Article Text

Abstract
Objectives To establish a unique sample of proarrhythmia cases, determine the characteristics of cases and estimate the contribution of individual drugs to the incidence of proarrhythmia within these cases.
Setting Suspected proarrhythmia cases were referred by cardiologists across England between 2003 and 2011. Information on demography, symptoms, prior medical and drug histories and data from hospital notes were collected.
Participants Two expert cardiologists reviewed data for 293 referred cases: 130 were included. Inclusion criteria were new onset or exacerbation of pre-existing ventricular arrhythmias, QTc >500 ms, QTc >450 ms (men) or >470 ms (women) with cardiac syncope, all secondary to drug administration. Exclusion criteria were acute ischaemia and ischaemic polymorphic ventricular tachycardia at presentation, structural heart disease, consent withdrawn or deceased prior to study. Descriptive analysis of Caucasian cases (95% of included cases, n=124) and culpable drug exposures was performed.
Results Of the 124 Caucasian cases, 95 (77%) were QTc interval prolongation-related; mean age was 62 years (SD 15), and 63% were female. Cardiovascular comorbidities included hypertension (53%) and patient-reported ‘heart rhythm problems’ (73%). Family history of sudden death (36%) and hypokalaemia at presentation (27%) were common. 165 culpable drug exposures were reported, including antiarrhythmics (42%), of which amiodarone and flecainide were the most common. Sotalol, a beta-blocking agent with antiarrhythmic activity, was also common (15%). 26% reported multiple drugs, of which 84% reported at least one cytochrome (CYP) P450 inhibitor. Potential pharmacodynamics interactions identified were mainly QT prolongation (59%).
Conclusions Antiarrhythmics, non-cardiac drugs and drug combinations were found to be culpable in a large cohort of 124 clinically validated proarrhythmia cases. Potential clinical factors that may warn the prescriber of potential proarrhythmia include older women, underlying cardiovascular comorbidity, family history of sudden death and hypokalaemia.
- epidemiology
- proarrhythmia
- QT interval prolongation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The Drug-induced Arrhythmia Risk Evaluation study has allowed the development of a cohort of cases of proarrhythmia.
These cases have provided crucial safety information, as well as underlying clinical and genetic data.
Only patients who did not die as a result of the proarrhythmia could be included.
Referral of cases by cardiologists alone may have led to the underestimation of the prevalence of drug-induced arrhythmia from non-cardiac drugs.
The analysis of ethnicity and differences in risk of QT prolongation could not be investigated.
Introduction
Drug-induced arrhythmia, or proarrhythmia, is the induction or exacerbation of cardiac arrhythmia associated with administration of a drug. The majority of drug-induced arrhythmic events relate to marked prolongation of the QT interval of the ECG, which can lead to the distinctive polymorphic ventricular tachycardia (VT) and ‘Torsades de Pointes’ (TdP), which in turn may lead to ventricular fibrillation (VF) and sudden death.1 This is also known as the acquired long QT syndrome (aLQTS). Occasionally polymorphic and monomorphic VT without QT prolongation can occur.2 3 In addition to drugs, other causes of aLQTS include endocrine disorders,4 cirrhosis,5 HIV and AIDS,6 inflammation and immunity,7 autoimmune disease,8 structural heart disease,9 electrolyte imbalances10 and eating disorders.11
Drug-induced arrhythmia is associated with the use of cardiovascular agents (particularly class III antiarrhythmic drugs) and also with many non-cardiovascular indicated drugs within different therapeutic categories, including antihistamines, antipsychotics and antimicrobials; an up-to-date list is maintained on the CredibleMeds register (Azcert, https://crediblemeds.org/). Currently, there is substantial evidence to support a clear association between over 50 different drugs and risk of TdP, even when taken according to the terms of the marketing authorisation, with a number of these being withdrawn from the market.12–14 Mechanistic proposals for clinical features such as electrolyte imbalance include block of the rapid form of the delayed rectifier potassium current (IKr) in cardiomyocytes.15–17 Genetic factors have also been identified. These include single nucleotide polymorphisms in the NOS1AP gene encoding the nitric oxide synthase 1 adaptor protein18; and mutations in potassium channel genes KCNH2, KCNQ1, KCNE1 and KCNE2 and/or the sodium channel gene SCN5A.19 20 Such mutations are also recognised to cause congenital long QT syndrome (cLQTS).21 Other notable risk factors include female sex, bradycardia, recent cardioversion, pre-existing electrolyte disturbance, elevated plasma concentrations and/or rapid infusion of QT-prolonging drugs and digitalis toxicity.22–24
Following the removal of several QT-prolonging drugs because of associated sudden deaths,25–28 risk minimisation strategies were introduced to mitigate the arrhythmic risk posed by drugs, including clinical studies to assess the proarrhythmic potential for a new drug within the premarketing development programme.29 However it has been recognised that there remain limitations in the conduct of clinical studies designed to evaluate a drug’s potential for QT prolongation and applicability of results to vulnerable patients.30 Because of the unpredictable nature of the condition, the Drug-induced Arrhythmia Risk Evaluation (DARE) study aimed to improve the understanding of the epidemiology of proarrhythmia by establishing a cohort of cases of drug-induced arrhythmia reported throughout England, to characterise typical patients with proarrhythmia and to describe the drugs found to be culpable in these cases of proarrhythmia. This manuscript is a per-protocol descriptive analysis of risk factors for the condition and the contribution of individual drugs to the risk of drug-induced arrhythmic events.
Methods
Study design and setting
Cardiologists across England were notified of the study by the British Pacing and Electrophysiology Group and the British Cardiac Society and asked to recruit patients. Study awareness and participation was further promoted by project presentation and local interaction across the country. Cases of suspected proarrhythmia were referred by cardiologists in England between March 2003 and July 2011. All consenting cases attended a face-to-face interview with a regional study nurse (North, South or Midlands regions) between May 2005 and August 2011.
Participants
Cases of proarrhythmia were included if they had one or more of the following criteria, all diagnosed as secondary to therapeutic drug administration or overdose: documented TdP, VF or VT (polymorphic or monomorphic, not associated with QT prolongation); exacerbation of pre-existing non-sustained arrhythmias to sustained; severe prolongation of the QTc interval corrected using Bazett’s formula (>500 ms) without symptoms; or moderate prolongation of the QTc interval (≥450 ms in men or ≥470 ms in women) with a clinical history of cardiac syncope.
All cases were reviewed by at least two experienced cardiologists, using hospital notes and interview questionnaire information, to ensure appropriate inclusion of cases. Patients with acute ischaemia, ischaemic polymorphic VT and structural heart disease (using symptoms, history of ischaemia and associated therapy, risk factors or ECG, stress test and coronary angiography results) were excluded. Case presentation (asymptomatic, syncope, VT, VF and/or TdP) and aetiology (QT prolongation-associated and non-QT prolongation-associated) were ascertained. Drugs received by the patient were adjudicated for culpability in contributing to proarrhythmia according to the clinical data, timing of medication and the presenting event that prompted referral. Prior reports of association with proarrhythmia were also taken into account, although drugs thought to contribute to causation but without such data were not excluded.
No sample size calculation could be performed for the study as, at the time of study initiation, the natural history, relative risk and potential risk factors of proarrhythmia were largely unknown.
Variables
A proforma questionnaire obtained patients’ self-reported information on age, gender, ethnicity, weight, height, smoking status, alcohol consumption, symptoms before, during and after the event (including ‘blackout’, ‘near blackout’, ‘dizziness/light-headedness’ and ‘palpitations’), medication taken before, during and after the event (including prescription, over-the-counter/herbal and recreational), any medical and cardiovascular history (including angina, myocardial infarction, ‘heart failure’, ‘heart valve problem’, ‘heart rhythm problem’, ‘high blood pressure’, hypokalaemia, hypothyroidism, diabetes mellitus, ‘stroke’, transient ischaemic attack, ‘liver problem’, ‘kidney problem’) and family medical history (including ‘sudden death’ and ‘unexplained blackout’). History of proarrhythmic events was validated using each patient’s hospital notes and an ECG taken at the time of the interview. Patient hospital notes, where available, were also used to validate drug history (including the drug(s) considered to be related to the proarrhythmic event), and medical and cardiovascular history for all cases.
Culpable drugs were mapped to the Anatomical Therapeutic Chemical classification system. The drugs were then classified according to the CredibleMeds register risk of causing QT prolongation and/or TdP into the following groups: known risk, possible risk, conditional risk and no known risk. Drugs are classified as having known risk when there is substantial evidence for QT interval prolongation and TdP risk when used according to the label; possible risk when there is substantial evidence for QT interval prolongation but insufficient evidence of TdP risk when used according to the label; and conditional risk when there is substantial evidence for QT interval prolongation and TdP risk but only under specific conditions (eg, overdose, interaction with another drug). Drugs were also classified according to cytochrome (CYP) P450 activity (inhibitors and inducers), and potential pharmacodynamics interactions were identified using the Drug Interaction Checker (Medscape). Potential pharmacodynamics interactions were classified into one of the following groups: QTc prolongation; cardiotoxic (non-QTc prolongation-related but other cardiac effect likely, eg, bradycardia or other dysrhythmia); conditional (cardiac effect unclear but drug interaction has an impact on a proarrhythmic risk factor, eg, potassium levels); and other (non-cardiovascular) or no drug interaction.
Statistical methods
Statistical analysis involved descriptive statistics, including measures of central tendency and dispersion for continuous variables (mean, SD, median, range and percentiles) and frequencies with proportions for categorical variables. Results were also stratified according to type of arrhythmia (QT prolongation-associated and/or non-QT prolongation-associated). All statistical analyses were performed using Stata V.12. Radar plots were also constructed in order to characterise cases and estimate the contribution of individual drugs to risk of proarrhythmia. Missing information relating to patients was described using a ‘not known’ category.
Results
Case characteristics
The final overall cohort consisted of 130 cases (figure 1), who were referred from a total of 98 consultant cardiologists across England (figure 2). As the majority of cases were Caucasian (n=124, 95.4%), the analysis was performed on these individuals only. Characteristics of the final cohort of Caucasian cases are shown in table 1. Cases were 62.9% female with a median age at interview of 66 years (IQR 52–73 years). All cases were adults (≥18 years). Around a third (35.5%) had a family history of sudden death. The types of arrhythmia reported in cases are shown in table 1. The majority of cases reported TdP, VF or cardiac arrest with QT prolongation (n=79, 63.7%), of whom 56 (45.2%) presented with TdP, 13 (10.5%) presented with VF and 10 (8.1%) presented with TdP and VF. However, 23% (n=28) of cases involved VT or VF not related to QT prolongation. Median (SD) QTc values were 578 (69) ms in QT prolongation-associated cases and 466.7 (40) ms in non-QT prolongation-associated cases.

Referrals and cohort accrual.

Geographical distribution of consultant cardiologists referring proarrhythmia cases.
Characteristics of cases (n=124)
Culpable drugs
A total of 165 patient drug exposures to 42 drugs deemed culpable were identified (table 2, two drugs were unspecified). The most frequently associated drug class was the antiarrhythmics, with 70 drug exposures (42.4% of drug exposures) in 67 (54.0%) patients. Amiodarone (n=40; 24.2% of drug exposures; 32.3% of patients), flecainide (n=23; 13.9% of drug exposures; 18.6% of patients) and sotalol, a beta-blocker with class III properties (n=25; 15.2% of drug exposures; 20.2% of patients), were the most frequently reported single drug causes and known to carry a risk of QTc prolongation and/or TdP. Antibiotics (eg, erythromycin; n=5, 3.0% of drug exposures; 4.0% of patients) and antidepressants (eg, citalopram; n=7, 4.2% of drug exposures; 5.7% of patients) were also implicated.
Drugs culpable in proarrhythmia cases, stratified by risk of QT prolongation and/or Torsades de Pointes
Of the 42 culpable drugs, 14 (33.3%) drugs carried a known risk (120 (72.7%) drug exposures), 8 (19.0%) carried a conditional risk (16 (9.7%) drug exposures), 6 (14.3%) carried a possible risk (7 (4.2%) drug exposures), 1 (2.4%) carried a risk in individuals with cLQTS, and 13 (31.0%) carried no known risk of QTc prolongation and/or TdP (18 (10.9%) drug exposures). The level of risk could not be established for two drugs.
Of the 13 culpable drugs carrying no known risk of QTc prolongation and/or TdP, 2 are known to contribute to bradycardia (timolol and digoxin), 2 are ‘not classified’ according to CredibleMeds based on the evidence available (cetirizine and verapamil) and 1 remains under active review (lofexidine).
Multiple drug combinations (table 3) were reported in 32 (25.8%) patients. Specifically, 27 (21.8%) patients reported two drugs, 2 (1.6%) patients reported three drugs, 2 (1.6%) patients reported four drugs and 1 (0.8%) patient reported five drugs. Two patients had unspecified drug combinations. Of the patients reporting more than one drug, 84.4% (27/32) reported using at least one cytochrome P450 inhibitor, with 6 (18.8%) using two or more in combination. A single patient reported using a CYP inducer. Potential pharmacodynamics interactions within patients reporting more than one drug, according to the Medscape Drug Interaction Checker, were QTc prolongation (19/32, 59.4%), cardiotoxic (3/32, 9.4%), conditional (1/32, 3.1%) and other (non-cardiovascular; 2/32, 3.6%) interactions. Seven patients (21.9%) reported a drug combination without a potential drug interaction.
Drug combinations culpable in cases of proarrhythmia
Types of arrhythmia
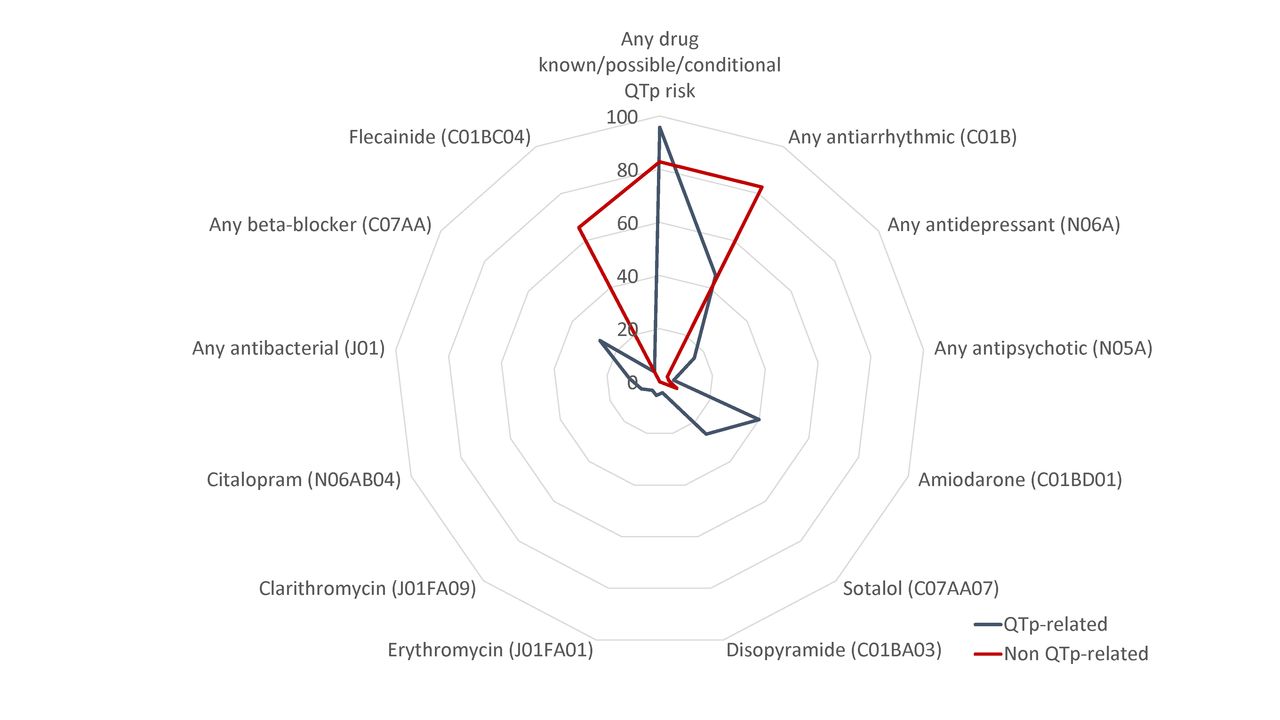
Types of proarrhythmia identified within this study included QT prolongation-related (n=95, 76.6%) and non-QT prolongation-related (n=29, 23.4%), the latter more typically associated with QRS prolongation (table 2). Stratification according to proarrhythmia type demonstrated few differences between the characteristics of QT prolongation-related and non-QT prolongation-related cases of proarrhythmia, with similar frequency of past medical conditions within both types (figure 3). Similarly drugs deemed culpable in cases of proarrhythmia were similar between these types, except for flecainide, which was more commonly implicated with non-QT prolongation-related compared with QT prolongation-related (figure 4).

Characteristics of QTp-related and non-QTp-related cases of proarrhythmia. FH, family history; QTp, QT interval prolongation; TIA, transient ischaemic attack.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Drugs (Anatomical Therapeutic Chemical codes) culpable in cases of proarrhythmia. QTp, QT interval prolongation.
Discussion
The DARE study established a cohort of 130 cases of clinically validated drug-induced proarrhythmia referred from across England. To our knowledge this is the largest single study describing a cohort of cases of drug-induced arrhythmia. This information can be used in conjunction with other methods for evaluating the risk of drug-induced arrhythmias, such as spontaneous reports, healthcare databases and active surveillance studies. An analysis of 124 Caucasian cases was undertaken. These Caucasian cases were predominantly female (62.9%) and middle-aged or elderly (median age at interview of 66 years (IQR 52–73 years)). The majority reported significant past cardiac comorbidity including heart rhythm problems (72.6%), high blood pressure (53.2%), heart valve problems (27.4%), angina (21.0%) and myocardial infarction (21.8%). This is consistent with data that demonstrate arrhythmia or heart failure to be a risk for proarrhythmia.31 Over a third of cases also had an associated family history of sudden death, supporting the potential genetic risk for drug-induced arrhythmia.21 Additionally, over a quarter of cases presented with hypokalaemia (26.6%). Hypokalaemia is associated with QT interval prolongation due to increased competitive blockade of IKr, which causes loss of function of the hERG (human Ether-a-go-go Related Gene) channel.16
Risk factors for proarrhythmia have been studied before. For example, one study demonstrated hypokalaemia, myocardial infarction, sepsis and heart failure to be risk factors for QT prolongation in both drug-induced and non-drug-induced hospitalised cases.32 Furthermore, a study of 21 patients with drug-induced QT prolongation from a Greek hospital found hypertension, female gender, paroxysmal atrial tachyarrhythmias and old age (>60 years) to be common characteristics of patients presenting with the condition.33 A study of a group of methadone users in Switzerland demonstrated greater risk of QT prolongation with hypokalaemia, higher methadone dose, altered liver function and use of P450 cytochrome inhibitors.34 Finally, a study of psychiatric patients with drug-induced LQTS showed hypokalaemia, abnormal T wave as well as hepatitis C and HIV infection to increase the risk of LQTS in this population.35
In our study amiodarone, sotalol and flecainide were the most common culpable drugs as was the antiarrhythmic drug group as a whole (42.2% of drug exposures). Their high prevalence may be due to the relative high potency of cardiac current blockade and/or reflect that cardiologists were the main referral source of cases. For example clinical trials of patients with ventricular and supraventricular arrhythmias treated with sotalol have shown a 4.3% prevalence of proarrhythmia.36 While class Ia, Ic and III antiarrhythmics carry a known risk of QT prolongation and/or TdP and can be potent IKr blockers, amiodarone is often thought of as a rare cause of TdP.37 Its importance in our cohort may be due to its relatively frequent use as an antiarrhythmic agent and/or that those most vulnerable to aLQTS (ie, elderly women with cardiac comorbidity) are more likely to receive amiodarone than other antiarrhythmics due to its perceived lower proarrhythmic risk. This is therefore an important warning to clinicians. Proarrhythmia unrelated to QT prolongation was most commonly observed in users of flecainide, recognised to result from conduction slowing, causing QRS duration prolongation.38 Amiodarone was also frequently reported to be associated with LQTS and TdP in a recent active surveillance study of 58 cases in Germany, a study that showed similar results to DARE, including the identification of hypokalaemia as a risk factor for LQTS and TdP.39
Nearly three-quarters of the culpable drug exposures were caused by drugs with known risk of QT prolongation and/or TdP, including antibiotics and antidepressants. However, 13 (31.0%) different drugs were diagnosed as culpable in proarrhythmia but not recognised as having such a risk according to the CredibleMeds register. Two are known to contribute to bradycardia (a risk for proarrhythmia), two are ‘not classified’ according to CredibleMeds based on the evidence available and one remains under active review (lofexidine). Drug combinations were also culpable in a quarter of cases, with up to five drugs being reported in combination. Of these drug combinations by far the majority, 84.4% (27/32), included at least one cytochrome P450 inhibitor. Drug combinations of antipsychotics and antidepressants have also previously been shown to increase the risk of QT interval prolongation when compared with antipsychotics alone.40 Concurrent use of more than one QT-prolonging drug or concurrent use with a drug that alters the pharmacokinetic profile of the drug is an important risk factor for adverse outcomes. On the other hand, other studies have shown no increased risk of QT interval prolongation with the use of multiple QT-prolonging drug combinations compared with single drugs.32 Furthermore, drugs with no known risk of QTc prolongation when used alone may result in prolongation of the QTc interval when used in combination. For example, ceftriaxone and lansoprazole were identified as having a risk of QTc prolongation when used together using electronic healthcare records and in vitro methodology.41 Drug interactions were also reported to represent a high proportion of cases of drug-induced TdP within a Belgium study using the EudraVigilance database (18 of 31 cases).42
Limitations of the DARE study include the inability to enrol patients who may have suffered from sudden death as a result of drug-induced arrhythmia; for ethical reasons only live patients could be included. Furthermore, as all referrals came from cardiologists, this may have resulted in selection bias and underestimation of the prevalence of drug-induced arrhythmia from non-cardiac drugs. The level of underestimation due to sudden death or cardiologist referral is difficult to quantify. Determining the cause of death in patients with sudden cardiac death is challenging, with ion channelopathies potentially accounting for 40% of cases of sudden arrhythmic death syndrome, being undetectable after a patient has died.43 A comparison with spontaneous reports of drug-induced arrhythmia might provide information on the level of underestimation of the prevalence of drug-induced arrhythmia from non-cardiac drugs; however, under-reporting of severe adverse drug reactions is known to be high, at approximately 80%.44 In addition, patient answers to questionnaires may have been subject to recall bias and some of the patient information could not be validated from patient records. Finally, differences in ethnicity could not be investigated in this group as there were too few cases of non-Caucasian ethnic origin. Ethnic differences have been shown to affect the risk of QT prolongation due to polymorphisms in cardiac ion channels.45 With a larger number of cases, ethnicity differences could be further investigated. It would also be desirable to estimate the incidence of proarrhythmia within the UK population, as has been done for a similar study.39 Future work might also involve an investigation of specific drug types and how exposure duration and patterns of usage might affect the risk of proarrhythmias.
Conclusions
Increased awareness in the past decade of the public health risk of QT-prolonging drugs has resulted in the regulatory authorities producing guidelines for studying the potential for QT prolongation in premarketing development and the adoption of risk-minimisation measures.29 However, due to rarity and diagnostic difficulties, the lack of reported TdP cases in premarketing or postmarketing safety monitoring is a challenge for drug safety.46 To date, linked epidemiological and pharmacogenetic data on proarrhythmic events have been lacking. As such, the DARE study has allowed the development of a cohort of cases that provide crucial safety information, as well as underlying clinical and genetic data.18 47 48 DARE has provided information that confirms risk factors for proarrhythmia, including patient comorbidities and use of drugs with known QTc prolongation risk. However, the study has also identified higher frequency of amiodarone as well as reports of drugs with no known QTc prolongation risk.
Caution is necessary when prescribing class I and III antiarrhythmic drugs. These include amiodarone given its frequent use in clinical practice. The prescriber needs to be aware of a patient’s concomitant medications and comorbidities, especially middle-aged to elderly women with cardiovascular disease and/or a family history of sudden death, as well as the likelihood of hypokalaemia. Furthermore prescribers must be aware of the contribution of non-cardiac drugs to the burden of drug-induced arrhythmias,49 with approximately 3% of prescriptions in the UK representing non-cardiac drugs with warnings for arrhythmic potential.50 Our findings reinforce the need for safer prescribing of proarrhythmic drugs in clinical practice.
Acknowledgments
The authors would like to thank the cardiologists who referred patients to the study, Pauline Telfer for her administrative assistance and Linda Robinson for data collection. The authors also thank the Steering Committee, the British Pacing and Electrophysiology Group (BPEG), now British Heart Rhythm Society (BHRS), and the British Cardiac Society (BCS), which were instrumental in the recruitment of patients. The authors also thank Ed Tong for his statistical support.
References
Footnotes
Contributors AJC, SAWS, ERB and DL designed the study. VM was responsible for data acquisition. ALC, DL and ERB performed the analyses. ALC, DL, VM, ERB, AJC and SAWS interpreted the findings. ALC, VM, ERB and DL wrote the first draft of the manuscript and revised subsequent versions. The other authors provided input, expertise and critical review of the paper. All authors read and approved the final version of the paper. AJC and SAWS are the guarantors.
Funding The DARE study was funded by the British Heart Foundation under special project grant SP/02/001.
Competing interests ERB was supported by grants from the international Serious Adverse Events Consortium during the conduct of the study. SAWS reports personal fees from ICON, Shire Pharmaceuticals, ONO Pharmaceuticals, Intermune Pharma and IPSEN outside of the submitted work. AJC reports personal fees from Mitsubishi, Laguna, Bayer, Biotronik, Richmond Pharmacology, Boehringer Ingelheim, Daiichi, Menarini, Novartis, St Jude Medical, Bristol-Myers-Squibb, Pfizer, Medtronic, Thrombosis Research Institute, Servier, Boston Scientific, Eli Lilly and Company, and organisational (non-commercial) fees from the European Heart Rhythm Association outside the submitted work.
Ethics approval Ethical approval was gained from the London Multicentre Research Ethics Committee (MREC), reference number MREC/02/2/73.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data available on request by emailing abigail.coughtrie@dsru.org.