Article Text

Abstract
Objective The aim of this paper was to identify the key factors of case management (CM) interventions among frequent users of healthcare services found in empirical studies of effectiveness.
Design Thematic analysis review of CM studies.
Methods We built on a previously published review that aimed to report the effectiveness of CM interventions for frequent users of healthcare services, using the Medline, Scopus and CINAHL databases covering the January 2004–December 2015 period, then updated to July 2017, with the keywords ‘CM’ and ‘frequent use’. We extracted factors of successful (n=7) and unsuccessful (n=6) CM interventions and conducted a mixed thematic analysis to synthesise findings. Chaudoir’s implementation of health innovations framework was used to organise results into four broad levels of factors: (1) ,environmental/organisational level, (2) practitioner level, (3) patient level and (4) programme level.
Results Access to, and close partnerships with, healthcare providers and community services resources were key factors of successful CM interventions that should target patients with the greatest needs and promote frequent contacts with the healthcare team. The selection and training of the case manager was also an important factor to foster patient engagement in CM. Coordination of care, self-management support and assistance with care navigation were key CM activities. The main issues reported by unsuccessful CM interventions were problems with case finding or lack of care integration.
Conclusions CM interventions for frequent users of healthcare services should ensure adequate case finding processes, rigorous selection and training of the case manager, sufficient intensity of the intervention, as well as good care integration among all partners. Other studies could further evaluate the influence of contextual factors on intervention impacts.
- case management
- frequent users
- implementation
- outcomes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The 13 studies included in this paper were identified by a rigorous search strategy used in a previous review of case management (CM) interventions for frequent users of healthcare services.
Material from qualitative studies was not included in the analysis.
Little description of CM interventions was provided in the included studies.
Introduction
Frequent users of healthcare services are a small group of patients accounting for a high number of healthcare visits, often emergency department (ED), and important costs.1–3 They use healthcare services for complex health needs,4–6 combining multiple chronic conditions with psychosocial or mental health comorbidities.5 7 8 Frequent use of services is often considered inappropriate7 9 and may be a symptom of gaps in accessibility and coordination of care.10 11 These patients are more at risk for incapacity, poorer quality of life and mortality.12–15 Regardless of healthcare setting, case management (CM) is the most frequently implemented intervention to improve care for frequent users of healthcare services and to reduce healthcare usage and cost.16 17
CM is a ‘collaborative process of assessment, planning, facilitation and advocacy for options and services to meet an individual’s health needs through communication and available resources to promote quality cost-effective outcomes’.18 Reviews reported positive outcomes associated with CM interventions among frequent users of healthcare services such as decreases in ED use and cost.16 17 19–21 They also concluded that CM interventions resulted in a better use of appropriate existing resources22 and a reduction in social problems such as homelessness and drug and alcohol abuse.22–24
A small number of systematic reviews briefly addressed enabling factors of successful CM interventions in the discussion section of their paper. In a review on the effectiveness of CM among frequent ED users, Kumar and Klein19 noted that frequency of follow-up, availability of psychosocial services, assistance with financial issues and active engagement of the case manager and the patient were important characteristics of CM interventions. Oeseburg et al 25 evaluated the effects of CM for frail older people (not necessarily frequent users) and highlighted that well-trained case managers with competent skills in designing care plans and coordinating services, effective communication and collaboration between the members of the healthcare team, as well as the acceptance of the case manager as the coordinator for care delivery, were key factors of CM. However, the identification of key factors of CM interventions was not a primary objective of these reviews, although this information would be useful to inform researchers and decision makers on the implementation of CM.
The aim of this paper was to identify the key factors of CM interventions among frequent users of healthcare services found in empirical studies of effectiveness.
Methods
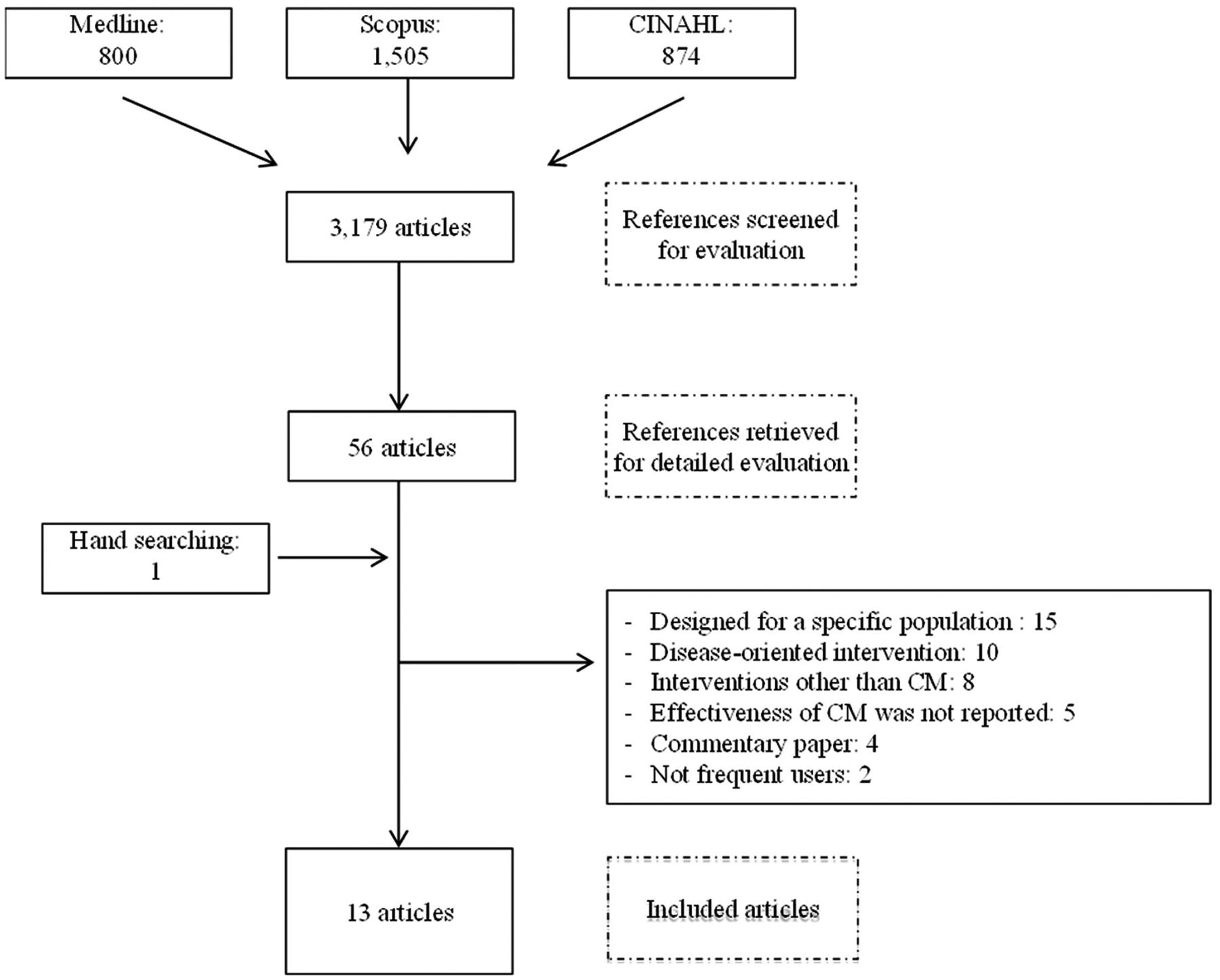
We first conducted a scoping review that aimed to report the effectiveness of CM for frequent users of healthcare services, using the Medline, Scopus and CINAHL databases covering the January 2004–December 2015 period, with the keywords ‘CM’ and ‘frequent use’.20 To be included in the review, studies had to report on the effects of a CM intervention on healthcare usage and/or cost. We excluded studies limited to a specific group of patients and interventions targeting a single disease. The review included 11 articles and concluded that CM could reduce healthcare use and cost. A detailed description of the articles included and the CM interventions is provided in the published review.20 For the purpose of this paper, the search strategy was updated to July 2017, therefore, two additional articles were added (figure 1), for a total of 13 studies.

{kind=link}
Scoping review flow chart of search results (2004–July 2017). CM, case management.
We then extracted factors of successful (n=7) and unsuccessful (n=6) CM interventions to conduct a mixed thematic analysis to synthesise findings across the studies26–28 using a framework proposed by Chaudoir et al. 29 This framework was developed to reflect factors hypothesised to impact outcomes and was used to capture the characteristics of CM interventions, while allowing comparisons among the studies included. According to this framework, the relevant factors were organised into four broad levels to address in the implementation of a health innovation: (1) environmental/organisational level: setting and structure in which CM is being implemented, including physical environmental, public policies, infrastructures, economical, political and social contexts and different features of the organisation (eg, leadership effectiveness, organisational culture and staff satisfaction towards the organisation); (2) practitioner level: characteristics and experience of the provider who is in contact with patients for the purpose of CM, including attitudes and beliefs towards CM, professional role and capacities; (3) patient level: characteristics and experience of the patient, including motivation, perception, personality traits, risk factors, skills and abilities and (4) programme level: aspects of CM, including characteristics and activities (evaluation, patient education, self-management support, referrals, transition, etc) as well as compatibility of the intervention with the organisation and adaptability.29–31
Results
Description of the studies
The 13 studies are described in table 1. Seven studies (two non-randomised controlled studies32 33 and five before–after studies34–38) reported positives outcomes on healthcare usage or cost. Wetta-Hall37 evaluated a multidisciplinary CM intervention among frequent ED users and demonstrated a decrease in ED use as well as an improvement in physical quality of life. Crane et al 32 assessed a multidisciplinary CM intervention including a care plan among frequent ED users and observed a decrease in ED use and healthcare cost. Shah et al 33 conducted a study with low-income, uninsured patients on the implementation of a care plan by a case manager and demonstrated that ED use, as well as cost, had significantly decreased. Pillow et al 34 conducted a before–after study with the top ED frequent users to measure the impact of a multidisciplinary CM intervention including a care plan and reported a trend towards a decrease in ED use. Rinke et al 35 in a study evaluating the impact of the implementation of a care plan by a case manager for the most frequent emergency medical services (EMS) users, as well as Tadros et al,36 in a study evaluating a CM intervention conducted by a case manager among frequent EMS users, observed a decrease in EMS cost and use. Finally, Grover et al 38 evaluated the effectiveness of a multidisciplinary CM intervention including a care plan among frequent ED users and reported a reduction in ED use and radiation exposure, improved efficacy of referral, but no change in number of admissions.
Description of the studies evaluating CM interventions among frequent users of healthcare services
Six studies reported no benefit on healthcare usage or cost, including three randomised controlled trials,39–41 two before–after studies8 22 and one non-randomised controlled study.42 The study by Bodenmann et al 39 on the effectiveness of a multidisciplinary CM intervention including a care plan and the pilot study by Lee and Davenport8 on a nurse CM intervention reported no change on ED use. Peddie et al 42 came to the same conclusion in a study evaluating the impact of a management plan on the frequency of ED visits. Sledge et al 41 conducted a study to evaluate a clinic-based ambulatory CM intervention and reported no significant change on number of admissions, ED use, total healthcare cost, quality of life and patient satisfaction. In a study evaluating the effectiveness of multidisciplinary CM, Phillips et al 22 observed an increase in ED use and no change on admissions. Similarly, in a study on a care coordination programme including care planning by a general practitioner and CM intervention, Segal et al 40 reported an increase in total healthcare and outpatient costs and no change on admissions and medication costs, as well as quality of life.
Key factors of CM intervention
Successful and unsuccessful factors of CM interventions are shown in tables 2 and 3, classified according to Chaudoir et al’s29 framework.
Characteristics of case management studies reporting positive findings, presented according to Chaudoir’s framework
Characteristics of CM studies reporting no benefit, presented according to Chaudoir’s framework
Most authors reported t hat access to, and close relationships between, case managers and their partners (healthcare providers at the hospital and clinics, staff from community organisations, etc) were key factors of CM interventions as well as engagement and involvement of healthcare and community partners.8 33 34 38 Two studies reported lack of collaboration between the case manager and primary care providers and lack of integration into a systemic approach to care as major flaws.8 41
The selection and training of the case manager was also mentioned as a key factor. A dedicated, trusting and experienced case manager could improve patient engagement in CM and foster better patient involvement in self-management.32 34 35 Conversely, authors of two studies highlighted the difficulty of finding a well-trained case manager as a main limitation of their study.22 41 Engagement of the case manager, as well as all the healthcare providers involved in the intervention, and their capacity to motivate the patient were also important, highlighting the need of having practitioners who feel buy-in in regard to the intervention.34
Pillow et al 34emphasised the importance of recruiting patients with greatest needs, namely very high ED users with complex healthcare needs. In three studies that did not demonstrate benefit, many patients did not have complex needs and/or were not the highest users of healthcare services,39 40 or had substance abuse or psychosocial issues without a chronic condition.22
Coordination of care,35 36 patient education and self-management support,8 32–34 and assistance to navigate in the healthcare system33 35 37 were key activities of successful CM interventions. Most of the studies included a care plan based on an evaluation of patient needs; five observed a reduction in healthcare use,32–35 38 whereas four reported no benefit.39–42 Revision of the care plan by a multidisciplinary team during the CM intervention, in response to a better understanding of patient needs or to a change in patient health condition seemed an important factor.34 35 38 Frequent contacts with the patient, either by telephone or in person, were also useful.32 33 35
Discussion
This paper is the first thematic analysis review synthesising key factors of CM interventions among frequent users of healthcare services. Access to, and close partnerships with, healthcare providers and community services resources were key factors of CM interventions that should target patients with the greatest needs and promote frequent contacts with the healthcare team. The selection and training of the case manager was also an important factor to consider in order to foster patient engagement in CM. Coordination of care, self-management support and assistance with care navigation were key CM activities. The main issues with unsuccessful CM interventions were problems in case finding or lack of care integration.
In a series of reports from The King’s Fund about the implementation of CM for people with long-term conditions, Ross et al 43 stressed the role and skills of the case manager, appropriate case finding and caseload, single point of access for patients, continuity of care, self-management support, interprofessional collaboration and development of information systems for the effective use of data and communication processes. Convergent findings were reported in a synthesis by Berry-Millett and Bodenheimer44 that aimed to examine the impact of CM to improve care and reduce healthcare costs for frequent users with complex needs. They identified six factors of successful CM, namely selecting high-risk patients, promoting face-to-face meetings, training case managers with low caseloads, creating multidisciplinary teams where physicians and case managers work in the same location, involving peers and promoting self-management skills. Our review, which aimed to identify key factors of CM as a primary objective, corroborates and completes these results, by a rigorous thematic analysis of 13 empirical studies on the topic.
As already noted by other authors,45 context description was lacking in most studies. As a complex intervention, CM includes various components interacting in a nonlinear way to produce outcomes that are highly dependent on context and variables across settings.46 47 Special attention should be paid to contextual factors of CM. Indeed, further studies could analyse not only if and how CM works for frequent users of healthcare services but also in what contexts.
Limitations
Description of CM interventions was a limit of many studies included. According to the International Classification of Health Interventions ,48 the coordination target for what was done was different in the studies. Including material from qualitative studies could enrich results in further steps.
Conclusions
CM interventions for frequent users of healthcare services should ensure adequate case-finding processes, rigorous selection and training of the case manager, sufficient intensity of the intervention and good care integration among all partners. Other studies could further evaluate the influence of contextual factors on intervention impacts.
Acknowledgments
The authors thank Ms Susie Bernier for her editorial assistance.
References
Footnotes
Contributors CH and M-CC developed the study and participated in its design and coordination. ML conducted the data collection and drafted the manuscript under the supervision of CH and M-CC. All authors were involved in drafting and editing the manuscript.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Patient consent None.
Provenance and peer review Not commissioned; externally peer reviewed.