4 would increase the sensitivity of the pH test to tubes placed in the oesophagus. Subsequent safety recommendations continued to uphold 5.5 as the safety threshold.10 The main disadvantage of lowering the pH cut-off is that more patients with tubes placed inside the stomach will be sent for chest X-rays, which is the second-line test. This is not ideal since chest X-rays are not only more expensive—on average each chest X-ray costs £30 whereas a tube of 100 pH strips costs slightly over £10iii—but also can delay feeding for up to 47 hours.iv In addition, chest X-rays, despite being considered the gold-standard of tube site verifications, are subject to misinterpretation errors.7 11
A drawback of our previous research was an exclusive focus on the risks from various bedside tests. However, the recommended checking procedure, in fact, uses a combination of two tests: the pH test followed by chest X-rays should the pH test fail. The question of selecting suitable pH cut-offs must be addressed using the same context. We are primarily interested in understanding the trade-offs in patient safety between maximising feeding in time and minimising feeding incidents. The aim of this research is to employ a decision analytic modelling approach12 which allows us to systematically analyse the safety of pH test under various cut-offs when embedded in the clinical setting13 to better inform policy makers and clinicians performing safety checks.
Materials and methods
Analysis of the National Reporting and Learning System
To provide an overview of the feeding incidents, we carried out a narrative analysis of incident reports submitted to the National Reporting and Learning System (NRLS). We included all cases with evidence of nasogastric tube misplacement at any site outside the stomach between October 2003 and 28 February 2009. Paediatric cases were excluded. Two authors (OHP and SO) independently reviewed the adverse event reports and classified these according to whether or not current safety guidelines were followed (cut-off 5.5). For reports containing sufficient details to enable an analysis of possible reasons of tube misplacements, we extracted the reported reasons for misfeeding and carried out thematic analyses to generate categories. Disagreements between the two reviewers were solved by discussion until consensus was reached.
Safety of pH under various cut-offs
Study design
We mapped out the clinical pathway of the safety guidelines with regard to NG tube feeding (figure 1). Since our target was the relative safety between different pH cut-offs, we focused on the subgroup of patients for whom aspirations were successful but analysed implications of unsuccessful aspirations on patient safety in the sensitivity analysis. We assumed that the pH cut-off values could take any number between 1 and 9 (the recommended range), as well as 5.5 (the current recommendation). Decision outcomes were scored with points out of 100, with 100 assigned to the outcomes with the best safety and 0 to the outcomes with the worst safety. The sensitivities and specificities of the pH test under various cut-offs were derived from our previous research. Aggregating the outcome scores by their respective probabilities resulted in a set of weighted scores. These weighted scores enabled a comparison of the relative safety of the pH test under various cut-offs.

Clinical pathway of using pH test to ensure safety in feeding by nasogastric tubes.
Outcomes of feeding decisions
Decision outcomes were identified from the clinical pathway (figure 1), assuming that all patients have successful aspirations. There were five outcomes in total. Feeding into the stomach by pH took place if the pH was at or below a certain cut-off and when the tube had been placed inside the stomach. Feeding into the lung or oesophagus took place when a low pH (≤cut-off) was combined with tube misplacements. If the pH exceeded a certain cut-off, then chest X-rays were used to establish tube sites. For those patients with tubes placed inside the stomach, the X-ray was deemed unnecessary because gastric placement could have been determined solely by pH. We distinguish between feeding by pH and feeding by chest X-rays since the latter carries radiation risks and could cause feeding delays for up to 47 hours.iii The remaining patients who received chest X-rays would reveal misplaced tubes—these were correctly identified and excluded, thus no feeding outside the stomach.
The safest outcomes (ie, feeding into the stomach by pH, no feeding outside the stomach) were assigned a score of 100 and the least safe outcomes (ie, feeding into the lung) was assigned a score of 0. For the remaining outcomes, we applied the analytic hierarchy process,14 converting qualitative judgements into quantitative scores. Two clinicians who were experts in gastroenterological diseases were invited to a face-to-face meeting with one of the authors (MN). During the meeting, they were briefed about the project and asked to first rank all the outcomes according to safety. They were then asked to make pairwise comparisons and articulate the strength of their preferences. For instance, feeding into the oesophagus was considered safer than feeding into the lung and the preference was very strong.
Consensus was reached through discussions, producing preference judgements ranging from no difference, weak, moderate, strong to extreme. We entered these into the MACBETH15 component of the decision analysis software, HiView. The software first checked whether the judgements were consistent with the safety rankings and once satisfied, converted the judgements into numeric ratings (table 1, last column). Further consistency checks were performed on the scores. For instance, oesophageal feeding received a safety score of 45, which means that its safety was considered nearly halfway in between the safest outcome (stomach feeding) and the least safe outcome (lung feeding). This should mirror the pairwise comparisons, where the preference for stomach feeding over oesophageal feeding (100 vs 45) was slightly stronger than the preference for oesophageal feeding over lung feeding (45 vs 0).
Probability and safety of decision outcomes of the pH test
Outcome probabilities were driven by two independent factors—the initial insertion (prior distribution of tube sites) and the accuracy of the pH test in differentiating various tube sites (ie, test sensitivity and specificity, table 1, middle column). Given the wide range of variations in reported tube misplacements and tube migrations (1.3%–50%), we assumed an average risk of insertion errors, whereby 70% of the tubes were inside the stomach with an equal number (15%) of misplacements in the lung and oesophagus (see online supplementary appendix 1 for reasoning). The sensitivities and specificities under individual pH cut-offs were extracted from our previous research. They were based on a clinical database with 1035 unique patient records from multiple clinical trials by a single clinician. This database included 754 stomach placements and 281 lung placements,16 17 with pH measured by both pH metre (Beckman pH1 10 portable pH metres) and pH paper throughout (1–11 Vivid pH paper). Since pH metre reading and paper reading do not always agree, we used pH metre reading to derive the accuracy data. Lack of evidence for oesophageal placements was remedied by reviewing studies on healthy cohorts under observations for reflux.18–20 Distribution of oesophageal pH was estimated based on the proportion of time when pH decreased below the various cut-offs. Table 2 summarises the accuracy of pH tests.
Supplementary file 1
Accuracy of pH test under cut-offs 1–9
Aggregating outcome scores by their respective probabilities resulted in a set of weighted scores. These reflected the relative safety of the recommended checking procedure under different pH cut-offs. In addition to the pH test, we analysed a scenario where patients are fed without safety checks (feed all) and where all patients are sent for chest X-rays before feeding (routine X-rays).
Sensitivity analyses
To capture the spectrum of insertion errors, we analysed two additional scenarios with low (10%) and high (50%) probability of tube misplacements (see online supplementary appendix 1 for reasoning). Lung and oesophageal intubations were equally likely at 5% and 25%, respectively. Tornado diagrams were used to identify variables of importance. All outcome and probabilistic inputs were varied ±15% within range (0–1 for probabilities and 0–100 for outcomes). Three-way sensitivity analyses were carried out to examine the direction of impact.
We considered the impact of successful aspirations, whereby aspirations were successful 90% of the time.21 For the remaining 10%, chest X-rays are used instead. We considered the impact of chest X-ray misinterpretations by assuming that chest X-ray of tubes located outside the stomach was interpreted as inside 10% of the time, which resulted in feeding into the wrong places (equally likely in lung and oesophagus)[v]. We then analysed the joint impact of unsuccessful aspirations combined with radiography misinterpretations.
We carried out the analyses in Microsoft Excel and TreeAge Pro (2015). Since chest X-rays were used as the reference standard across pH accuracy studies, chest X-rays were assumed to be 100% accurate in the main body of analysis.
Results
Analysis of feeding incidents reported to NRLS
A total number of 2368 adverse event reports were identified. After excluding cases that were irrelevant or with incomplete information, we reviewed 104 cases with documented feeding tube misplacement. These included 6 counts of death, 15 counts of severe harm and 23 counts of moderate harm. The remaining 60 cases recorded no harm (43 cases) or low harm (17 cases). Further analysis was carried out on 75 out of 104 narratives containing sufficient details. In 11 reports, the wrong tube location was discovered prior to feed or medication (either by pH or by chest X-rays). Of the remaining 64 cases, we analysed reasons for misfeeding. The most frequently cited reason was misinterpretation of chest X-rays (25 cases). The pH test (with 5.5 as the cut-off) itself was responsible for 10 feeding incidents. There were also 23 cases where safety guidelines were not followed, including 12 cases where feeding was carried out without safety checks (table 3, online supplementary appendix 2 for further details).
Supplementary file 2
Mode of failure to identify tube misplacement
Safety of the pH test under various cut-offs
The higher the cut-off, the more sensitive and the less specific the pH test becomes (table 2). However, it is impossible to be free from X-ray-related feeding delays and at the same time to be free from feeding incidents due to the lack of accuracy of the pH test. This is captured in figure 2, which shows the trade-off between feeding incidents (more numerous under higher cut-offs) and feeding delays (more numerous under lower cut-offs). As the cut-off reduced, the increase in the number of unnecessary X-rays (feeding delays, x axis) was faster than the reduction in feeding incidents (y axis). Consider cut-off 5 vs 6 for instance. The magnitude of difference was four times, that is 9% (=22%–13%) increase in unnecessary X-rays versus 2.1% (=2.9%–0.8%) decrease in feeding incidents (primarily in the oesophagus).
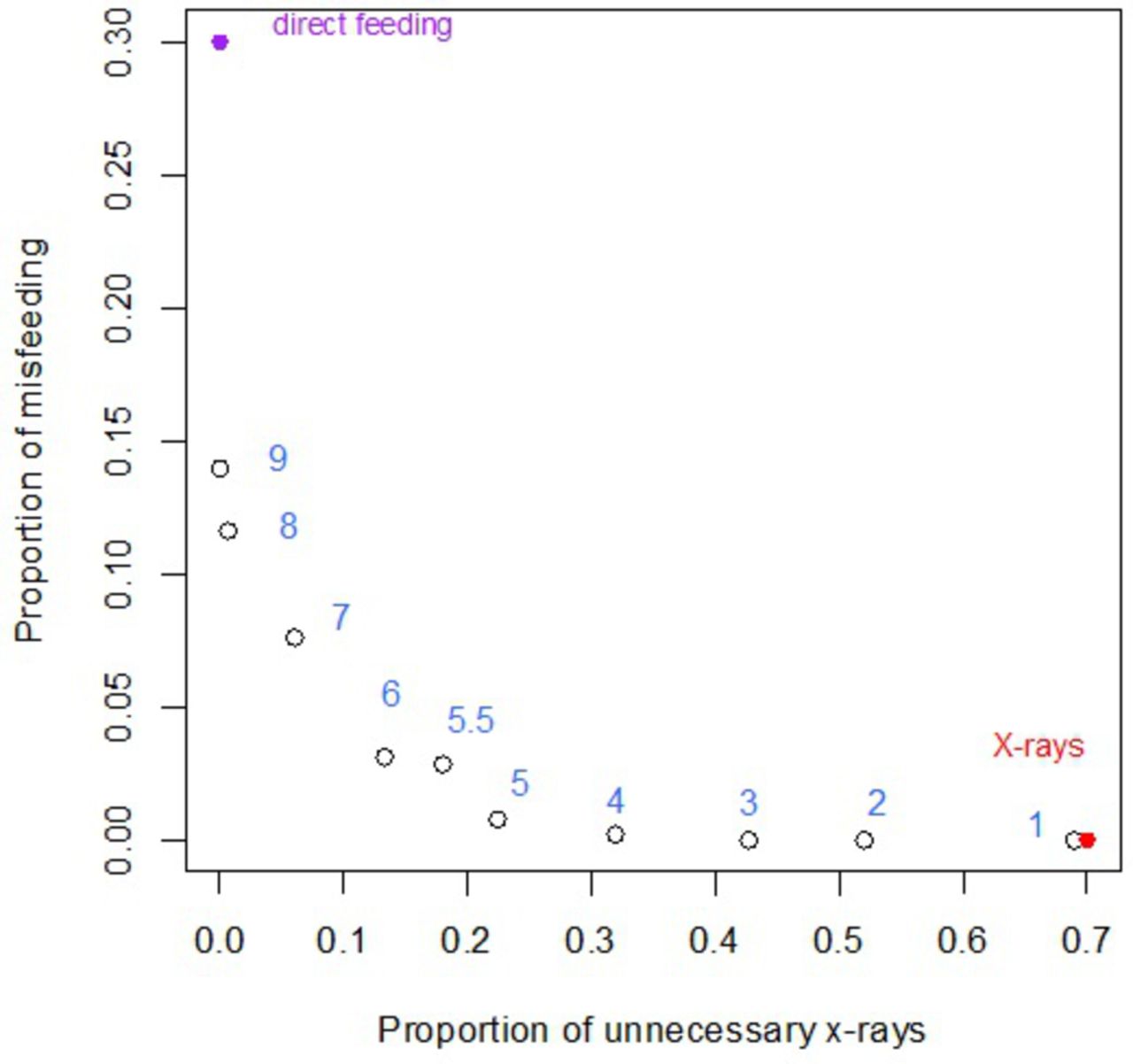
Trade-off between the number of unnecessary X-rays and feeding incidents.
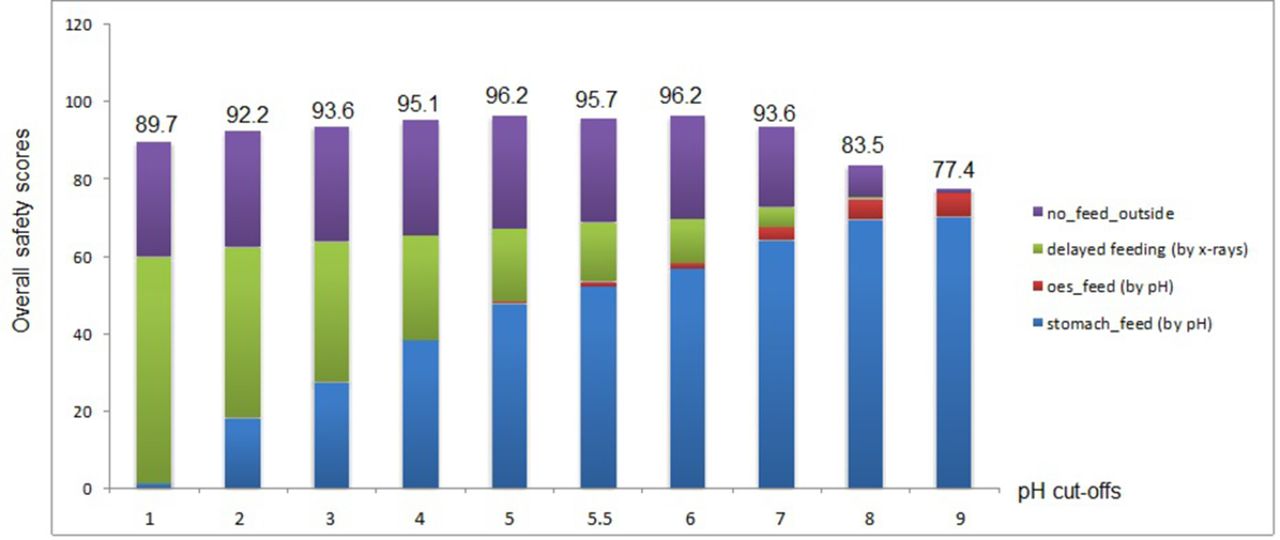
Nevertheless, it would be misleading to select pH cut-offs based on the number of feeding delays or feeding incidents alone because different outcomes have different impact on patient safety. Instead, we used the aggregated safety scores to assess the relative safety under different cut-offs. These are shown in figure 3, along with part-score contributions made from individual outcomes. At lower cut-offs, the scores were primarily made up of delayed feeding and no feeding outside the stomach, whereas at higher cut-offs stomach feeding made increasingly significant contribution to the overall safety. No points were attributed to lung feeding with a safety score of 0.

{kind=link}
{kind=link}
{kind=link}
Safety of the checking procedure under pH cut-offs 1–9, showing separate contributions made by each decision outcome to the overall weighted safety scores.
Cut-off 5 and cut-off 6 had the highest safety score (96.2), and, therefore, the ‘safest’ overall. This is in a context of an ideal (and hypothetical) test which has a score of 100, by identifying every tube in the stomach for feeding while excluding every tube outside the stomach. By contrast, to feed all patients without discrimination is the least safe strategy with a weighted score of 76.75, from feeding correctly (though randomly) in 70% of patients with stomach placements (part score 70) but misfeeding in 15% oesophageal placements (part score 6.75) and in 15% lung placements (part score 0). Routine use of chest X-rays had a weighed score of 89.5 from correctly identifying all 30% of misplaced tubes (part score 30) and from feeding correctly in 70% of the patients though with a delay (part score 59.5, mean delay 17 hours, range 1.5–47 hours,iii see online supplementary appendix 3 for further details).
Supplementary file 3
Sensitivity analysis
The largest impact on the overall safety was attributable to safety of delayed feeding (scores 50–95) and to the pH specificity in the oesophagus (range 0.6–0.99). Decreasing the score assigned to delayed feeding by five points (from 85 to 80) would make cut-off 5, the safest option. A 10% increase at 5.5 (from 0.81 to 0.89) while keeping the specificities at 5 constant (0.948) would result in cut-off 5.5 becoming the safest overall. Varying the initial tube misplacements also had a large impact, influencing safety across all cut-offs. However, cut-off 5 remained the ‘safest’ under 50% tube misplacements. Similarly, unsuccessful aspirations and/or chest X-ray misinterpretations reduced the safety across all cut-offs and more so for lower cut-offs than for higher cut-offs, since chest X-rays were used more often at lower cut-offs. Despite this, pH test under cut-off 5 remained the safest within range 1–5.5 (table 4).
Sensitivity analysis of the safety of various pH cut-offs
Discussion
Summary of main findings
The recommended safety procedure prior to feeding by NG tube is composed of two tests, the pH test and chest X-rays when the pH test fails (>5.5). Our analysis showed that with a score of 96.2 out of 100, the checking procedure was the safest under cut-off 5 given 30% or more of tube misplacements. Respiratory feeding is excluded; misfeeding in the oesophagus was kept to a minimum to balance the need to reduce feeding delays from unnecessary chest X-rays. Routine chest X-rays were less safe than the pH test (score 89.5) and to feed all was the most risky (score 76.76).
Strengths and limitations
Using a decision analytic approach, we analysed the safety of the checking procedure under pH cut-offs 1–9 based on combined evidence from expert judgements, literature and clinical studies. We considered both the impact and the probabilities of various outcomes. Feeding delays caused by chest X-rays were formally incorporated, by a safety score lower than the ideal 100. The entire range of pH cut-offs was analysed, in addition to the commonly used ones. The safety of routine chest X-rays and feeding all patients without checks was similarly analysed.
The key evidence base underlying this analysis comes from Metheny et al over a 12-year period (1989–2001). Although slightly dated, this research, we believe, remains the most impressive body of evidence on aspirate pH measurement and prediction of feeding tube position by using a standard well-designed study protocol from six acute care hospitals.
The largest uncertainty remains in the oesophageal pH, especially in the critical range between cut-offs 4 and 5.5 due to the lack of direct evidence. We did not consider costs in this analysis. However, the same framework can be applied when new evidence becomes available and extended to incorporate additional factors of importance, for example, costs. A further limitation of our study is that our evidence on gastric and respiratory pH came from pH metre measurement whereas in practice pH papers are widely used. This will not influence our conclusion because pH paper is known to be less sensitive when compared with pH metre. In addition, we have focused only on the subgroup of patients with successful aspirations since we are primarily interested in the relative safety of pH cut-offs. Our sensitivity analysis explored impact from unsuccessful aspirations and chest X-ray misinterpretations. Although safety across all pH cut-offs has been reduced, cut-off 5 remains the safest test to use.
Comparison with existing literature
As a universal first-line test for ensuring feeding safety, numerous studies investigated the pH test for its accuracy in identifying stomach and lung placements.16 17 However, all the studies focused on the accuracy of the pH test per se. By contrast, the checking procedure, in fact, contains two tests: the pH test followed by chest X-rays when necessary. Thus, the safety of the pH test must be evaluated in the context of its use, by considering its downstream implications for clinical decision-making. We found that the key issue was to achieve a balance between reducing feeding incidents and reducing unnecessary chest X-rays. The decision analytic approach provides the normative framework for dealing with conflicting objectives. One study closer to our remit22 investigated cost utility of the clinical algorithm (ie, checking procedures) for NG tube placement confirmation in adult patients. Our study differs from this study in that in our study accuracy of the pH test is not a given but constitutes the key source of uncertainties for achieving safe NG feeding.
Implications for practice
Although the current recommended pH cut-off is 5.5, the British Society of Gastroenterology guidance for enteral feeding suggests that tube aspirate pH measurement needs to be <5.0 prior to every use, but advises caution when the patient is on acid suppression.23 Routine use of X-rays was not advised. Our study showed that reducing the pH cut-off from 5.5 to 5 can reduce the number of feeding incidents. Because majority of the patients have stomach placements, and because gastric pH has a mean value around 4,8 a lower threshold means that more patients will be sent for chest X-rays. Chest X-rays, when misinterpreted, can lead to feeding incidents.7 There is a clear need to develop cost-effective bed-side tests which not only have high accuracy but also have the ability to withstand human errors in their applications.
Chest X-rays misinterpretations
Although chest X-ray misinterpretations constituted a major source of feeding errors (table 3), our main analysis assumed that chest X-rays were 100% accurate based on a number of considerations. First, we limited our evidence base to a cohort of clinical studies with clear demonstration of administering and interpreting a reference standard (see above). This gave us confidence in the accuracy of chest X-rays in our evidence base. Second, there is little data on the actual distributions of chest X-ray misinterpretations in relation to NG tube feedings, obscuring the direction in which the analysis would be influenced by such an assumption. A stomach tube might be misinterpreted as located outside the stomach, resulting in either overestimation of the specificity of the pH test (when pH>5.5) or underestimation of test sensitivity (when pH<5.5). Similarly, a non-stomach tube might be misinterpreted as located inside the stomach, with opposite implications for test sensitivity and specificity.
It is also important to note that in practice, reducing pH cut-offs from the existing 5.5 to 5 will not increase misfeeding attributable to chest X-ray misinterpretations. This is because the change will affect those patients with a pH between 5 and 5.5. All these patients will receive feeding under the existing cut-off, whereas under the new, lower cut-off, only a proportion of them, who have demonstrated stomach intubation from chest X-rays, will be fed. An important lesson here is that the quality of a formal analysis is inevitably constrained by the availability of the evidence, and the quality of it.
Conclusions
The pH test with an upper cut-off at 5 was the safest test for the verification of NG tube locations. The choice of pH cut-off depended on the prevalence of tube misplacements, the impact of feeding delays and the specificity of the pH test for oesophageal placements. Routine data collection at the local level should be implemented to optimise safety recommendations.
References
Footnotes
↵i Worldwide usage of 1.5 billion was estimated from NHS usage by assuming demand proportional to population size.
↵ii https://www.england.nhs.uk/wp-content/uploads/2015/03/never-evnts-list-15-16.pdf
↵iii Costs of chest X-rays were derived from NHS reference price 2015 and price of pH strips were from NHS supply chain website (https://www.supplychain.nhs.uk/).
↵iv Mean delay 17 hours, range 1.5 hours–47 hours. Unpublished audit data carried out in 2016 at the St Mary’s hospital, London, UK from 23 patients.
↵v There is no reported data on the frequency of chest X-ray misinterpretations for verifying NG tube insertions. Reported error rates of diagnostic X-rays for lung cancers ranged between 5.3% and 24%. Since chest X-ray is a second-line test, the greater the likelihood of its misinterpretations, the more a higher rather than lower pH cut-off would be preferred.
Contributors GBH, PMMB, LDP and MZN designed the study; MZN, OHP and SO conducted research; OHP and SO analysed the NRLS database. MN, OHP and SO interpreted the data. MZN carried out the decision analysis. MZN, JRH and PMMB drafted the manuscript. Final manuscript is approved by all authors. GBH had final responsibility for the final content.
Funding The research was supported by the NIHR Diagnostic Evidence Co-operative, London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. MZN is also partially supported by a grant from the Innovate UK (Biomedical Catalyst Fund, ref: 102134) award to GBH and company Ingenza, for developing a new pH paper test for nasogastric tube placements.
Competing interests None declared.
Ethics approval London—Chelsea REC(Reference: 16/LO/0998), which supported a clinical study as well as interview studies related to the use of pH tests in the clinical setting.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data availale