Article Text

Abstract
Objective The present study aimed to evaluate the association between smoking and incident pterygium in adult Korean men.
Design A retrospective nationwide longitudinal cohort.
Setting National Health Insurance database of South Korea.
Participants This study included Korean men (age range: 40–79 years) registered in the Korea National Health Insurance Service database from 2002 through 2013. We compared HRs for pterygium between 90 547 current/past and 90 547 never-smokers via 1:1 propensity-matched analysis.
Primary outcome measure Incident cases of pterygium were identified from the database.
Results Pterygium developed in 5389 (6.0%) never-smokers and 3898 (4.3%) past/current smokers (P<0.001). The incidence of pterygium per 1000 person-years in never-smokers and in past/current smokers was 6.5 and 4.7, respectively (age-adjusted HR, 0.73; 95% CI, 0.70 to 0.76). This protective effect was more pronounced among current smokers than among past smokers (for current smokers: HR, 0.68; 95% CI, 0.65 to 0.71 and for past smokers: HR, 0.85; 95% CI, 0.80 to 0.90). A longer duration of smoking and higher amounts of cigarette consumption were associated with a lower incidence of pterygium.
Conclusions Longitudinally, cigarette smoking was associated with a reduced risk of pterygium, and this protective effect was more pronounced among current smokers than among past smokers.
- cigarettes
- incidence
- pterygium
- smoking
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study is unique because our study is the first large-scale longitudinal study to evaluate the temporal relationship between cigarette smoking and risks of pterygium.
A lack of clinical information, including visual acuity, severity of pterygium and the eye affected, is an inherent limitation of the present claims database study.
Last, we could not access data on sun exposure, which is one of the most important risk factors for pterygium. However, our detailed stratified matching allowed us to establish two comparable groups and eliminated the effect of confounding factors, such as sun exposure.
Introduction
Cigarette smoking is considered one of the most important risk factors for a number of systemic diseases1 and eye diseases such as age-related macular degeneration,2 retinal vein occlusion3 and thyroid eye disease.4 However, for some diseases or conditions, inverse association was also reported: smoking seemed to relieve inflammatory bowel disease5; smoking was associated with decreased incidence of Parkinson disease6 and smokers seemed to have better short-term health outcomes than non-smokers following hospitalisation for heart attacks, a phenomenon also known as ‘smoker’s paradox’ in cardiology.7 8
Pterygium is a triangular mass of thickened conjunctiva extending over the cornea that may cause a disturbance in vision. The association between smoking and pterygium has been investigated via cross-sectional studies,9–21 a propensity score-matched study22 and meta-analysis.23 Unlike most reports on the negative aspects of smoking in public health and the majority of systemic diseases, smoking has been repeatedly reported as a protective factor against the development of pterygium in cross-sectional studies,13–16 including one conducted in Korea.21
However, to establish a temporal relationship between cigarette smoking and the development of pterygium, a large, well-designed longitudinal cohort study is required. The National Health Insurance Service (NHIS) database in South Korea provides an adequate opportunity for the evaluation of the development of pterygium among the general population according to smoking status. Therefore, we evaluated the association between cigarette smoking and incident pterygium in a nationwide random sample comprising 181 094 men from South Korea.
Methods
Ethics
This retrospective cohort study adhered to the tenets of the Declaration of Helsinki, and the study design was approved by the institutional review board of the NHIS Ilsan Hospital, which waived the requirement for written informed consent.
Database
A unique national insurance system has been implemented in South Korea, covering approximately 97% of the nation’s population. This study used a new dataset developed by the Korean NHIS and released for use in research for the first time in 2016: the National Health Screening Cohort (NHIS-HEALS).24 The NHID includes approximately 510 000 randomly selected individuals between the ages of 40–79 years, who were enrolled in the Korean National Health Screening Program in 2002 and 2003 (~10% of NHIS beneficiaries who had participated in a screening program). These selected participants were followed up until 2013. The database contains data regarding sociodemographic factors, medical examination results, interventions, prescription drugs and diagnostic codes for all medical care transactions from all types of medical facilities. Detailed cohort profiling has been described previously.24
Study cohort
Based on a previous report regarding the presence of a large proportion of unreported women smokers in Korea due to cultural and social barriers,25 and because of the very low proportion of women smokers (3.9%) in the NHID database, we included only men in this study. Therefore, the study cohort included men enrolled in the National Health Screening Program between 2002 and 2003 who met the following eligibility criteria: (1) response to questions regarding smoking status; (2) age between 40 and 79 years in 2002 (the lower and upper limits were set based on those of the database) and (3) clinical data for continuous variables including body mass index, blood pressure and other parameters (except age) within the top and bottom 1%. Patients with pterygium in 2002 and 2003 were excluded. A detailed diagram of the study population is shown in figure 1. We performed propensity matching of the study cohort according to propensity scores based on 38 potential baseline confounders, including age, income level, area of residence, medical history and examination results, history of prescription-drug use and antihypertensive medication and utilisation of eye care (table 1). Details regarding diagnosis codes for comorbidity are provided in online supplementary table 1. Sociodemographic factors such as income level or residence area were identified as one of the strongest predictors for pterygium in previous studies.9–21 All Korean citizens were categorised as insured employees, insured self-employed individuals or medical aid beneficiaries. This database provided subjects’ income levels in 10 percentiles for insured employees, 10 percentiles for insured self-employed and the lowest level of income for medical aid beneficiaries, in a total of 21 levels. However, since the proportion of medical aid beneficiaries were very small, we combined the lowest level of 10 percentiles from insured self-employed group and medical aid beneficiaries group. Geographically, South Korea could be divided into 16 different provinces. Therefore, we stratified income level using a 20-level categorisation and area of residence using 16-level categorisation. Korean citizens who were covered under NHIS were categorised as insured employees, insured self-employed individuals and Medical Aid beneficiaries. Income among insured employees was categorised into income levels 1–10, while income among insured self-employed individuals was categorised into income levels 11–20. Income among Medical Aid beneficiaries was categorised as income level 1.
Supplementary file 1

Flow chart of participant selection.
Baseline characteristics of the study participants (smokers vs never-smokers matched using propensity score matching)
Smoking status and validation
The Korean National Health Screening Program employed a standardised questionnaire for smoking status (see online supplementary document 1). Participants were classified according to smoking status as never-smokers or smokers. Smokers were classified as either past or current smokers. For subgroup analyses, we also collected data regarding the duration of smoking (≤9, 10–29 or ≥30 years) and daily cigarette consumption (<10, 10–19, 20–29 or ≥30 cigarettes).
To verify the smoking status of self-reported never-smokers during 2008–2013, we determined the proportion of men who had reported being current or past smokers during 2002–2007. A total of 61 210 men had reported being never-smokers more than once during 2008–2013, of whom 47 178 (77.1%) had reported being never-smokers more than once during 2002–2007 as well. Therefore, smoking status was largely consistent over time.26
Follow-up and primary end points
Participants enrolled between 2002 and 2003 were followed up from 1 January 2004 until the first date on which one of the following had occurred: loss to follow-up due to disqualification from NHIS (mainly death), incidence of pterygium in any eye or last visit to any medical care facility within the study period (31 December 2013). The primary end-point of the study was the incidence of pterygium. Cases of pterygium were defined based on an ophthalmologist’s examination and claims with the Korean Classification of Diseases code for pterygium (H110; corresponding to 372.4 from the International Classification of Diseases, Ninth Revision, Clinical Modification). Incident pterygium was defined based on the person rather than based on the eye.27 We defined an incident case as the first diagnosis of pterygium in any eye regardless of the right or left side of the eye.
Statistical analysis
We developed propensity models using logistic regression for smokers (past and current) compared with never-smokers. Individual propensities for smokers were estimated via logistic regression analysis of 38 potential confounders (table 1). Smokers and never-smokers were then matched according to propensity scores in a 1:1 ratio based on 8→1 digit matching. We performed descriptive statistical analysis of propensity-matched cohorts to estimate the incidence of pterygium per 1000 person-years. Cox regression models were used to estimate HRs. Data of the propensity-matched cohort were evaluated via age-adjusted analysis. The cumulative incidence of pterygium from 1 January 1 2004 to 31 December 2013 was described using a Kaplan–Meier survival curve. Cox proportional hazards analysis of the duration of smoking was performed according to 1-year age strata in order to account for immortal-time bias. The association between daily cigarette consumption and pterygium was evaluated via age-adjusted analysis. Proportional-hazard assumption for Cox regression was verified using the plot of log (-log); graphs showed no indication of violation. For sensitivity analysis, data of the whole cohort were evaluated via propensity-adjusted analysis according to deciles of propensity scores and age. The level of statistical significance was set at P<0.05. Analyses were performed using SAS System for Windows V.9.4 (SAS Institute, Cary, North Carolina, USA) and Stata/MP V.14.0 (StataCorp, College Station, Texas, USA).
Results
Characteristics of the study cohort
A total of 181 094 men met the inclusion criteria, including 90 547 never-smokers and 90 547 past/current smokers (table 1). Patient demographic and clinical characteristics in the whole unmatched cohort (n=229 493) varied greatly between the two groups; these data are provided in online supplementary table 2. In the propensity-matched cohort, all variables, except the incidence of pterygium, were similar between the two cohorts: pterygium developed in 5389 never-smokers and 3898 smokers (P<0.001). Detailed comparisons between the two groups based on the 20 income strata and 16 area of residence strata are provided in online supplementary table 3. Income and area of residence were similar between the two groups.
Incidence of pterygium
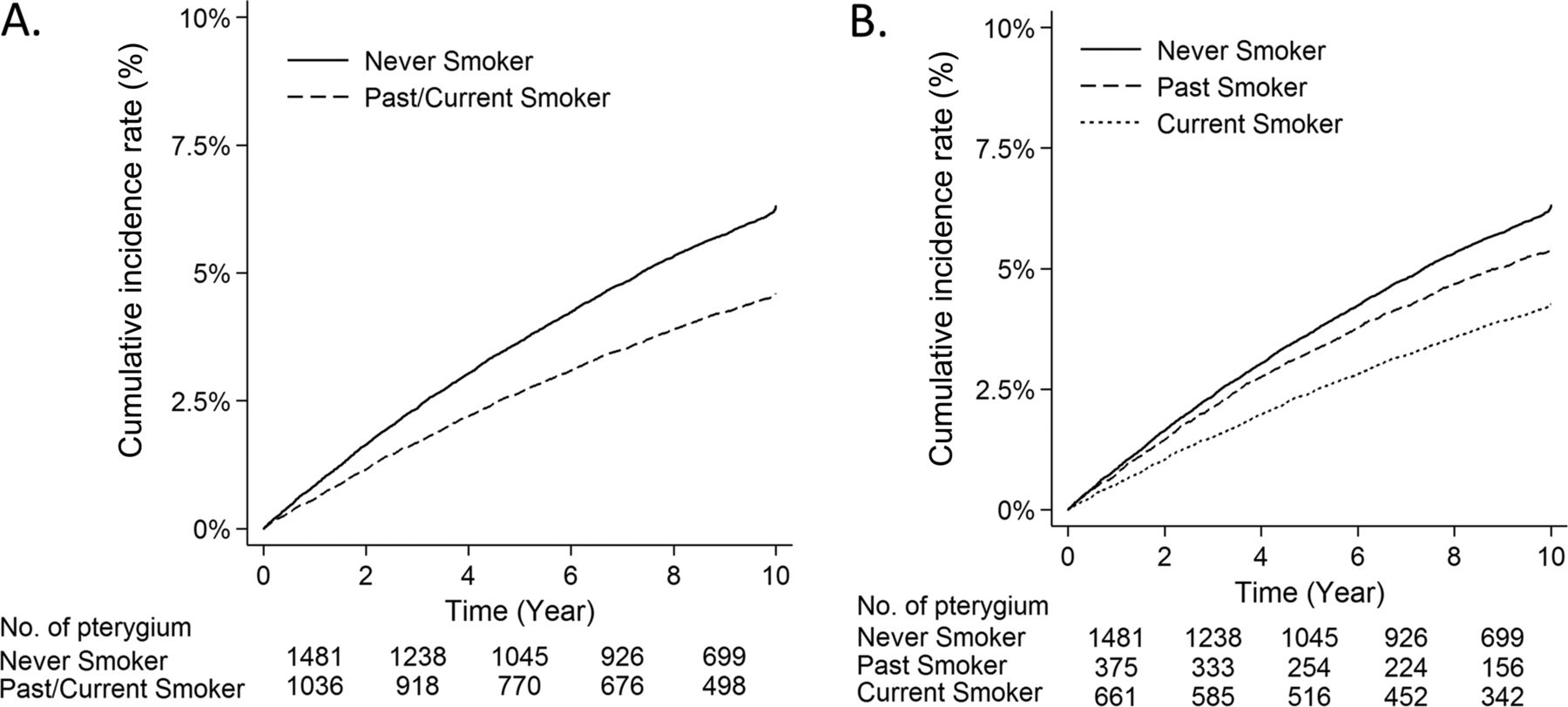
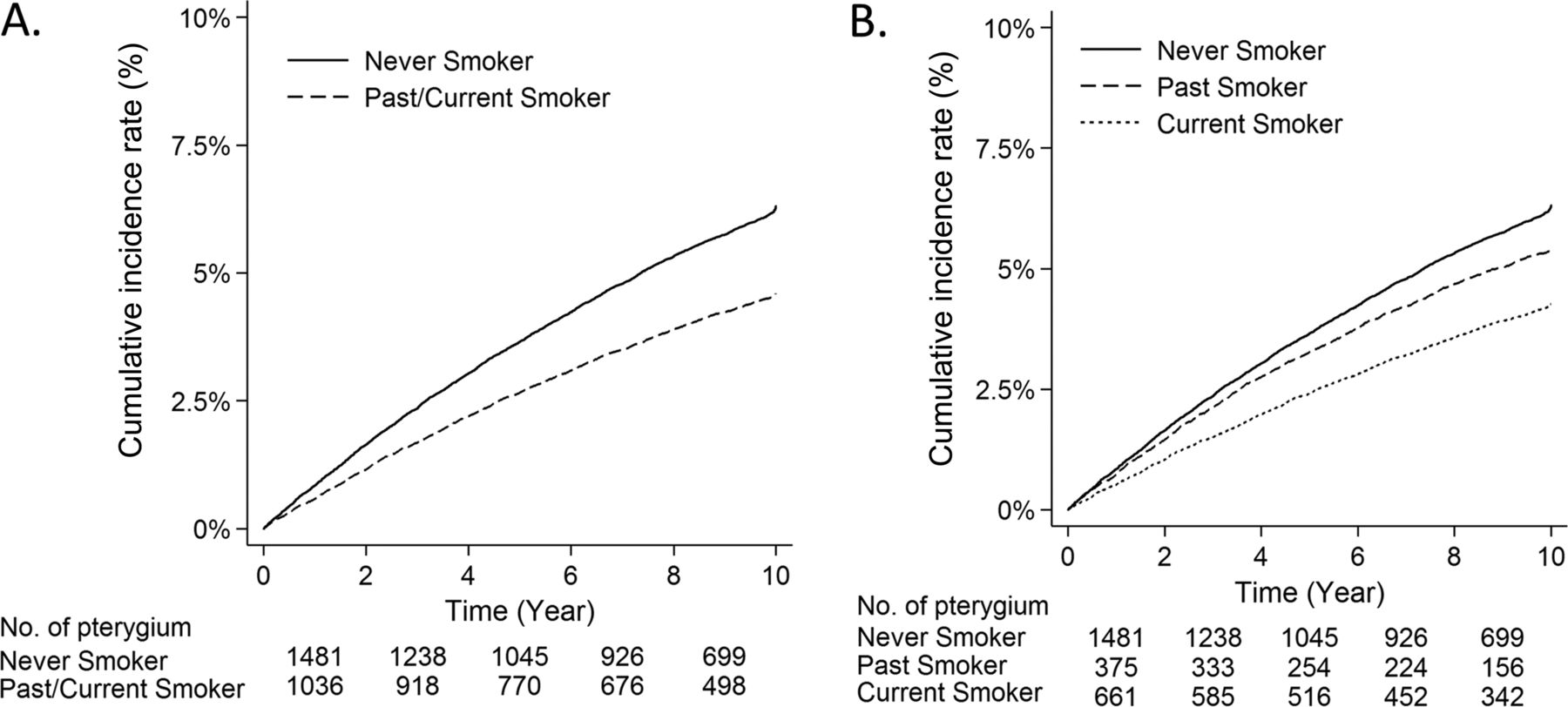
Table 2 presents the HRs for pterygium for the propensity score-matched cohorts. The risk of pterygium among smokers was significantly lower than among never-smokers in propensity-matched cohorts (age-adjusted HR, 0.73; 95% CI, 0.70 to 0.76). The risk of pterygium in age subgroups (40–59 and 60–79 years) exhibited a similar trend; however, HRs for the older age-subgroup were greater than those for the younger age-subgroup (HR: younger cohort, 0.70; older cohort, 0.79). The Kaplan–Meier survival curve demonstrated a clear difference in the incidence of pterygium between smokers and never-smokers (figure 2A).
{kind=link}
{kind=link}
Cumulative incidence of pterygium among smokers and never-smokers between 1 January 2004 and 31 December 2013. We observed significant differences in the cumulative incidence of pterygium between smokers and never-smokers included in a retrospective cohort derived from a National General Health Screening Program conducted between 2002 and 2013 (A and B).
Incidence of pterygium in smokers and non-smokers
In table 3, HRs for past smokers were lower than those for never-smokers and greater than those for current smokers in the age-adjusted model (HR: past smokers, 0.85; current smokers, 0.68). This trend was also reflected in the survival curve for the cumulative incidence of pterygium: the survival curve of past smokers was located between those of never-smokers and current smokers (figure 2B).
Incidence of pterygium in smokers and non-smokers
Table 4 shows subgroup analyses of smoking for the risk of pterygium. In the 1-year age-stratified Cox model, men who smoked for 10–19, 20–29 and ≥30 years were less likely to have pterygium than never-smokers (HR, 0.69, 0.70 and 0.75, respectively). Similar negative association was observed in terms of daily cigarette consumption: men who smoked <10, 10–19 and ≥20 cigarettes daily were less likely to have pterygium than never-smokers (HR, 0.69, 0.67 and 0.68, respectively). In sensitivity analyses of the unmatched cohort using propensity score-adjusted analysis, the multivariable-adjusted HR for pterygium for smokers was 0.72 (95% CI, 69 to 0.75) (see online supplementary table 4).
HRs and 95% CIs for pterygium according to duration and frequency of smoking
Discussion
To our knowledge, our study is the first large-scale longitudinal study to evaluate the temporal relationship between cigarette smoking and risks of pterygium in a nationwide sample of 181 094 Korean men. We confirmed the protective effect of smoking against the prospective development of pterygium in a historical cohort. This effect was more pronounced in current smokers than in past smokers and was surprisingly greater in men who smoked more than in those who smoked less. Our results are noteworthy because various conditions were controlled, including age, income level, area of residence, health examination variables, comorbidities, drug use and frequency of eye care utilisation.
Previous cross-sectional studies have reported inconsistent results regarding the prevalence of pterygium in individuals who smoke. Among the Chinese population in Singapore, smoking was associated with a higher risk of pterygium in univariate analysis; however, in a model with age, sex, occupation and smoking as covariates, no such association was observed.17 Among the Malay population in Singapore, bilateral pterygium was marginally associated with smoking (OR, 1.5; 95% CI, 1.0 to 2.2). However, no type of pterygium (in one eye or both eyes) was significantly associated with smoking (OR, 1.2; 95% CI, 0.9 to 1.5).11 Similarly, a more recent pooled analysis of the three major ethnic groups in Singapore revealed no significant association between smoking and pterygium/severe pterygium.20 In a previous cross-sectional study conducted in South Korea,21 analyses revealed somewhat different results depending on the method used to control for other variables, such as sociodemographic factors: in unadjusted analyses, longer duration of smoking was associated with an increased risk of pterygium; however, in adjusted analyses including sociodemographic factors and sun exposure as factors, the opposite finding was observed. Finally, in a multivariable model, lifetime smokers had a lower prevalence of pterygium compared with never-smokers (OR, 0.7; 95% CI, 0.6 to 0.9). This also highlights the importance of proper control for other sociodemographic factors in a cross-sectional study.21
The Barbados Eye Study, which included a predominantly African Caribbean population living in an area with very different climate and race compared with the above-mentioned Asian countries, also reported the protective effect of smoking on pterygium. However, an early cross-sectional study performed in 2001 reported a low prevalence of pterygium among current smokers (OR, 0.62; 95% CI, 0.41 to 0.94),13 while a later longitudinal study reported a relatively weaker protective effect (OR, 0.82; 95% CI, 0.48 to 1.39).28
The mechanism underlying the protective effect of smoking on pterygium remains somewhat unclear. Such effects may be explained by vasoconstriction or suppression of inflammatory cytokines induced by nicotine as well as alterations in the tear film such as increases in levels of secreted antibodies. However, as our epidemiological study could not provide any evidence regarding this matter, further studies are required to more fully elucidate the mechanism underlying the development of pterygium.
This study has several limitations. First, we had no access to data on the severity of pterygium or the eye affected (right, left or both). Second, it is possible that self-reported smoking habits are underestimated. However, this misclassification bias would lead to the underestimation of the true association between smoking and pterygium. However, it is possible that delayed diagnosis resulted in underestimation of pterygium incidence in the present study. Third, we also considered the possibility that the study population included in the health screening databases may have been biased relative to general population-based controls, who may not have received national general health screening. it is also possible that these biases were similar among smokers and never-smokers. To minimise selection or surveillance bias, we controlled for 38 possible confounding factors, including eye care utilisation. To minimise the immortal time bias, we performed a 1-year age-stratified analysis to estimate the association between duration of smoking and pterygium. Fourth, we could not access data on sun exposure, which is one of the most important risk factors for pterygium. However, we performed a detailed stratified matching of sociodemographic factors, including 20 strata for income level and 16 strata for area of residence, between smokers and never-smokers. This stratified matching allowed us to establish two comparable groups while eliminating the effect of confounding factors such as sun exposure. In addition, our results should be generalised with some caution, as this study was limited to East Asian men only.
In conclusion, our longitudinal study revealed a temporal relationship between cigarette smoking and subsequent lower incidence of pterygium. This protective effect was more pronounced among current smokers than among past smokers. We also found a low risk of pterygium in smokers, after dividing smoking by duration or intensity. Unlike the negative aspects of smoking in public health and various diseases, cigarette smoking may have an unexpected protective effect on the development of pterygium.
Acknowledgments
This study used data from the NHIS-NCS 2002-2013 (NHIS-2017-2-293), which was released by the KNHIS.
References
Footnotes
Contributors Conception and design: THR, DWK, CYC and SSK. Analysis and interpretation: THR, DWK, CYC and SSK. Data collection: THR, DWK, CYC and SSK. Manuscript preparation: THR, CYC and SSK. Overall responsibility: SSK.
Disclaimer The authors alone are responsible for the content and writing of this article. SSK had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval The institutional review board of the NHIS Ilsan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Access to NHIS-NSC data are available from the website of NHIS (https://nhiss.nhis.or.kr) after completing the application process and receiving approval (http://nhiss.nhis.or.kr/bd/ab/bdaba021eng.do). Detailed cohort profile and the methods for obtaining data are explained in the following source: Lee J, Lee JS, Park SH, Shin SA, Kim K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. International journal of epidemiology. 2016. doi: 10.1093/ije/dyv319. PubMed PMID: 26822938.