Article Text

Abstract
Objectives Prevention of type 2 diabetes mellitus (TD2M) is a priority for healthcare systems. We estimated the cost-effectiveness compared with standard care of a structured education programme (Let's Prevent) targeting lifestyle and behaviour change to prevent progression to T2DM in people with prediabetes.
Design Cost-effectiveness analysis alongside randomised controlled trial.
Setting 44 general practices in Leicestershire, England.
Participants 880 participants with prediabetes randomised to receive either standard care or a 6-hour group structured education programme with follow-up sessions in a primary care setting.
Main outcome measure Incremental cost utility from the UK National Health Service (NHS) perspective. Quality of life and resource use measured from baseline and during the 36 months follow-up using the EuroQoL EQ-5D and 15D instruments and an economic questionnaire. Outcomes measured using quality-adjusted life years (QALYs) and healthcare costs calculated in 2012–2013 prices.
Results After accounting for clustering and missing data, the intervention group was found to have a net gain of 0.046 (95% CI −0.0171 to 0.109) QALYs over 3 years, adjusted for baseline utility, at an additional cost of £168 (95% CI −395 to 732) per patient compared with the standard care group. The incremental cost-effectiveness ratio is £3643/QALY with an 86% probability of being cost-effective at a willingness to pay threshold of £20 000/QALY.
Conclusions The education programme had higher costs and higher quality of life compared with the standard care group. The Let's Prevent programme is very likely to be cost-effective at a willingness to pay threshold of £20 000/QALY gained.
Trial registration number ISRCTN80605705.
- DIABETES & ENDOCRINOLOGY
- HEALTH ECONOMICS
- PRIMARY CARE
- PREVENTIVE MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Evidence on resource usage, quality of life and clinical outcomes obtained prospectively alongside the first randomised controlled trial in the UK to assess a structured education and lifestyle-based diabetes prevention programme among participants with prediabetes.
Efforts made to assess likely real-world costs of national implementation in a National Health Service (NHS) primary care setting.
Good length of follow-up (3 years) permitted cost-effectiveness to be demonstrated without reliance on long-term extrapolation.
Missing data due to economic questionnaire being introduced halfway through study and attrition in patient responses to questionnaires.
Further follow-up required to assess long-term benefits of intervention.
Introduction
Type 2 diabetes mellitus (T2DM) is a major public health problem in terms of patient morbidity, mortality and costs to the healthcare system. Individuals with T2DM experience reduced quality of life, increased healthcare costs and higher risk of long-term complications such as cardiovascular disease, stroke, heart failure, renal failure, amputation and blindness.1–3 In the UK, diabetes accounts for around 10% of total healthcare expenditure, projected to increase to 17% by 2035/20364 as the prevalence of T2DM continues to rise. Hence, there is a need to identify and implement interventions across the healthcare system aimed at preventing diabetes.
Several initiatives have been developed to promote preventative measures for T2DM, including pharmacological and surgical interventions, and behavioural strategies focusing largely on lifestyle changes such as moderate-intensity physical activity, a healthy diet and weight regulation.5 However, there is a lack of empirical evidence on how these programmes translate into UK routine clinical care. To address this gap, a pragmatic structured education intervention for prevention of T2DM within primary care pathways was developed, the Let's Prevent programme, which targets lifestyle behaviour change among individuals with prediabetes using simple, non-technical language and visual aids. The programme is based on the Diabetes Education and Self-Management for On-going and Newly Diagnosed (DESMOND) programme, the first national education programme for people with T2DM to meet the National Institute for Health and Care Excellence (NICE) criteria6 and shown to be effective and cost-effective.7 ,8
Although clinical trials have demonstrated that lifestyle interventions reduce the risk of progressing to T2DM in this population,9 it remains unclear whether these interventions represent a cost-effective use of healthcare resources, and none have been evaluated in the UK setting of the National Health Service (NHS). The primary outcome of the Let's Prevent Diabetes randomised controlled trial (RCT) was progression to T2DM during 3 years. Overall, there was a non-significant 26% reduction in the risk of developing T2DM in the intervention arm compared with standard care (p=0.18).10 A significant reduction in progression to T2DM was seen in the intervention arm compared with standard care when only those who attended all of the education sessions (ie, the initial 6 hours plus the two annual refresher sessions) were included in the analysis (LJ Gray, T Yates, J Troughton, et al. Engagement and retention critical for the success of the NHS Diabetes Prevention Programme—the Let's Prevent Diabetes Programme. Submitted 2016). In 2016, the NHS Diabetes Prevention Programme called ‘Healthier You’ was launched for adults with prediabetes, and programmes from four providers were commissioned to be delivered in specific areas of England.11 An adapted version of the Let's Prevent Diabetes programme is being delivered as part of this national programme. The programme structure was amended to fit with the NHS specification and will be delivered over a number of shorter sessions taking place over 9 months.
Alongside the Let's Prevent trial, we assessed the cost-effectiveness of a structured education intervention for prediabetes implemented in primary care compared with standard care.
Methods
We performed an incremental cost-utility analysis of structured education programme called Let's Prevent using data from the clinical trial,12 with differences in costs and effects calculated relative to the standard care group. The analysis was conducted from the perspective of the healthcare system, with wider social costs not included. Effectiveness was measured by quality-adjusted life years (QALYs), which capture differences in life expectancy and/or quality of life.
Eight hundred and eighty patients were enrolled in the cluster RCT from July 2009 to June 2011, with 447 patients (51%) in the intervention group and 433 (49%) in the standard care group.10 Those randomised to standard care received a booklet giving information on risk factors for T2DM and how physical activity and lifestyle change can be used to prevent or delay the disease. Patients randomised to the intervention group received the same booklet as those in the standard care arm but were offered an initial 6-hour structured education programme, three monthly nursing support phone calls, and a 3-hour group-based follow-on maintenance session at 12 and 24 months, described previously.10 ,12 These behaviour change techniques are similar to those in the proven and widely implemented DESMOND programme.8 ,10
Economic data collection
All participants were followed up at 6, 12, 24 and 36 months. A trial questionnaire administering the 15D quality of life instrument and capturing self-reported medication was used from baseline. Halfway through the study (May 2012, trial started on December 2009, ended on July 2014) an additional self-reported economic questionnaire was introduced, which included the EQ-5D-3L instrument and asked participants to recall primary (face-to-face and telephone contacts with general practitioners or practice nurses) and secondary care (outpatient and accident and emergency attendances and inpatient episodes and lengths of stay) contacts over the previous 12 months, as well as out-of-pocket expenses (eg, travel costs), employment status and impact on work (eg, sick days, lost earnings due to ill health). Given its introduction in mid-study, the economic questionnaire was sent to only 22 participants (2.5%) at 12 months, 408 participants (46%) at 24 months and 617 participants (70%) at 36 months.
Quality of life
We estimated the quality of life in the intervention and standard care groups using the 15D and EuroQol EQ-5D instruments. A published regression equation13 mapped 15D utility scores into EQ-5D values when 15D but no EQ-5D data were available. When EQ-5D data were available, utility values were derived using the UK social tariff.14 In the base case analysis, observed and mapped EQ-5D utility values were merged, with preference given to the former when both were available, to minimise the number of missing utility data points that had to be estimated using multiple imputation. We assumed changes in mean utility values between each time point to be straight line transitions, and weighted the average change in utility between each time point for each patient by the survival time within trial to estimate QALYs gained during the study period, equivalent to an area under the curve calculation. Differences in mean QALYs between the two groups during the 36 months of the trial were adjusted for baseline differences in utilities.
Intervention costs
The cost of the ‘Let's Prevent’ intervention was estimated at £200 per participant, which included the cost of providing the initial intervention, refreshers and support over the 3-year trial period (see online supplementary table S1). One-off costs, such as educator training and teaching materials, were also included in the intervention cost. Other trial-related costs such as clinical tests and questionnaires were not included in the analysis, as they did not differ between the trial groups and would not exist outside the trial environment. The intervention cost was divided into yearly costs based on the year in which the relevant expenditure was required. If adopted more widely, the Let's Prevent intervention cost would likely be lower due to synergies with the DESMOND programme (eg, using DESMOND trained and accredited educators to deliver Let's Prevent and conduct quality assurance). We estimate these synergies would reduce the cost from £200 per participant to £179, and explore the implications of this in the sensitivity analysis; details of these costings are provided in online supplementary table S1.
supplementary tables
Primary and secondary costs
Costs per healthcare contact in a primary care setting were calculated using unit costs obtained from standard national sources,15 including qualification costs and direct care costs where applicable. Hospital inpatient and outpatient contacts were valued using NHS reference costs 2012–2013.16 All unit costs are reported in online supplementary table S2.
Medication costs
Medication use, collected at baseline and during the trial by questionnaire from participants assisted by healthcare staff, was valued using weighted average medication unit costs from national prescribing volumes and costs17 (see online supplementary table S2). There was no evidence of a statistically significant difference (p=0.75) in medication costs at baseline between the intervention and standard care arms.
Statistical analysis
We performed a within-trial economic analysis, with total healthcare costs and QALYs gained per patient calculated for the 36 months of the trial period in the intervention and standard care groups.
To deal with missing data, multiple imputations were performed using a chained model with 60 iterations, regressed on the baseline complete covariates: age, sex, body mass index and practice code. The imputed variables were EQ-5D (observed and mapped) at 0, 6, 12, 24 and 36 months, non-inpatient costs at 24 and 36 months and medication costs at 12, 24 and 36 months. Non-inpatient costs at 12 months were not imputed as the proportion of missing data (98%) was too high to result in a valid imputation exercise; instead we used non-inpatient costs at 24 months as an approximation of 12 month costs. This was done after multiple imputation.
We accounted for clustering effects at practice level using a mixed-effects model with a random-effects component, using practice codes. Covariates were deemed statistically significant if p<0.05. Utilities were adjusted for baseline differences between the intervention and standard care groups in all subsequent analysis, using analysis of covariance. Statistical analysis was performed using Stata V.13 (StataCorp). All costs and QALYs were discounted to present values at a 3.5% annual rate, the recommended UK rate.18 We calculated an incremental cost-effective ratio (ICER) by dividing the mean cost difference between intervention and standard care groups by the mean QALY difference. We report the probability that the intervention is the most cost-effective option at a threshold of £20 000/QALY gained using the net benefit framework and Fieller's theorem.
Sensitivity analyses
Sensitivity analyses were performed to explore the impact of structural uncertainty surrounding a number of assumptions made in the analysis, notably the use of different types of clustering, the use of 15D or EQ-5D to generate QALYs, the inclusion or exclusion of incompletely reported hospital admission costs, and the use of a ‘real-world’ cost for the intervention.
Results
A high proportion of missing data in the costs and effects variables made the use of complete case analysis unreliable and prone to potential bias. Twenty-one per cent of data were missing concerning 15D utilities, and 45% concerning medication use. The degree of missing data was highest concerning variables from the economic questionnaire (EQ-5D-3L, inpatient and non-inpatient healthcare contacts) with 98%, 62% and 41% of data missing at 12, 24 and 36 months, respectively (see online supplementary table S3). Moreover, data on in-patient episodes displayed some logical inconsistencies in the reported answers, such as patients reporting zero hospital admissions overnight but spending 2 days in hospital, and incomplete length of stay information when episodes were reported. Given the unreliability of these data, inpatient costs were not included in the main analyses, but are reported in a sensitivity analysis.
Resource use and costs
Costs are summarised in table 1, and detailed resource use and costs in online supplementary table S4. There were no significant differences in medication or non-inpatient costs over the 3 years of the study, with the 95% CI around the total cost difference spanning 0.
Mean cost per patient by cost category (undiscounted)
Utilities
Mean utility scores at different time points after merging reported EQ-5D responses and responses mapped from the 15D, and after multiple imputation to deal with remaining missing values, are shown in figure 1; online supplementary table S5 reports the values on which the figure is based, plus values based on observed data alone, and based on data prior to multiple imputation. QALYs derived from these utility estimates and discounted to present values, equivalent to area under the curve calculations, are summarised in table 2. Online supplementary table S6 also reports QALYs undiscounted and following adjustment for baseline differences.
Cost-effectiveness analysis results

Mean utility scores after multiple imputation for merged EQ-5D utility (reported+mapped) by Int and Std group at different time points. (Error bars indicate CIs. Undiscounted. See online supplementary table S5 for values.) Int, intervention; Std, standard care.
QALYs over the 36 months of follow-up were slightly higher in the intervention than in the standard care arm, having adjusted for baseline differences and for clustering, but the differences were not statistically significant, with the 95% CI spanning 0 (+0.0461, 95% CI −0.0171 to 0.109).
Cost-effectiveness analysis
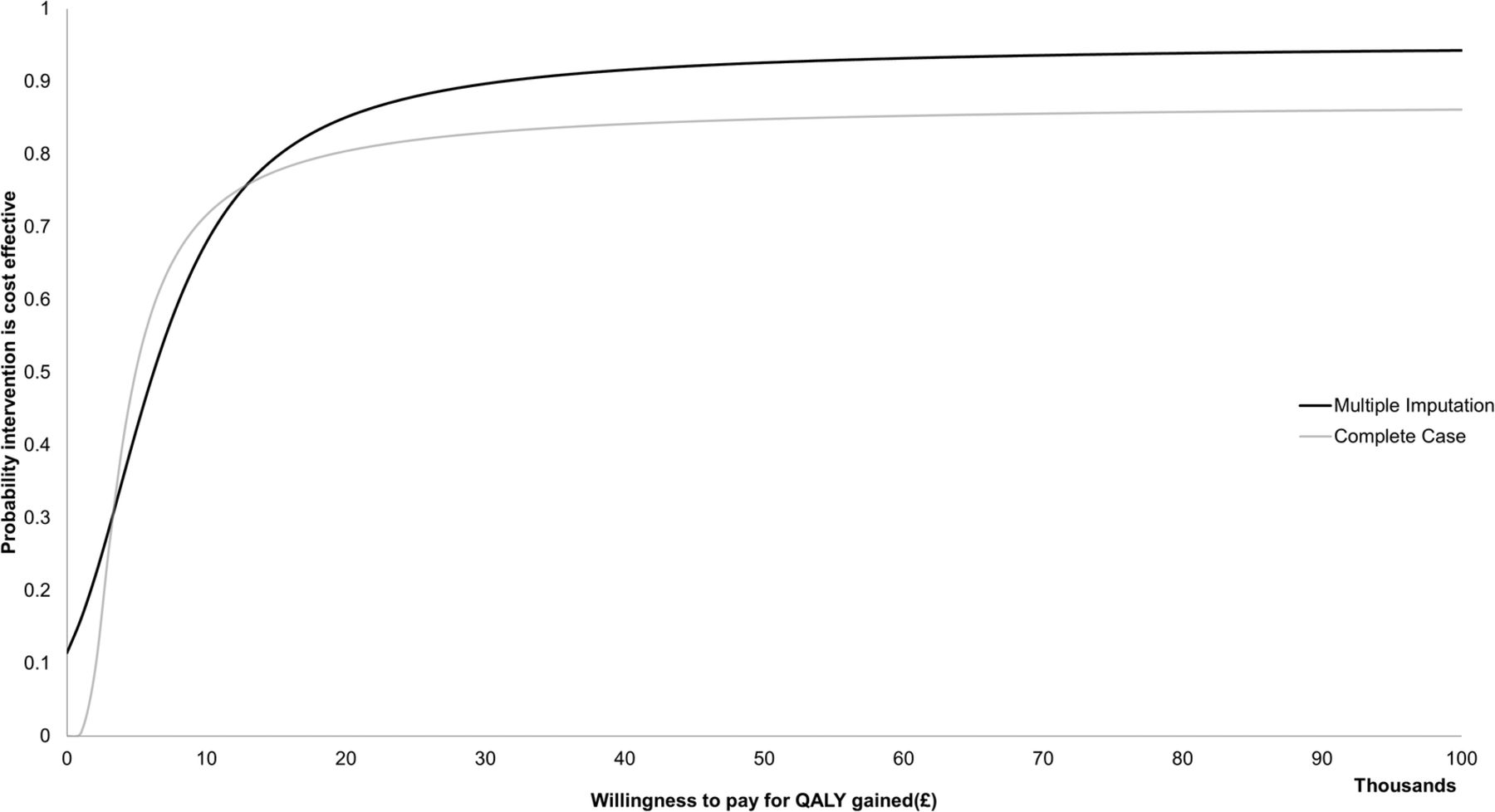
The within-trial cost-effectiveness analysis is reported in table 2, with a complete case analysis included for comparison. After accounting for clustering and missing data, the intervention group was found to have a net gain of 0.046 (95% CI −0.0171 to 0.109) QALYs over 3 years at an additional cost of £168 (95% CI −395 to 732) per patient compared with the standard care group. This gives an ICER of £3643/QALY gained, with an 86% probability that the intervention is cost-effective at a willingness to pay threshold of £20 000/QALY. Using only complete case (n=225), the ICER is £4906/QALY with an 80% probability of being cost-effective at a willingness to pay threshold of £20 000/QALY. Figure 2 shows the probability that the intervention is cost-effective at different willingness to pay per QALY ceilings, ranging from £0 to £100,000.
{kind=link}
{kind=link}
Cost-effectiveness acceptability curve showing the probability that the Let's Prevent intervention is cost-effective for different ceilings of willingness to pay (cluster adjusted). QALY, quality-adjusted life year.
Sensitivity analysis
In all exploratory scenarios for the within-trial analysis, the intervention remained cost-effective at a threshold of £20 000/QALY (table 3). For example, not adjusting for the cluster nature of the trial increased the ICER to £4845/QALY. Performing multiple imputations without using practice code as one of the baseline covariates resulted in an ICER of £7891 with a reduced probability (76%) that the intervention is cost-effective compared with the standard care group. Disregarding data from the economic questionnaire (EQ-5D, non-inpatient costs), the net gain in QALYs (0.039) was similar to the primary analysis using EQ-5D merged data (0.046). The net difference in total costs was also similar (£187), as in both scenarios the bulk of the cost difference between groups is a result of the intervention cost. Using a ‘real-world’ cost of £179 (£174 discounted) to deliver the Let's Prevent intervention, rather than the trial costs (£200, £195 discounted), the net difference in total costs falls from £168 to £147, and the ICER falls to £3188.
Sensitivity analysis (multiple imputation models as reported in primary analysis, unless specified)
Discussion
In this study, we have estimated the cost-effectiveness of the Let's Prevent intervention, a structured lifestyle modification programme within a primary care context, using QALYs as our main outcome measure. We have found that the education programme has a high probability of being cost-effective compared with standard care.
The Let's Prevent intervention resulted in more QALYs (0.046) but was more expensive than standard care. These differences were not statistically significant, but the health economics literature is clear that the decision to estimate incremental cost-effectiveness should not be based on separate and sequential hypothesis tests concerning cost and effect differences, but should instead consider the joint density of cost and effect differences.19 ,20 The results here bear out this recommendation, showing that modest cost and effect differences considered jointly produce a high probability that the intervention will be cost-effective, albeit in the context of a substantial amount of missing data, which we discuss below.
A number of previous cost-effectiveness analyses of interventions to prevent diabetes have been published. A systematic review in 2010 identified eight studies of lifestyle and medication therapy to prevent T2DM among high-risk individuals, concluding that these were typically very cost-effective with a median cost per QALY gained of $1500.21 Most prominently, the Diabetes Prevention Program (DPP) and its Outcomes Study (DPPOS) have demonstrated that either intensive lifestyle intervention or metformin in a US healthcare setting could prevent T2DM in high-risk adults for at least 10 years after randomisation, at modest cost or in some scenarios with cost savings per QALY gained.22 The Let's Prevent study is the first UK RCT in participants with prediabetes of a structured education and lifestyle-based diabetes prevention programme designed to be implemented in the NHS primary care setting. Major strengths of this cost-effectiveness analysis include being integrated with a well-designed randomised study in a multiethnic primary care setting to obtain reliable estimates of the intervention's effectiveness over a good length of follow-up (3 years). We were also able to prospectively measure quality of life and healthcare use. The most relevant studies available for comparison concern structured education and lifestyle interventions in patients with T2DM such as the DESMOND intervention. The DESMOND intervention was also found to be cost-effective8 in its study population of patients with established T2DM, with an ICER of £5387/QALY gained.
Trial-based economic evaluations also have limitations, notably that the ‘real-word’ costs for the Let's Prevent intervention are likely to be lower than the within-trial costs which our base case analysis used. In the real world, there would be economies of scale in terms of both manpower and resources required. For example, the one-off costs incurred (educator training, food models, venue costs for training and training materials) would be spread over a much longer period than the trial, bringing the cost per patient down. Additionally, in the trial, educators were paid to run courses; in the real world, the programme would be a commissioned service and existing members of staff would work in a different way, that is, running group courses rather than meeting patients on a one-to-one basis. Hence, we estimate that the ‘real-world’ cost of delivering intervention would be £179 rather than the £200 observed in the trial, and this would reduce the ICER to £3188/QALY, making the Let's Prevent programme even more cost-effective when implemented in clinical practice. However, we acknowledge that some of these real-world differences—such as group versus individual courses—could reduce effectiveness as well as cost.
Another important limitation of the cost-effectiveness analysis relates to the degree of missing data. This ranged from 20% to 56% of observations in the data categories used for the base case analysis. Missing data existed mainly because the economic questionnaire was only introduced halfway through the study, and partly as a result of attrition in patient responses to questionnaires over time. Where possible, we accounted for missing data using multiple imputation, a validated technique23 in the context of RCTs which is superior to complete case analysis. We had insufficient data to impute the 12-month non-inpatient costs, and instead used 24-month estimates as a ‘best guess’ for 12-month data. Given the similarity in non-inpatient costs, both between intervention and standard care groups, and between time points, the effects of this assumption on the analysis were minimal. Moreover, we excluded hospital inpatient costs from the base case analysis due to the high levels of missing data. When these were imputed and included in a sensitivity analysis, the intervention became more cost-effective, adjusting for clustering.
We also used sensitivity analysis to explore aspects of our base case analysis. In the base case analysis, to reduce the amount of data requiring imputation, we mapped 15D scores into EQ-5D scores using a published regression equation.13 The sensitivity analysis showed that, irrespective of the instrument or composite instrument used to estimate QALYs, the intervention group was consistently associated with a net gain compared with the standard care group, once differences in baseline utility had been accounted for. Using only data from the 15D instrument, the net gain in QALYs in the intervention group was similar to our primary analysis using composite EQ-5D-based data.
Our cost-effectiveness analysis is based on what we believe to be the longest RCT among prediabetes patients in a UK community setting. Additional follow-up might be expected to yield greater quality of life benefits for the intervention group, as the benefits of postponing development of T2DM are not immediately apparent, and this would further improve the cost-effectiveness of the intervention. We originally planned to conduct some extrapolation, based on the assumption that the trial might produce differences in numbers with diagnosed diabetes, the long-term outcomes of which could then be propagated by modelling. In fact, no statistically significant differences were observed in the proportion developing diabetes, or in cardiovascular disease or coronary heart disease 10-year risk; instead, the outcomes were driven by the observed quality of life differences, which would not have been propagated by available extrapolation models. The study design does not permit us to identify reasons for these small differences. However, some qualitative work conducted as part of the study suggests that patients receiving the structured education programme felt they had an increased understanding of the nature and implications of their diagnosis, and better understood key messages about lifestyle changes with regard to diet and physical activity.24 This may have resulted in higher utility levels. Further research is under way to explore whether these small differences in quality of life are concentrated in particular domains of the EQ-5D. Additional follow-up of patients would reveal whether the observed quality of life differences are maintained, and whether any significant differences emerge in risk factors or in development of diabetes. Meanwhile, the results of the Let's Prevent Diabetes intervention appear to have been sufficiently promising for the NHS to adopt a modified version within the framework of the NHS Diabetes Prevention Programme initiated in 2016.
Conclusion
This study provides a reliable estimate of the costs of the Let's Prevent intervention, and broadly based estimates of the outcomes of the intervention in terms of QALYs and healthcare costs. The pragmatic nature of the study suggests that the intervention could be readily implemented in the real-world setting. The results appear robust across a range of assumptions, indicating that the Let's Prevent intervention is cost-effective using quality-adjusted survival as the main outcome measure. Owing to the modest number of cases of T2DM prevented, this study has not attempted to quantify the additional long-term benefits this would provide.
References
Footnotes
Twitter Follow Alastair Gray @HERC_Oxford
Contributors JL wrote the cost-effectiveness analysis plan, analysed the economic data, and drafted and revised the paper. DA cleaned and analysed the economic data, and drafted and revised the paper. MJD was the principal investigator for the Let's Prevent Programme Grant, initiated the project, commented on drafts of the paper and approved the final version. LJG was the statistician for the Let's Prevent Programme Grant, had input into the design of the study and the collection of data, commented on drafts of the paper and approved the final version. KK and TY had input into the design and running of the study, commented on drafts of the paper and approved the final version. AMG designed the cost-effectiveness plan and the collection of economic data, led the cost-effectiveness analysis, contributed to drafts of the paper and approved the final version. AMG is the guarantor for the paper and affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding This research was funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0606-1272). This report/article presents independent research commissioned by the NIHR under its Programme Grants for Applied Research scheme (RP-PG-0606-1272).
Disclaimer The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests An adapted version of the Let's Prevent Diabetes intervention is on the framework for the NHS Diabetes Prevention Programme. This work is led by Ingeus (main contractor), and Leicester Diabetes Centre, University Hospitals of Leicester (sub-contractor) will provide training and quality assurance for which funding will be received. MJD, KK, TY and LJG were involved in the development of this adapted programme. MJD, KK and TY were members (KK chair) of the NICE PH 38 (preventing type 2 diabetes: risk identification and interventions for individuals at high risk) Programme Development Group.
Ethics approval Main Research Ethics Committee, University Hospitals of Leicester Trust R&D Committee, Leicester City PCT and Leicestershire County and Rutland PCT. Trial Registration: ISRCTN80605705.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data requests pertaining to the Lets Prevent trial should be made directly to ctu@le.ac.uk.