Article Text

Abstract
Objectives Disability is considered an important issue that affects the elderly population. This study aimed to explore the relationship between disability and all-cause mortality in US elderly individuals.
Design Retrospective and longitudinal designs.
Setting Data from the National Health and Nutrition Examination Survey (NHANES 1999–2002) conducted by the National Center for Health Statistics of the Centers for Disease Control and Prevention.
Participants A total of 1834 participants in the age range 60–84 years from NHANES 1999–2002.
Main outcome measures We acquired five major domains of disability (activities of daily living (ADL), general physical activities (GPA), instrumental ADL (IADL), lower extremity mobility (LEM) and leisure and social activities (LSA)) through self-reporting. We applied an extended-model approach with Cox (proportional hazards) regression analysis to investigate the relationship between different features of disability and all-cause mortality risk in the study population.
Results During a mean follow-up of 5.7 years, 77 deaths occurred. An increased risk of all-cause mortality was identified in elderly individuals with disability after adjustment for potential confounders (HR 2.23; 95% CI 1.29 to 3.85; p=0.004). Participants with more than one domain of disability were associated with a higher risk of mortality (ptrend=0.047). Adjusted HRs and 95% CIs for each domain of disability were 2.53 (1.49 to 4.31), 1.99 (0.93 to 4.29), 1.74 (0.72 to 4.16), 1.57 (0.76 to 3.27) and 1.52 (0.93 to 2.48) for LEM, LSA, ADL, IADL and GPA, respectively.
Conclusions The results of this study support an increased association between disability and all-cause mortality in the elderly in the USA. Disability in LEM may be a good predictor of high risk of all-cause mortality in elderly subjects.
- elderly
- mortality
- disability
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study used a nationwide population-based dataset.
The study explored the impact of disability on all-cause mortality in elderly individuals in the USA.
Self-reported disabilities may not reflect objective surveys of functional representation.
Introduction
Disability, which has been defined as the consequence of activity limitations, participation restrictions and impairments, is generally regarded as an important and serious issue in elderly individuals which affects quality of life and lifestyle.1 Many patients aged 65 years and older have a disability or functional decline, leading to hospitalisation and acute medical illness. The increasing numbers of elderly individuals with disability in the coming decades is causing major public health apprehension about the latent economic and social burden. Disability is attributed to the negative manifestations of an interaction between an elderly individual and the environment,1 as well as increasing utilisation and healthcare costs,2 premature death3–5 and diminished quality of daily life.6
Disability in elderly individuals is identified on the basis of their difficulty in participating in daily activities or those activities necessary for independent living and integration into their environment.1 Several domains in functional disability, such as activities of daily living (ADL)7 and instrumental ADL (IADL), have been developed for the screening and prediction of early functional decline in elderly individuals.8 ,9 Disability in ADL and IADL have generally been accepted as poor prognostic factors in the elderly.4–10 Some relevant studies have demonstrated an association between disability and functional decline, chronic multimorbidity and mortality in elderly subjects.11 ,12 Prior studies have also reported that disabilities in lower extremity mobility (LEM), leisure and social activities (LSA) and general physical activities (GPA) are linked to increased risk of cognitive decline, late life disability and poor survival outcomes.13–16
However, the roles of disability severity and different patterns of functional decline as well as the association between various functional domains and all-cause mortality remain unknown and have not been examined in the US elderly population. Therefore, we investigated the relationship between the presence and severity of disability—including the number and different types of functional domain—and all-cause mortality using data from the 1999 to 2002 National Health and Nutrition Examination Survey (NHANES).
Methods
Study design and participants
NHANES, conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention, is a survey for the measurement of health and nutritional status in the USA. Initiated in the early 1960s, NHANES has been accomplished as a series of unique surveys providing abundant information on various health topics. It comprises detailed home interviews, including demographic, socioeconomic, dietary and health-related questions, and examinations executed by trained medical personnel at a mobile examination centre. Detailed consent documents and survey operation manuals for the 1999 to 2002 NHANES are available from the NHANES website.17 ,18 Detailed all-cause mortality information and follow-up data from the time of study participation were obtained using the NHANES Linked Mortality File, which was provided by the NCHS according to the probabilistic matching between NHANES 1999–2002 participants and National Death Index death certificate records. The follow-up data in the present study were calculated from the date of examination until date of death or censoring on 31 December 2006 (whichever came first).
Participants were only enrolled if they were aged 60–84 years in order to prevent possible age misclassification.19 Demographic information was collected through a structured home interview and accompanied by a series of physical examinations and blood sampling at a mobile examination centre. Among the elderly population, eligible subjects with incomplete data for the disability questionnaire screening, or without relevant laboratory and/or clinical examinations, were also excluded. The 1999 to 2000 and 2001 to 2002 NHANES studies were executed in accordance with the Declaration of Helsinki and approved by the NCHS institutional review board. Informed, written consent was obtained from all participants before the start of the study.
Self-reported disability
This study focused on five major domains of functional disability: ADL, IADL, GPA, LSA and LEM. Participants were interviewed and asked 19 specific questions for measurement of self-reporting functional status. The questionnaire was designed to assess the subject's level of difficulty in fulfilling a task without using equipment, and the 19 specific questions were classified into the following five major functional domains: GPA (standing up from an armless chair, grasping small objects), LEM (walking up 10 steps), LSA (performing leisure activities at home), ADL (dressing, eating, walking and getting out of bed), IADL (doing household chores, preparing meals and managing money).19 This variable was assessed as the sum of the five major functional domains at baseline and analysed as a continuous variable, with a range of 0 to 19. Each disability was defined as difficulty in performing one or more activities within the specified domain and analysed as a continuous variable, with a range of 0–4, 0–7, 0–3, 0–2 and 0–3 for ADL, GPA, IADL, LEM and LSA, respectively. The presence of a disability was defined as any functional disability within the five major domains. Numbers of disabilities were assessed as the sum of the number of domains in which a subject was disabled at baseline and analysed as a continuous variable, with a range of 0 to 5. Severity of disability was determined by summing the number of domains in which a subject was disabled.
Covariates
Participants were interviewed to collect information on age, gender, race/ethnicity, body measurements, blood pressure (BP), pre-existing medical conditions and smoking status. After a NHANES-associated physician had collected three or four BP measurements using a mercury sphygmomanometer, average systolic and diastolic BP values were obtained. Hypertension was defined as the use of antihypertensive medications, an average BP ≥140/90 mm Hg, or by self-reporting of a physician's diagnosis. Diabetes mellitus was defined as the use of diabetic medications (including insulin injection and/or oral hypoglycaemic agents), a random plasma glucose level of ≥200 mg/dL, or by self-reporting of a physician's diagnosis. Other chronic medical conditions—for example, stroke and heart disease (defined as a history of myocardial infarction, coronary artery disease (CAD), congestive heart failure, or angina)—were ascertained using self-reporting questionnaires. Cognitive impairment was determined from the result of the Digit Symbol Substitution Test (DSST), a subtest of the Wechsler Adult Intelligence Scale. Information on the quality control procedures used in this study has been published elsewhere.20 Details of the processing instructions and collection of specimens are discussed in the NHANES Laboratory Procedures Manual, which is available on the NHANES website.18 ,19
Statistical methodology
All statistical analyses were performed using SPSS for Windows V.18.0 with the Complex Samples Procedure applied to incorporate sample weights and adjust for clusters and strata within the Complex Sample design. Quantitative variables were expressed as means and SDs, while qualitative data were presented as numbers and percentages. Demographic characteristics were compared using the χ2 test for discrete variables, and an independent t test or Wilcoxon rank-sum test was used for continuous variables. A two-sided probability (p) value of <0.05 was considered significant. Survival analysis applying a Cox (proportional hazards) regression model was used to calculate HRs with 95% CIs for a comparison of participants' functional status, including presence of disability, number of disabilities or each individual domain of disability, using multivariate linear regression. An extended-model approach was used for the adjustment of covariates: model 1, not adjusted for other variables; model 2, adjusted for age, gender, race and marital status; model 3, model 2 plus serum C-reactive protein (CRP), glucose, low-density lipoprotein (LDL) and total bilirubin levels; model 4, model 3 plus hypertension, diabetes mellitus, strokes and heart disease, including CAD; model 5, model 4 plus serum albumin, cognitive impairment, number of prescription medications taken. p Values for trend tests (ptrend) were assessed by treating the number of domains in which a subject was disabled as a continuous variable with a range of 0–5, to observe the association between the presence of an increasing number of disabilities and all-cause mortality risk in elderly individuals. Kaplan-Meier survival plots represented the associations between five major domains of functional disability and the risk of all-cause mortality in US elderly patients.
Results
Characteristics of the study sample
A total of 21 004 participants attended the mobile examination centre between 1999 and 2002. Following the collection of two NHANES datasets (1999–2000 and 2001–2002), participants aged below 60 (N=17 298) or above 85 years (N=409) were excluded from the study. A total of 3297 participants were aged between 60 and 84 years. After participants with incomplete data for the disability questionnaire screening (N=308), or without relevant laboratory and/or clinical examinations (N=853), or not included in the mortality follow-up and/or loss to follow-up (N=302) were excluded, 1834 participants were included in the analyses. Selected baseline characteristics of the study sample shown as a disability group (N=482, mean±SD age 71.94±7.17 years) and a non-disability group (N=1352, mean±SD age 69.79±6.92 years) are summarised in table 1. Compared with the non-disability group, participants with a disability tended to be older and had significantly higher serum CRP, glucose and lower serum total bilirubin and albumin levels (all p<0.05). Furthermore, participants with a disability were also found to be associated with a significantly higher prevalence of diabetes mellitus, stroke, heart disease including CAD, and cognitive impairment and a higher number of prescription medications taken (all p<0.05).
Participant characteristics of disability and non-disability
Disability and risk of mortality
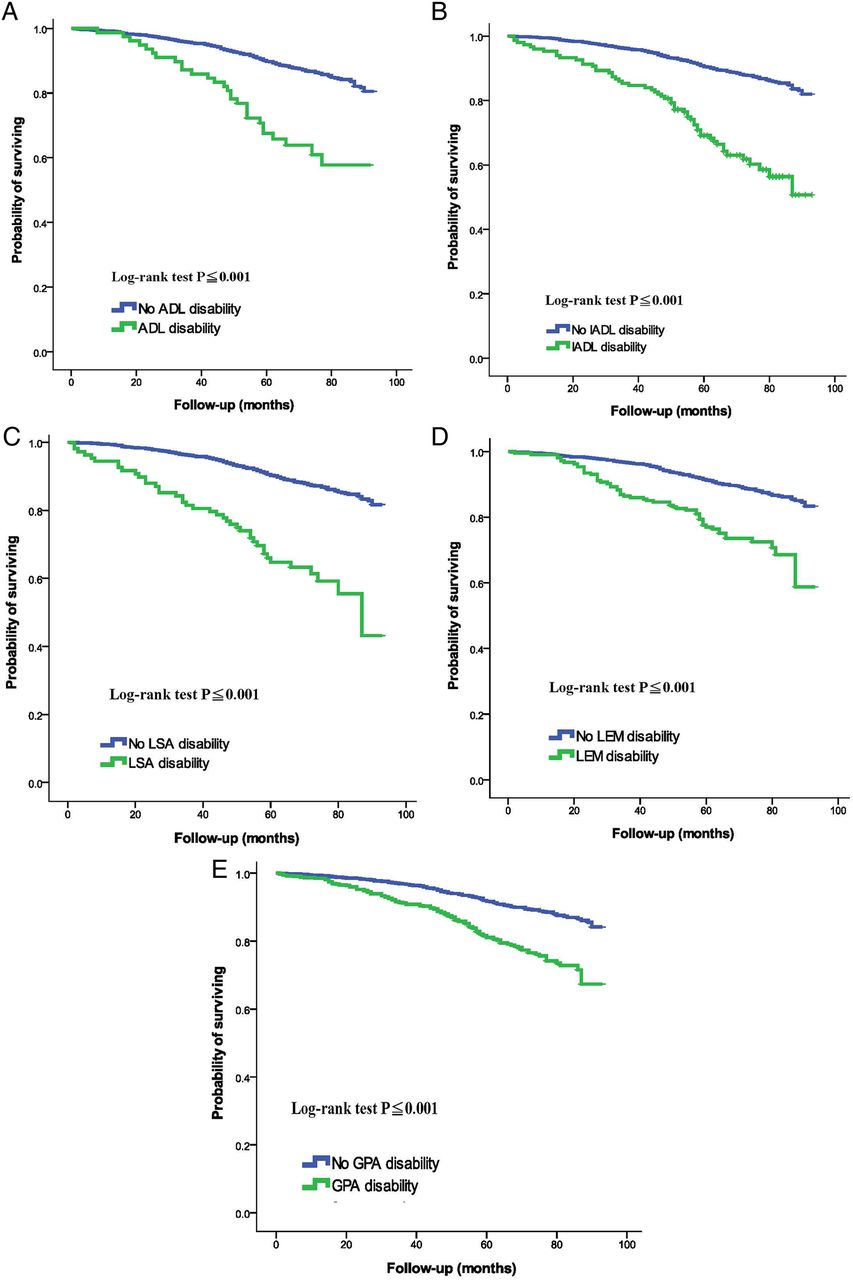
During a mean follow-up of 5.7 years, 77 deaths occurred. The results from models examining an association between disability and the risk of mortality in elderly patients are presented in table 2 and figure 1. As demonstrated in table 2, a strong linear increase in HRs was detected as the number of disabilities increased (ptrend<0.05). Following additional adjustments, the HRs and 95% CIs for individuals with domains of LEM, LSA, ADL, IADL and GPA disability were 2.53 (1.49 to 4.31), 1.99 (0.93 to 4.29), 1.74 (0.72 to 4.16), 1.57 (0.76 to 3.27) and 1.52 (0.93 to 2.48), respectively. There was a significant interaction between disability and gender (p<0.001). Based on the significant findings of the interaction testing, gender-stratified analyses were performed. The associations between disability and risk of mortality in elderly men and women are presented in tables 3 and 4. These findings revealed that the strength of the association between disability and mortality was stronger for women than men. As shown in figure 1, we analysed the participants' prospect of survival in each of five functional status categories. We have presented the prospect of survival in each of five functional status categories for elderly men in online supplementary figure 1 and for elderly women in online supplementary figure 2, since the interaction term was significant. In the fully adjusted models, the probability of survival declined significantly with disabilities in ADL, GPA, IADL, LEM and LSA (all p<0.001).
Regression coefficients of the presence and number of disabilities for the risk of mortality in elderly individuals
Regression coefficients of the presence and number of disabilities for the risk of mortality in elderly men
Regression coefficients of the presence and number of disabilities for the risk of mortality in elderly women
{kind=link}
Kaplan–Meier plots of associations between five major domains of functional disability (activities of daily living (ADL), general physical activities (GPA), instrumental ADL (IADL), lower extremity mobility (LEM) and leisure and social activities (LSA)) and the risk of all-cause mortality in elderly individuals in the USA.
Supplementary figures
Discussion
In this study, we investigated a nationally represented sample of older adults in the US population to determine whether there is an association between disability and all-cause mortality risk among elderly individuals. We found the presence of disability in five major functional domains (ADL, GPA, IADL, LEM and LSA) to be associated with an increase in all-cause mortality risk in elderly individuals aged 60–84 years, independently of basic demographics, health behaviours, chronic medical illnesses and nutritional markers. Elderly individuals with more domains of disability had a higher risk of all-cause mortality. Of all of these functional domains, LEM disability was associated with the poorest prognoses. There is general agreement among geriatricians and gerontologists that disability results from underlying pathophysiological and/or biological alterations that are age-related and may be aggravated by single/multiple diseases or end-stage outcomes of severe diseases.21 Functional assessment of disability and predicting disability risk are cornerstones of geriatric medicine. However, few studies have examined the association between disability and all-cause mortality risk in the elderly population.22–24 The present study is the first survey-based analysis to produce evidence of an association between LEM disability and all-cause mortality risk.
Disability status has been demonstrated to be a strong indicator in predicting adverse outcomes,7–9 probably because measurements of disability are able to disclose the influence of the presence and severity of multiple pathologies on an individual's overall health. Millán-Calenti et al10 used several indicators of functional impairment, including ADLr and IADL, to examine the relationship between disability and all-cause mortality risk in an elderly population. They reported that advanced age and female gender are important factors associated with disability in ADL and IADL, which correlated with mortality risk in elderly subjects.10 A recent study conducted by Avelino-Silva et al25 further demonstrated that ADL and IADL dependency were not only associated with in-hospital deaths of older patients, but also with other adverse outcomes (eg, delirium, nosocomial infection and longer hospitalisation). Our study differed from prior studies in providing additional, thorough data linking disabilities to all-cause mortality risk in elderly individuals, using a geographically dispersed national US sample. Functional status was assessed, not only by ADL and IADL, but also by other clinically relevant disability domains, including GPA, LEM and LSA. Our study revealed that disability in LEM correlated significantly with all-cause mortality risk in elderly individuals.
Plausible explanations for this increased association between disability and all-cause mortality risk in elderly individuals are multifactorial, including loss of muscle strength/mass, low gait speed, and cognitive impairment. First, an age-associated decline in muscle strength/mass, an important predictor of physical function, disability and mortality,26 is profoundly modulated by a number of physiological factors, including inflammation, hormone regulation, neurological integrity, nutritional status and physical activity, among others. A study conducted by Rantanen et al27 revealed that poorer muscle strength was associated with more difficulty in performing physical ADL. Moreover, decreased physical activity predicted a decline in muscle strength and an increased risk of losing muscle mass.28 ,29 The presence of an underlying medical illness (eg, diabetes mellitus, stroke or heart disease, including CAD) was also associated with decreased muscle strength.30 Proposed pathways of illness-related muscle impairment include physical inactivity, nutritional depletion and systemic inflammation, which are risk factors associated with increased rates of mortality among the elderly.31–34 Second, decreased gait speed has been found to play an important role in the association between disability and all-cause mortality risk. A slow gait speed may be recognised as a screening measure that reflects deconditioning and decreased physical and social activity in the elderly. In the general population, an age-related reduction in lower extremity strength was associated with a slower gait speed.35 In a prospective population-based study of 934 individuals aged 65 years or older living in Italy,36 walking speed was confirmed as a strong predictor of adverse health-related events and a significant risk factor for mortality in community-dwelling older adults. Studenski et al13 demonstrated gait speed to be increasingly associated with survival among elderly individuals from a pooled analysis of nine cohort studies, including 34 485 participants aged 65 years or older. Third, disabilities in several domains, such as GPA, IADL, LEM and LSA, may be related to low cognitive function, which is also associated with all-cause mortality risk in elderly individuals. In a longitudinal follow-up study of 5908 participants aged 60 years and over, poorer cognitive performances correlated inversely with a higher risk of mortality.14
We have also examined the potential effect of sex on the relationship between disability and mortality. The plausible explanations for the presence of interactions are biological differences in gender,37 including hormonal effects, immune system responses and genetic factors, gender paradox in mortality and morbidity,38 and gender differences in disability-related health conditions.39 Previous studies have demonstrated that women live longer, report more limitations in function, and survive longer with greater disability late in life.37–40 In this study, we explored evidence that supports the relationship between disability and all-cause mortality in elderly individuals, especially in women. These findings expand on our existing knowledge and highlight the importance of using multiple disability assessment tools as potential clinical predictors of elderly individuals at risk of all-cause mortality. Functional assessments made with the aid of well-validated instruments should be a fundamental part of the health evaluation of elderly individuals. Early detection of different domains of disability may be beneficial for learning to recognise which elderly individuals are most in need of intervention to reduce their risk of mortality.
This study has several potential limitations. First, it was an observational, retrospective and longitudinal analysis of an existing database at a single time point, rather than an analysis of long-term repeated observations with limited causal inferences; evaluating such causal relationships would require longitudinal studies. Next, the disability status of individuals was self-reported, which may on occasion have led to over-reporting of the participants, and may be affected by recall bias or misclassification. In addition, in the NHANES sample, not all selected participants were interviewed and not all interviewed participants were examined. Non-response bias resulting from these missing data may be an important source of error in the survey. Finally, self-reported disabilities may not reflect objective surveys of functional representation. However, previous studies have demonstrated a high degree of correlation between self-reported disabilities and objective physical measures.15 ,16 ,41 The results also suggest a high degree of concordance between self-reported disability data and direct observations of ADL performance.37 In addition, it is not possible to identify subjects who transition in and out of a state of disability. It is also not possible to examine short-term versus long-term disability. Some subjects may have been disabled at the time of the interview and subsequently recovered later on. The opposite may also be true (ie, not disabled at the time of interview and developed disability soon after). Finally, despite adjustments having been made for a large number of potentially confounding factors, residual confounding effects due to unmeasured confounders of the association between disability and risk of all-cause mortality in elderly individuals cannot be ruled out.
In conclusion, the present study has revealed a strong linear increase in disability to be associated with all-cause mortality risk in a representative sample of the US elderly population. Preventing disability would be clinically advantageous in promoting normal ageing and reducing the risk of mortality in this population. Additional studies are warranted to elucidate further the mechanism(s) of this association.
References
Footnotes
Contributors L-WW contributed to the design of the study, was responsible for the management and retrieval of data, contributed to initial data analysis and interpretation, and drafted the initial manuscript. L-WW, W-LC, T-CP, S-TC, H-FY, Y-SS, JY-HC and T-WK decided on the data collection methods. L-WW and W-LC were also responsible for the data analysis decisions. T-WK conceptualised and designed the study, supervised all aspects of the study, critically reviewed and revised the manuscript, and approved the final manuscript as submitted. All authors meet the ICMJE criteria for authorship.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All authors declared willingness for data management and sharing.