Article Text

Abstract
Introduction In-centre nocturnal haemodialysis (INHD) is an underutilised dialysis regimen that can potentially provide patients with better clinical outcomes due to extended treatment times. We have established an INHD programme within our clinical network, fulfilling a previously unmet patient need. This feasibility study aims to gather sufficient data on numerous outcome measures to inform the design of a multicentre randomised controlled trial that will establish the potential benefits of INHD and increase the availability of this service nationally and internationally.
Methods and analysis This will be a non-randomised controlled study. Prevalent patients on haemodialysis (HD) will electively change from a conventional in-centre HD regimen of 4 hours thrice weekly to a regimen of extended treatment times (5–8 hours) delivered in-centre overnight thrice weekly. After recruitment of the INHD cohort, a group of patients matched for age, gender and dialysis vintage will be selected from patients remaining on a conventional daytime dialysis programme. Outcome measures will include left ventricular mass as measured by MRI, physical performance measured by the short physical performance battery and physical activity measured by accelerometry. Additionally we will measure quality of life using validated questionnaires, nutritional status by bioimpedance spectroscopy and food diaries, and blood sampling for markers of cardiovascular disease, systemic inflammation. Suitable statistical tests shall be used to analyse the data. We will use omnibus tests to observe changes over the duration of the intervention and between groups. We will also look for associations between outcome measures that may warrant further investigation. These data will be used to inform the power calculation for future studies.
Ethics and dissemination A favourable opinion was granted by Northampton Research Ethics Committee (15/EM/0268). It is anticipated that results of this study will be presented at national and international meetings, with reports being published in journals during 2017.
Trial registration number ISRCTN16672784.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Inclusion of control group matched for age gender and dialysis vintage.
Many outcome measures that can and will inform future study design.
Use of robust and validated techniques.
No randomisation of treatment allocation.
Relatively small sample sizes and study is now powered.
Introduction
Incidence and prevalence of chronic kidney disease (CKD) has increased significantly over the last decade.1 ,2 It is estimated that between 5% and 8% of the current UK population have some degree of chronic renal impairment.3 ,4 Of these, a small proportion will progress to end-stage renal disease (ESRD) and require some form of renal replacement therapy (RRT). After transplantation, the second most common form of RRT in the UK is haemodialysis (HD)5 and according to the latest UK renal registry data5 there were 24 166 patients on HD in the UK in 2014, an increase of 2% over 2013. This trend of increasing numbers has been consistent over the last decade.
Patients typically receive HD three times per week for four hours per session. This conventional HD (CHD) regimen has a large physiological impact on a patient's cardiovascular system,6–8 and potentially contributes to high rates of cardiovascular disease in this population. This is particularly important as cardiovascular death accounts for 40% of all-cause mortality9 in patients on HD. The symptom burden related to HD is also extremely high,10 with many patients reporting very poor quality of life.11 ,12 These problems combined with the fact that many patients lose large portions of their time travelling to and from dialysis centres mean that many are unable to continue in paid employment.
The increasing number of patients on CHD is putting increased demand on dialysis services, and slots for HD are now at a premium. Home-based HD is one method of providing extended treatments to patients, but currently only 4.7% of patients on HD are on a home HD programme.2 Although home HD may be more flexible and provide opportunity for more patients to receive treatment, there are significant barriers preventing major usage. These include physician-related factors, such as lack of knowledge and expertise; as well as patient-related factors such as fears and anxieties around self-cannulation or distance from medical care, and perceived caregiver burden.13
In-centre nocturnal haemodialysis (INHD) is an alternative method of delivering extended HD to patients that overcomes barriers to home HD for some patients. INHD provides extended periods of HD overnight for prevalent patients on HD in the outpatient setting, and may also help accommodate the increased demand for HD. There are already cross-sectional data that suggest INHD may be associated with improvements in certain clinical outcomes14–19 and may even improve survival.20 Despite these potential clinical benefits, INHD is not routinely offered as a standard therapy choice in the UK.
The aim of this non-randomised controlled feasibility study is to provide data which will inform future trial design to adequately assess the benefits of INHD. Currently, the majority of trials investigating the effects of extended nocturnal HD involve participants on daily treatments at home.21 At the time of publication, evidence for the benefits of INHD mainly suggests improvements in cardiovascular health, specifically with regards to left ventricular hypertrophy (LVH), and blood biochemistry. However, of the papers investigating the effects on LVH, only one has used cardiac MRI (CMR), which is recognised as the gold standard.22 No data currently exist on the impact INHD may have on physical performance or physical activity levels.
The MIDNIGHT study (Maintenance In-centre nocturnal haemoDialysis: a feasibility study iNvestIGating the effects on cardiac structure and pHysical funcTion) is the first stage in a programme of planned studies seeking to understand the extent to which longer HD sessions can improve physical and psychological health, as well as how overnight HD programmes can be implemented into routine practice in the UK. The MIDNIGHT study will investigate the effect of INHD on previously unresearched outcome measures, using gold standard techniques including CMR, accelerometry and bioimpedance spectroscopy (BIS), to observe left ventricular (LV) structure and function, activity levels and body composition, respectively.
Methods and analysis
Interventions to be measured
This study will compare the effects of a 6-month programme of INHD on a number of outcome measures to matched control patients undergoing conventional daytime HD. This is a non-randomised controlled, feasibility study and patients in the intervention group can electively choose to switch to INHD.
The intervention group will undertake extended, INHD starting with a minimum of 5 hours and then building up incrementally, aiming for 7–8 hours three times per week according to their preference. The INHD programme will be delivered by three HD units within the East Midlands Renal Network, with patients arriving for their treatments in the evening and undergoing HD overnight.
The control group will receive CHD, defined as 4-hour HD sessions three times per week provided to patients during the day time.
As this trial is a feasibility study, no single measure has been selected as a primary outcome at this stage. A number of relevant variables have been identified that may be suitable as a primary outcome measure for a future multicentre randomised controlled trial. Collecting these data in our sample will inform the SD by which future sample size can be calculated.
Patient recruitment
The INHD intervention arm of the study will be a convenience sample of patients who have elected to start INHD. All patients electing to start INHD will be screened and all eligible patients will be approached to participate in the study.
In comparison, purposive sampling will be used to recruit patients to the control arm of the study. This is to ensure that the control group is comparable and well matched to the intervention group. The control group will be matched for age, gender, diabetes status and dialysis vintage.
To be eligible for the study patients must be prevalent adults on HD who have the capacity for consent and are able to undergo CMR. Further descriptions of inclusion and exclusion criteria for this study are shown in table 1. Patients will be recruited to the intervention arm from three centres in the Leicester Renal Network providing INHD programmes. Control patients may be recruited from any centre in the Leicester Renal Network.
Inclusion and exclusion criteria for screening patient eligibility prior to recruitment into the MIDNIGHT study
Study timeline
The study timeline is shown in figure 1. Patients in the intervention arm will be approached for consent 1–2 weeks after starting INHD. Initial assessments will include: baseline CMR (to be completed within 4 weeks of the patient beginning INHD); physical performance assessments; body composition analysis; questionnaires exploring quality of life functional capacity, sleep quality, fatigue and symptom burden and blood sample collection. Patients will also be given an accelerometer to wear for 1-week for objective measurement of physical activity.

Flow chart showing when outcome measures will be collected. BCM, Body Composition Monitor; BRU, Biomedical Research Unit; CHD, conventional haemodialysis; CMR, cardiac MRI; INHD, in-centre nocturnal haemodialysis.
Interim assessments will take place after 3 months. This will involve repeating the questionnaires, body composition, physical performance and blood sampling. The interim assessments will be conducted over two visits, with the physical performance assessments completed on a separate day to blood sample collection to ensure that the blood sample is not affected by physical exertion involved in the performance tests.
Six months after baseline CMR all baseline assessments will be repeated at which point the protocol will be complete.
Cardiovascular endpoints
Cardiovascular disease in patients on HD is primarily driven by non-traditional risk factors, including chronic inflammation, chronic uraemia, myocardial stunning, vascular calcification and stiffening and endothelial damage. It has been documented that 75% of patients on HD have LV hypertrophy which is strongly linked to outcome and mortality in patients on HD. Previous studies using echocardiography suggest that INHD may reduce LV mass by as much as 14 g in 6 months, and a recent study using a 1.5 Tesla (1.5 T) CMR showed that INHD led to a reduction of 8 g of LV mass in 1-year.22
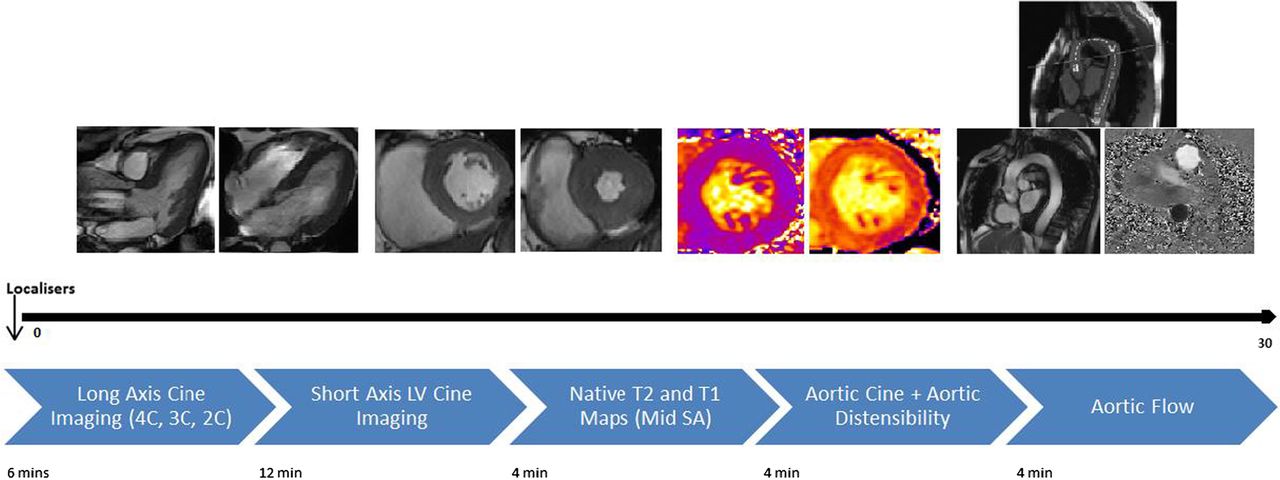
The CMR scan protocol timeline is shown in figure 2. We aim to conduct CMRs on a non-dialysis day within 24 hours of the previous HD session. Cardiac structure and function will be assessed using a 3 T CMR platform (Skyra, Siemens Medical Imaging, Erlangen, Germany). The CMR protocol will be similar to that previously described but without contrast administration.23 LV volumes and mass will be quantified with epicardial and endocardial contours of a contiguous stack of multiphase ventricular short axis cines (10–12 slices, 8 mm slice thickness, 25% gap) at end-diastole and end-systole. Native T1 and T2 mapping at mid-ventricular level will be undertaken for tissue characterisation, with non-contrast T1 mapping offering the opportunity to assess myocardial fibrosis.23 ,24 Tissue tracking will be used to assess systolic strain and diastolic strain.25 Arterial stiffness will be assessed by measuring the distensibility of the ascending and descending thoracic aorta. Changes in the cross-sectional luminal area of aorta in a 5 mm thick slice will be measured and concomitant measurement of blood pressure at the time of sequence acquisition will allow calculation of aortic distensibilty.26 We will also use CMR to measure aortic pulse wave velocity as a further measure of arterial stiffness.

{kind=link}
{kind=link}
Protocol used for CMR procedures and pictures showing the images gained at those points. CMR, cardiac MRI; SA, short axis; LV, left ventricular.
CMR image analysis
All scans will be anonymised and analysed off-line. Both visual and quantitative analysis of CMR images will be undertaken, as per international guidelines.27 Quantitative analysis will be performed by a single operator using Food and Drug Administration (FDA) approved commercially available software. These will include: LV mass (g); end-diastolic volume (mL); end-systolic volume (mL); stroke volume (mL); and ejection fraction (%). All volumetric data will be indexed to body surface area.
Calculation of T1 and T2 values will involve the drawing of epicardial and endocardial borders from a mid-short axis slice of the LV.28 LV strain and strain rate will be assessed as previously described.25 Manual drawing and propagation of endocardial and epicardial contours onto the end-diastolic image, will allow the calculation of LV endocardial and epicardial circumferential and longitudinal strain and strain rates.
Aortic distensibility will be analysed as previously described.29 A region of interest using JIM V.6 (Xinapse software, UK) will be used to manually identify the ascending thoracic aortic area, which will be represented graphically against time. The following, validated formula will be used to determine aortic distensibility:
(maximum aortic area−minimum aortic area)/(minimum aortic area×ΔP).
ΔP is the brachial pulse pressure reading performed during CMR.30
Physical performance
Patients on HD have been shown to have reduced physical performance compared with healthy age-matched controls.31–34 This impacts on the ability to carry out activities of daily living, and it has also been shown that poor physical performance is linked to higher mortality risk.35 ,36 INHD will give patients more free time in the daytime to be physically active and engage in exercise activities, which may improve their physical performance.
We will measure physical performance using the short physical performance battery (SPPB) and the sit-to-stand 60 test (STS60). Both the SPPB and STS60 have been used by many research groups investigating the impact of exercise interventions in patients on HD. The SPPB comprises three simple tests: a balance test, requiring patients to stand in three increasingly difficult positions for 10 s; a gait speed test, where patients are timed walking along a 4 m course; and a STS5, where patients stand up and sit down in a chair as quickly as possible five times, providing a measure of muscle power.37 The STS60 provides a surrogate marker of muscular endurance.
Physical activity
Owing to the scheduling and side effects of CHD, many patients on HD have a very sedentary lifestyle with extremely low activity levels.38–40 INHD will allow patients to be more active during the day.
Physical activity will be objectively measured using SenseWear Activity Monitors, which will be worn by the patients for 1-week. Measurements made by the accelerometer will provide values for average Metabolic Equivalent of Tasks (METs; a measure related to oxygen consumption that quantifies functional capacity)41 for each patient during the time worn, energy expenditure and number of steps.
Nutrition, body composition and blood biochemistry
Current evidence suggests that INHD may improve nutritional aspects of patient's health, and may also increase body weight.15 ,19 ,42 ,43 An increase in bodyweight is a desirable outcome for undernourished patients on HD, if the weight gained is lean tissue.44–46 However, the Frequent Haemodialysis Network (FHN) randomised-controlled trial that looked at nocturnal HD conducted on 5–7 days of the week at home, failed to show an improvement in body composition.47 This may have been due to the difference in their dialysis prescription, but may also be due to their assessment of body composition using single frequency bioimpedance analysis, a less-sensitive technique with disputable validity in patients on HD.
In the MIDNIGHT study, body composition will be analysed by BIS using a Body Composition Monitor (BCM; Fresenius, Bad Homburg, Germany). The BCM has been validated against a number of gold standard measurements for use in patients on HD.48 The calculations used by the BCM permit the accurate assessment of overhydration status in patients, as validated against expert clinical assessment.49 ,50 Outcomes acquired include ‘normally hydrated’ lean tissue mass, ‘normally hydrated’ adipose tissue mass, intracellular fluid, extra cellular fluid, fat mass and body cell mass.
Data relating to clinical blood biochemistry and haematology will also be collected from routine monthly blood tests conducted as part of patient's standard care.
Quality of life
Previous research has shown that INHD may lead to significant improvements in patient's quality of life.51
We will assess changes in quality of life using the Short Form-12 questionnaire (SF-12; Quality Metrics), which has been previously validated for use in the renal disease population.52 ,53
Symptom burden
Longer dialysis is known to improve the clearance of small and middle weight molecules.54–56 The physical and psychological improvements previously documented51 are likely to be associated with a reduction in symptoms experienced by patients; however, previous studies have failed to report this. We will measure symptom burden using the Palliative Outcome Scale—Symptoms Renal (POS-S Renal) questionnaire. This 17-item questionnaire is specifically developed for use on patients with renal disease.57 ,58
We will also assess the levels of fatigue in these patients using the Functional Assessment of Chronic Illness Therapy—Fatigue (FACIT-F).59–61
Sleep quality
Patients on HD often experience disturbed and poor quality sleep.62 ,63 Some data suggest that extended HD can improve sleep quality and reduce symptoms of sleep apnoea.64–66 The Pittsburgh Sleep Quality Index (PSQI) will be used to assess the impact of our INHD programme on patient's sleep quality.67–69
Data analysis plan
Demographic data on patients will be gathered and suitable comparisons (eg, χ2 test) will be made to ensure that the groups are well matched. All outcome measures will undergo appropriate omnibus tests to investigate statistical differences between patients and within patients. In addition to this we will look at associations between outcome measures and investigate potential interactions between variables, to generate hypotheses for future studies.
Ethics and dissemination
Ethical and safety considerations
The MIDNIGHT study protocol was reviewed by the Northampton Research and Ethics Committee (REC). This committee appraised the ethical implications of procedures that would be carried out during the study and the potential impact on patient rights and well-being. Favourable opinion from the REC means that due care and consideration has been made to preserve patient rights and the methodology is ethically justified; favourable opinion was provided on the 9 July 2015 (REC reference: 15/EM/0268). Further to this, local research and innovation approval was provided by University Hospitals of Leicester on 13 July 2015 (UHL11434).
Informed consent will be obtained from participants in line with recommendations set out in E6(R1) of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Good Clinical Practice guidelines.
Dissemination plan
We plan to present all data at national and international conferences. Furthermore, we will also publish the findings in international journals. We expect to publish our initial findings during late 2016/early 2017. Following the publication of our results participant level data will be available for collaborations, on request.
Trial registration
The MIDNIGHT study is registered with the ISRCTN (ISRCTN16672784). The registration process was initiated before the recruitment began; however, time constraints at one centre led to our first patient being recruited prior to payment clearing and completing our registration status. It is for this reason our registration status is listed as retrospective.
References
Footnotes
Twitter Follow Darren Churchward at @Darren_Churchy
Contributors DRC contributed to the drafting, review and final preparation of the manuscript. MPMG-B contributed to the drafting and review of the manuscript. GPM, RP and WP contributed to the conceptual design of the study and review of the manuscript. JOB contributed to the conceptual design of the study, review of the manuscript and gave final approval.
Funding This study was funded through a grant from the van Geest Heart and Cardiovascular Health Research Fund.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the National Health Service, the sponsor or the funders.
Competing interests None declared.
Ethics approval NREC East Midlands—Northampton.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Anonymised participant level data will be made available to interested collaborators on request, following publication of final results manuscript.