Article Text

Abstract
Objective The proliferation of studies using motivational signs to promote stair use continues unabated, with their oft-cited potential for increasing population-level physical activity participation. This study examined all stair use promotional signage studies since 1980, calculating pre-estimates and post-estimates of stair use. The aim of this project was to conduct a sequential meta-analysis to pool intervention effects, in order to determine when the evidence base was sufficient for population-wide dissemination.
Design Using comparable data from 50 stair-promoting studies (57 unique estimates) we pooled data to assess the effect sizes of such interventions.
Results At baseline, median stair usage across interventions was 8.1%, with an absolute median increase of 2.2% in stair use following signage-based interventions. The overall pooled OR indicated that participants were 52% more likely to use stairs after exposure to promotional signs (adjusted OR 1.52, 95% CI 1.37 to 1.70). Incremental (sequential) meta-analyses using z-score methods identified that sufficient evidence for stair use interventions has existed since 2006, with recent studies providing no further evidence on the effect sizes of such interventions.
Conclusions This analysis has important policy and practice implications. Researchers continue to publish stair use interventions without connection to policymakers' needs, and few stair use interventions are implemented at a population level. Researchers should move away from repeating short-term, small-scale, stair sign interventions, to investigating their scalability, adoption and fidelity. Only such research translation efforts will provide sufficient evidence of external validity to inform their scaling up to influence population physical activity.
- meta-analysis
- stairs
- point-of-choice
- intervention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The methods enabled pooling of estimates despite study heterogeneity.
We confined our analyses to studies with signs only, to allow for comparability among interventions.
We modelled the data using a ‘hypothetical effect to detect’.
We did not specifically audit generalisability measures in the included studies.
Introduction
Effective strategies to increase population levels of physical activity are much needed, given the high burden of non-communicable disease attributable to inactivity.1 Recent changes in the concepts of physical activity now suggest that total physical activity is important, and that methods to increase active living, through incorporating physical activity into everyday life, are important for achieving population-level change.2
One approach to encourage active living is the use of ‘point of choice’ signs to promote stair use. These interventions involve the short-term installation of a poster or stair-rise banners, to encourage people to take the stairs rather than an adjacent escalator. The promise of stair signage interventions to increase incidental physical activity is substantial.3 Furthermore, some studies have explored the physiological effects of regular stair use, and demonstrated cardiometabolic and biomarker improvements in those achieving high levels of stair use.4–6
Stair use signage is an environmental intervention that is potentially scalable, and could be delivered in multiple sites across communities. In addition, these interventions are inexpensive, simple to deliver, feasible and trial-able—all key elements of any new innovation that is introduced into a population.7
Much research has been conducted into the effects of ‘point of choice’ signs to promote stair use since 1980.8 Further studies in the 1990s were well publicised and addressed stair-promoting signs in underground train stations and shopping centres.9 ,10 Since then, a plethora of studies has investigated stair-promoting signs and stair-rise banners in numerous countries, but has focused more on selected settings, such as hospitals and health facilities, universities and government buildings.11–13 Other researchers have focused on the differences in efficacy through minor variations in intervention modality, for example, testing sign position and communication attributes of the message.14 Effects have been small but significant since the earliest studies, even in motivated samples such as School of Public Health staff15 or American College of Sports Medicine conference delegates.16
In the Centres for Disease Control and Prevention (CDC) Community Guide, published in 2002, stair promotional signage was a ‘strongly recommended intervention’ for public health approaches to promoting physical activity.17 The first review of these types of interventions, which included eight studies, suggested that a net increase of 2.8% in stair use could be expected following stair promotion signage.18 Webb et al19 pooled data from six of their own stair use studies in shopping centres, and reported a two-fold increase in the likelihood of stair use following a motivational sign; baseline stair use was 5.5%, with an additional 6% increase in stair use following these interventions. Another review of interventions up to 2006, which included 11 studies, demonstrated a median 2.4% increase from a median baseline of 8% stair users.20 This review further demonstrated that effects were similar across different baseline stair use levels, and with different stair use prompts and message reinforcers.
Nocon et al3 identified 25 studies, with 42 results, and in a narrative review reported that 31 of 42 effects were significant, with absolute stair use increases ranging from 0.3% to 10.6%. The ORs for post-signage, compared with presignage stair use ranged from 1.05 to 2.93, but due to heterogeneity, formal meta-analysis was not carried out. Finally, Bellicha et al21 reported an updated systematic review, with 50 studies included. Two-thirds of stair interventions in workplaces showed significant effects, as did three-quarters of studies in other settings. Absolute increases following stair promotion signs showed a 4% increase of the median baseline use. These reviews observed similar effect sizes, and used similar methods for review and effect size calculation.
The present study has three aims which build on previous reviews, but take a specific policy-relevance approach to these interventions. Our objectives were:
To carry out a meta-analysis which adjusts for study heterogeneity, to assess the pooled effect size of stair promotion interventions;
To identify, using a sequential meta-analysis approach, when in the history of these interventions was it clear that they were effective; and
To reframe the future research agenda in light of policy and practice needs.
Methods
This study followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).22 A literature search was undertaken using two electronic databases, Scopus and MEDLINE. For each database the following search terms were used, with no restriction on the year of publication:
Scopus: (TITLE-ABS-KEY (stair* OR (‘point of decision’)) OR (‘point of decision’ AND sign*) OR (‘point of choice’ AND sign*) AND (‘physical activity’ OR exercise OR fitness)).
MEDLINE: stair* and (point of decision OR point of choice) and (physical activity or exercise).
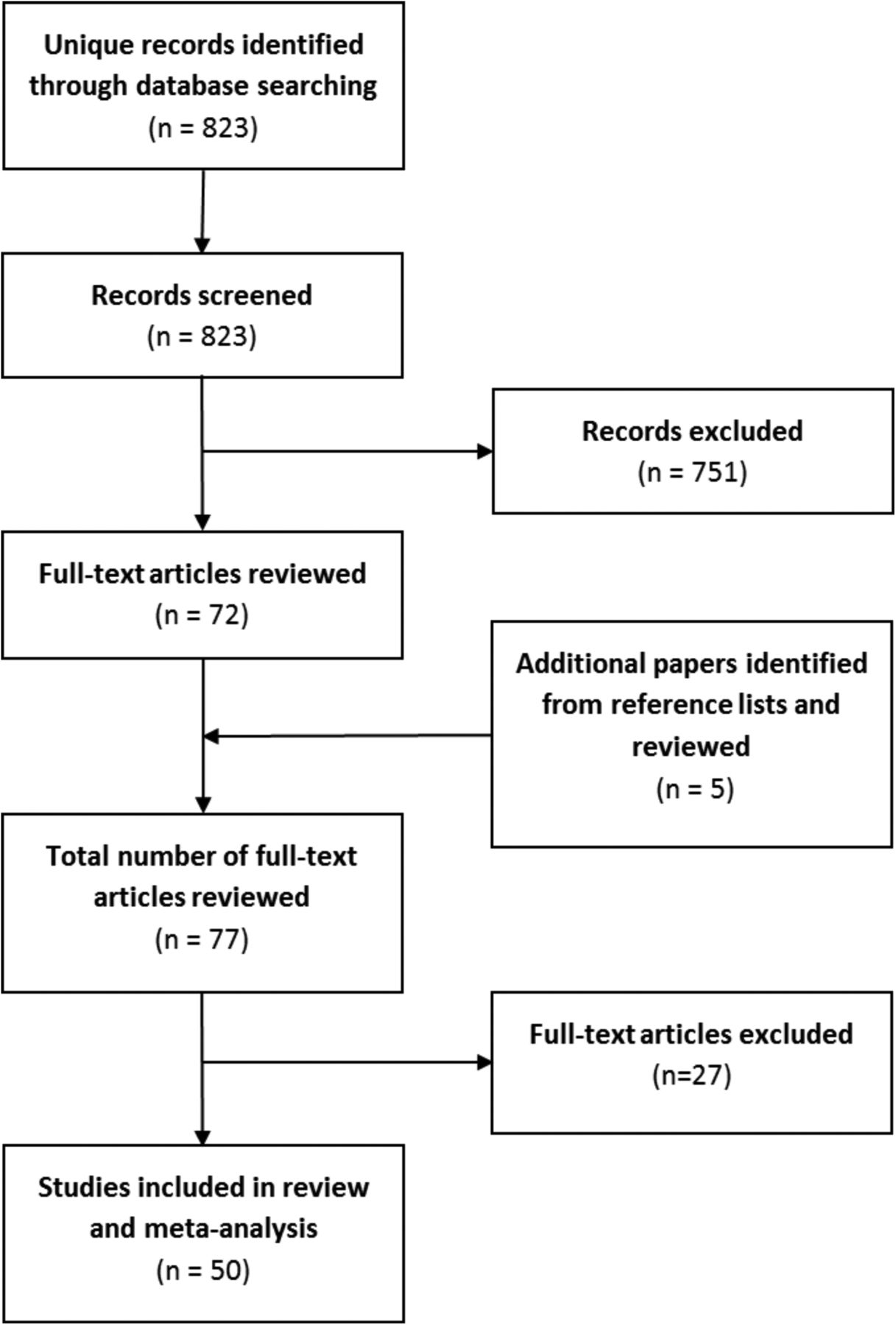
This search identified 823 studies. All titles and abstracts were screened to identify studies involving a stair use intervention. In total, 72 studies were located. The reference list of each of these papers were also screened, which identified a further 5 stair intervention studies, giving a total number of 77 papers for potential inclusion in the review. Full papers were obtained for these 77 studies and assessed for eligibility by at least two members of the research team.
Studies were eligible for inclusion if they used point of decision signs (including posters and stair rise banners) to encourage stair use, and reported the number of observations, and either the OR with 95% CIs or the number and percentage of people observed to use the stairs at baseline and post-intervention. The reported denominator in these studies was total observations of both stair and escalator/elevator use, and the primary outcome was the proportion of stair usage pre-post intervention.
The included studies typically used direct observation using multiple researchers to count occurrences of stair use versus escalator/elevator use, with one count recorded each time an individual took the stairs or escalator from one floor to another. Several studies used coding of videotape footage,23 infrared motion sensing24 or infrared sensing validated by direct observation.13 ,25 ,26 Studies were excluded if they were: a review paper, used self-report data only, reported physiological effects of stair climbing (as opposed to a behaviour change intervention) and/or used a multicomponent (more than just signage) intervention. These criteria led to the exclusion of 27 papers; the remaining 50 papers were included in the analysis (figure 1). The included studies were published between 1980 and 2014, reflecting a 34-year period.

Flow chart of study selection process.
The first objective was to assess the pooled impact of stair use signs, as this is the most generalisable format of this kind of intervention. The current review focused on stair climbing. If studies reported ascending and descending stair use separately, the ascending value only was used. For studies which did not differentiate ascending and descending stair use, the overall stair use data were used. This was the case for 14 out of the 50 included studies.9 ,10 ,12 ,13 ,15 ,16 ,24 ,27–33
For studies that reported pre-stair and post-stair use percentages, with an overall number of total observations, but did not report pre-observation and post-observation numbers separately, we assumed that total volume of pedestrian traffic remained relatively constant over time. Thus, equal numbers of observations were assumed during baseline and intervention periods when these periods lasted for the same duration. If the intervention data collection phase differed in duration to the baseline period, the number of observations was allocated proportionally.
Data were extracted on intervention sites only. Most studies were uncontrolled time series observations, but where control site data were available, these were not used in this analysis. For each study, data were extracted on stair use from baseline to the first post-sign measurement. If longer term follow-up was reported or posters were removed and replaced with a different poster, these effects were not included in this review. This allowed us to calculate one comparable estimate per study and therefore ensure even weighting of studies in the analysis.
If studies reported multiple effects for different population subgroups, for example, ethnic subgroups, males versus females or those of different age categories, these data were combined in the analysis into one study estimate. Also, if studies reported the impact of signs in a range of similar locations, for example, different shopping malls or different rail stations, data were pooled for analysis. However, if studies incorporated a range of different ‘types’ of sites, for example, stair signage at a bank, an airport, a library and an office (eg, ref. 12), these were considered as separate intervention estimates. For most studies, one estimate only was used; however, for some studies, two (8,14), three34 or four12 estimates were calculated. A total of 57 estimates were used from 50 studies included in the review (see online supplementary table A1).
supplementary appendix
Analysis
Analysis was carried out in two ways. First, effects of the interventions were expressed as ORs, derived from the pre-signage and post-signage proportions of stair users. The data were meta-analysed using Stata V.13 (STATA. Release V.13. Statistical software. College Station. Texas, USA: StataCorp LP; 2013). We carried out a random-effects model of the pooled OR across the whole 34-year period. In addition, we examined the pooled ORs for interventions at an early and later period, based on a median split of estimates over time; the early period comprised studies published between 1980 and 2007 (n=31 estimates), and the recent period, 2008–2014 (n=26 estimates).
The studies' heterogeneity was estimated as weight and a forest plot generated to show the effect size associated with each study. The estimates included in this study showed high heterogeneity due to different study designs, different length of pre follow-up and post follow-up time periods, use of different stair use signs, and pooling and splitting of some study outcomes. For this reason, we adjusted for heterogeneity and for multiple testing in the second phase of analysis.
The second part of the analysis used a form of sequential meta-analysis,35 with α-spending function and cumulative z-curves monitoring boundaries36 used to evaluate the evidence of change, while accounting for heterogeneity of the estimates and repeated testing of significance. We used the α-spending function as a method to ensure that the significance level did not exceed 0.05 at each step in the sequential analysis, as data from each additional study were included in the analysis.37 The critical α values transformed into their corresponding cumulative z-scores estimates were compared with a z-curve monitoring boundary which identified the cumulative evidence for intervention effects with each added study estimate. Based on the median baseline estimate of stair use across studies, we specified a threshold effect of a 10% baseline rate of stair use, and a post-intervention effect of 20%, with a maximum type I error of 5% and a maximum type II error of 10% (90% power). This model provided information to demonstrate or reject an OR increase of 2 (a priori estimate) in post-intervention stair use compared with the assumed 10% pre-intervention control for stair use studies. The baseline rate of 10% was chosen as it was very close to the median of baseline stair use estimates in studies included in the meta-analysis.
The α-spending function and cumulative z-curves monitoring boundaries were based on Sidik-Jonkman reciprocal of the study-specific variance and across-study variances.37 The conventional fixed-sample, two-sided significance level of 0.05 was used, with a critical z-value fixed at 1.96 added as a reference. While the sequential meta-analysis accounts for heterogeneity and repeated significance testing, sensitivity analysis was carried out by repeating each analysis after the removal of 19 studies that had extreme ORs (≥7), see online supplementary table A1. The trial sequential analyses with random-effects models were performed using the trial sequential analysis programme.35
Results
Pooled data from the included studies comprised 416 565 observations at baseline (including 19 estimates with zero pre-intervention stair use), and 626 809 observations post-intervention. Across the 57 estimates, the median baseline stair use rate was 8.1% (IQR 0–32.6%) and median post-intervention stair use rate was 17.4% (IQR 1.6–33.8%).
The median absolute increase (post-proportion minus pre-proportion of stair users) was 2.2% (IQR 1.1–6.4%) and the median relative increase ((post-pre)/pre) was 16.9% (IQR 7.4–54.8%). The baseline–post-intervention absolute and relative increases did not differ by period, when intervention estimates were divided into early and late periods (data not shown).
The meta-analysis for earlier (1980–2007), later (2008–2014) and overall studies (1980–2014) indicated that over the whole 34-year period, the likelihood of stair use following the signage intervention was increased by 52% (OR 1.52, 95% CI 1.37 to 1.70, shown in figure 2). The effect was an increase in the likelihood of stair use of 44% following signs in the earlier period (OR 1.44, 95% CI 1.26 to 1.63), and by 85% (OR 1.85, 95% CI 1.49 to 2.29) in the recent period. The estimated variations in OR attributable to the studies' heterogeneity (I2 statistics) were similar for overall, earlier and later periods (97.5%, 97.6% and 97.4%, respectively, see figure 2), indicating high heterogeneity among studies.

Forest plot of the preintervention and postintervention stair signage effects; studies published from 1980 to 2007 (upper half), later studies published from 2008 to 2014 (lower half of panel) and overall effect size.
Sequential meta-analysis
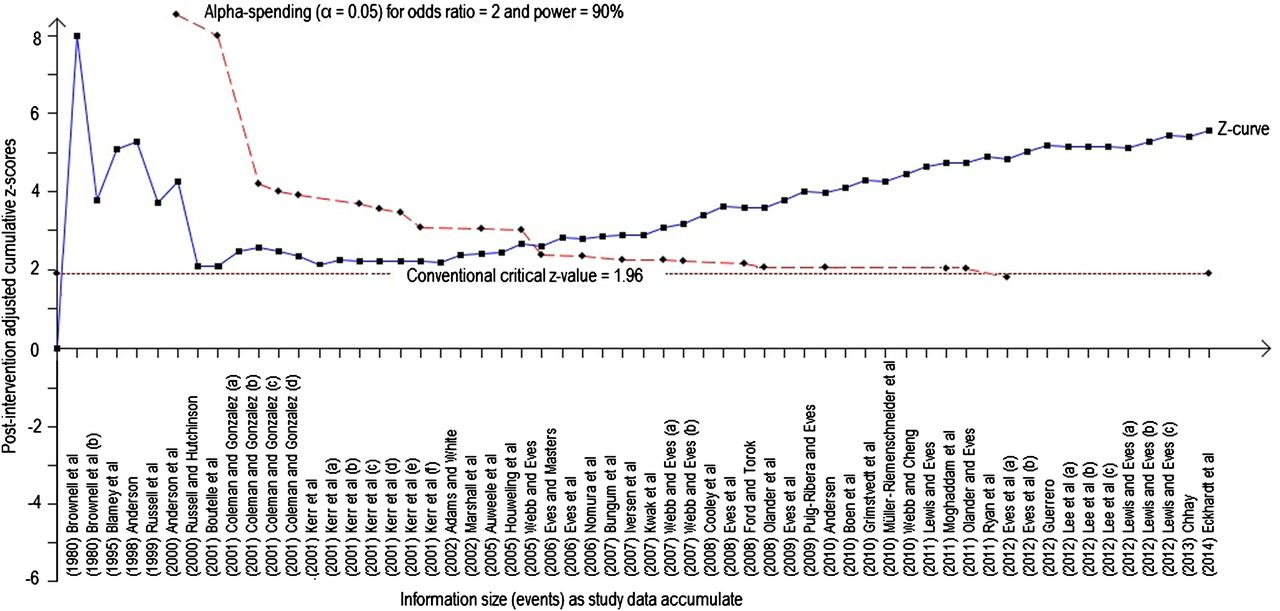
The second set of analyses focused on identifying the point at which the evidence base on stair use signage was sufficient for generalisable public health action using a sequential meta-analysis. We present the z-curve monitoring boundary to assess the evidence provided by each study sequentially. The threshold boundary curve is shown in figure 3 as the dashed line (negative slope from left to right), against which z-scores of the data from each study are compared (solid line).
{kind=link}
{kind=link}
{kind=link}
Trial sequential analysis showing the effects of stairs signage interventions published from 1980 to 2014, with heterogeneity and multiple testing adjusted.
Figure 3 shows results from the sequential analysis of all studies from 1980 to 2014. Just considering the study estimates, even the first studies were informative, as the lower line shows that these interventions increased stairs use (ie, the cumulative z-curve crossed the nominal z-value of 1.96 following the first publication). However, due to low volume of pedestrian traffic (events) in the initial studies, this inspection lacks the power to show a significant post-intervention effect of 20%.
As more studies were added, the sequential analysis accounted for the studies heterogeneity and multiple testing to show the point where the observed studies' sequential cumulative z-scores estimates and the monitoring threshold lines cross (study #24). This is the point at which there is enough accumulated evidence that signage interventions definitively increase stair usage significantly (arrow in figure 3). This corresponds to research published in 2006, suggesting that signage studies published beyond that date did not contribute further to the evidence base on intervention effect sizes.
Data using the z-curve monitoring boundary was also carried out for each period, and are shown in the online supplementary appendix figures A1 and A2. Online supplementary figure A1, for the earlier period 1980–2007 alone, shows the same result as figure 2, namely that the threshold point for sufficient evidence is achieved by 2006. Considering only studies in the later period starting in 2008 (see online supplementary figure A2), the threshold point was achieved by 2011. This result suggests that even if no stair sign studies had been conducted prior to 2008, the studies conducted from 2008 to 2011 alone provided sufficient evidence that these interventions are effective at encouraging stair use.
Sensitivity analysis
Sensitivity analysis was performed by removing the studies with the highest heterogeneity values. This reduced the effect sizes of the outcome and revealed that the initial studies had the power to show evidence on intervention effect sizes.
Discussion
This review and meta-analysis provides evidence that motivational signs increase the likelihood of stair use by over 50%, with the pooled evidence remaining consistent since 2006. Sensitivity analysis, which excluded studies with OR≥7 showed that the initial study published in 1980 had enough power to reveal evidence of effectiveness of stair use interventions. There is a 30+ year history of these types of interventions; the evidence showed a slightly higher effect size in the recent studies, but this was not significantly different to the effects observed in the early studies.
The absolute effect size of a 2.2% increase in stair use pooled across 57 estimates in this review, is very similar to summary estimates reported earlier.18 ,20 These earlier reviews also noted that effect sizes were similar, irrespective of baseline stair use levels or the duration of intervention.20
One review considered that motivational and directional signs were better than motivational messages alone, but there were too few studies to assess incremental benefit of stairwell improvements.21 There is some suggestion that the initial short-term impact is greater than repeated sign studies over a longer period.3 Nonetheless, their repeatedly stated ‘potential’, if applied to populations, could contribute to lifestyle incidental physical activity only if they are scaled up to the population level.
Stair promoting interventions are inexpensive. An economic appraisal of the costs and benefits of physical activity interventions has shown that point of decision signs are the least costly investments for governments interested in promoting physical activity.38 They demonstrate the greatest cost-effectiveness in terms of costs per unit change in physical activity in the population; although their individual effects are small, these summate to a population effect on physical activity if many inactive people become engaged in stair use.38
The major concern with stair use studies is not their lack of evidence, but their lack of translation testing at a population-wide scale. Almost all stair sign studies conducted to date have assessed the short-term impact of motivational signs, placed in a single, or in some instances multiple, locations, usually shopping malls or rail stations. There is almost no evidence of external validity in these studies.21
The present review identified that there was clear evidence of effectiveness by 2006, yet for the last decade researchers have explored minor variations to protocols or to behavioural theory, rather than testing these interventions at the population level. Thus, despite a history of stair use studies, with consistent positive results, their scalability, adoption and fidelity are not known, and the scaled up evaluation in implementing stair signs in many hundreds of public sites has not occurred.
The disconnection between the needs of researchers, practitioners and policymaker is well characterised by this type of intervention. Stair use signs are low cost and have the potential to be applied across whole communities. Therefore, this type of intervention is of interest to policymakers looking for evidence-based approaches which can be widely implemented at low cost. Given the ‘parallel universe’ inhabited by researchers,39 researchers have continued to test motivational signs in localised settings, unconnected to policymakers' needs. On the other hand, policymakers think that the evidence is complete, given the large number of ‘scientific studies’, and are not aware of the need to re-evaluate the feasibility of implementation at scale. For example, will the simplicity of the marketed stair use messages be counter-productive for health promotion by creating a naïve community perception that health gain can be achieved by occasional stair use alone? Barriers to stair use signs also need systematic investigation; such signs may be seen to restrict shopping centre advertising opportunities, cause injury risk concerns (under building codes and occupational health legislation), and might pose security issues in airports and some hotels. All of these proposed barriers are speculative, but would seem to be useful directions for the next generation of studies, assessing feasibility prior to scaling up interventions. This evaluation step is known as ‘translational formative research’,40 and precedes the dissemination of public health interventions.
Despite the lack of translational research, some government agencies, including Health Canada41 and an Australian state Government42 have developed stair use signs and sent them out to a myriad of agencies, but no follow-up assessment occurred. Process evaluation of these policy actions at scale is not reported, and their reach and implementation is not known. Future agency-level dissemination of stair signage could benefit from specific researcher–policymaker collaboration.43
Strengths and limitations
Strengths of this study included the methods that enabled pooling of estimates despite study heterogeneity. We confined our analyses to studies with signs only, and excluded additional components of sign-based interventions such as stairwell improvements. The reason for this was for comparability among interventions and because this most minimalist intervention is most replicable in the real world. Further, we modelled these data using a ‘hypothetical effect to detect’; this presumed a 10% baseline rate of stair use, and a rate of 20% post-intervention; if we had chosen a smaller baseline, ∼5%, and attempted to identify an effect of 10% post-intervention, then the threshold would have been crossed even earlier. We did not specifically audit generalisability measures in the included studies (see ref. 21), although in the context of the current paper, it is perhaps more important to note the lack of translational formative evaluation and assessment of subsequent research undertaken at a population scale.
Conclusion
The clear evidence of effectiveness of stair-promoting interventions is contrasted with their limited public health application. This review has demonstrated that the number of stair use reports that have proliferated in the research literature in the past decade has not added to the evidence base on their established efficacy. Different kinds of research should be carried out, comprising future testing of the real-world potential of stair signage interventions and their implementation at scale. Three decades of research in this area has not resulted in substantial dissemination into the population, and the promise of stair use interventions is not advanced by further repetition of the research conducted in the past decade. Research partnerships are needed between researchers and policymakers to conduct specific scaling-up assessment.43 This collaborative research is needed to answer the key question; not ‘Can these interventions work?’, but ‘Is there a realistic potential for stair use interventions to be delivered at a population scale?’
References
Footnotes
Contributors AB conceived the study idea; KF and ML undertook the searches; KM and ML undertook the review and data extraction; MK undertook the data analysis; AB and KM developed the manuscript with assistance from MK; all authors approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data from this study are included in this manuscript. The original data which were used in the meta-analysis are published in the original studies.