Article Text

Abstract
Introduction Gyejibongneyong-hwan (GBH), also known as Guizhi Fuling formula, and is widely used for uterine fibroids in East Asian countries. Many clinical trials assessing the efficacy and safety of GBH formula for the treatment of dysmenorrhoea have been reported. This review will assess the clinical evidence for and against the use of GBH formula as a treatment for dysmenorrhoea. It will also discuss the proposed mechanism(s) that could link herbal medicine to improvements in dysmenorrhoea.
Methods and analysis Fourteen databases will be searched until September 2016. We will include randomised controlled trials (RCTs) examining GBH decoctions for any type of dysmenorrhoea. All RCTs of decoctions or modified decoctions will be included. The methodological qualities of the RCTs will be assessed using the Cochrane Collaboration tool for assessing risk of bias.
Ethics and dissemination This systematic review will be published in a peer-reviewed journal. The review will also be disseminated electronically and in print. It will be updated to inform and guide healthcare practices.
Trial registration number CRD42015023419.
- dysmenorrhoea
- Guizhi Fuling formula
- Gyejibongneyong-hwan
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The strength of this systematic review is unbiased search of various databases without any language restriction.
The trial screening and data extraction will be conducted independently by two authors.
We will use the GRADE approach to assess confidence in estimates of effect.
In the field of complementary and alternative medicine, there are insufficient randomised controlled trials.
Introduction
Dysmenorrhoea can be primary or secondary and is among the most painful menstrual problems of women of reproductive age.1 This study focuses on primary dysmenorrhoea (PD), which is defined as painful menses in women without any uterine abnormalities.2
The prevalence of PD varies from 20% to 90% depending on the pain measurements employed and ethnicities examined.3 PD interferes with women's daily living and schoolgirls' activities. In Korea, 78.3% of adolescent girls have been reported to have PD during their menstrual periods, and this is the main cause of short-term school absences.4 The main symptoms of PD are abdominal and lower back pain before and during menstruation. Fifteen per cent of girls require analgesics to relieve these symptoms.5
Current thinking on the aetiology of PD is that the hormone prostaglandin triggers uterine muscle contractions which result in cramping and pain.6 ,7 In Korean medicine, PD is thought to be caused by the stagnation of the blood or Qi in the lower abdomen during menstruation.8 Non-steroidal anti-inflammatory drugs are considered the first-line treatment for PD.9 Other treatments, such as oral contraceptives and β-blockers, are also prescribed.10 However, these are ineffective and can even elicit adverse events, such as digestive disorders, which have occurred in up to 25% of women.11 Thus, a large number of patients with PD seek complementary and alternative approaches, such as acupuncture,12 moxibustion13 ,14 and herbal medicine.15 ,16
In this review, we will investigate evidence related to the effectiveness of Gyejibongneyong-hwan (GBH) formula, which is widely used in traditional Korean medicine (TKM) and traditional Chinese medicine (TCM) for treating the symptoms of PD.
Methods
Study registration
The protocol for this systematic review has been registered on PROSPERO 2015 under the number CRD42015023419.
Data sources
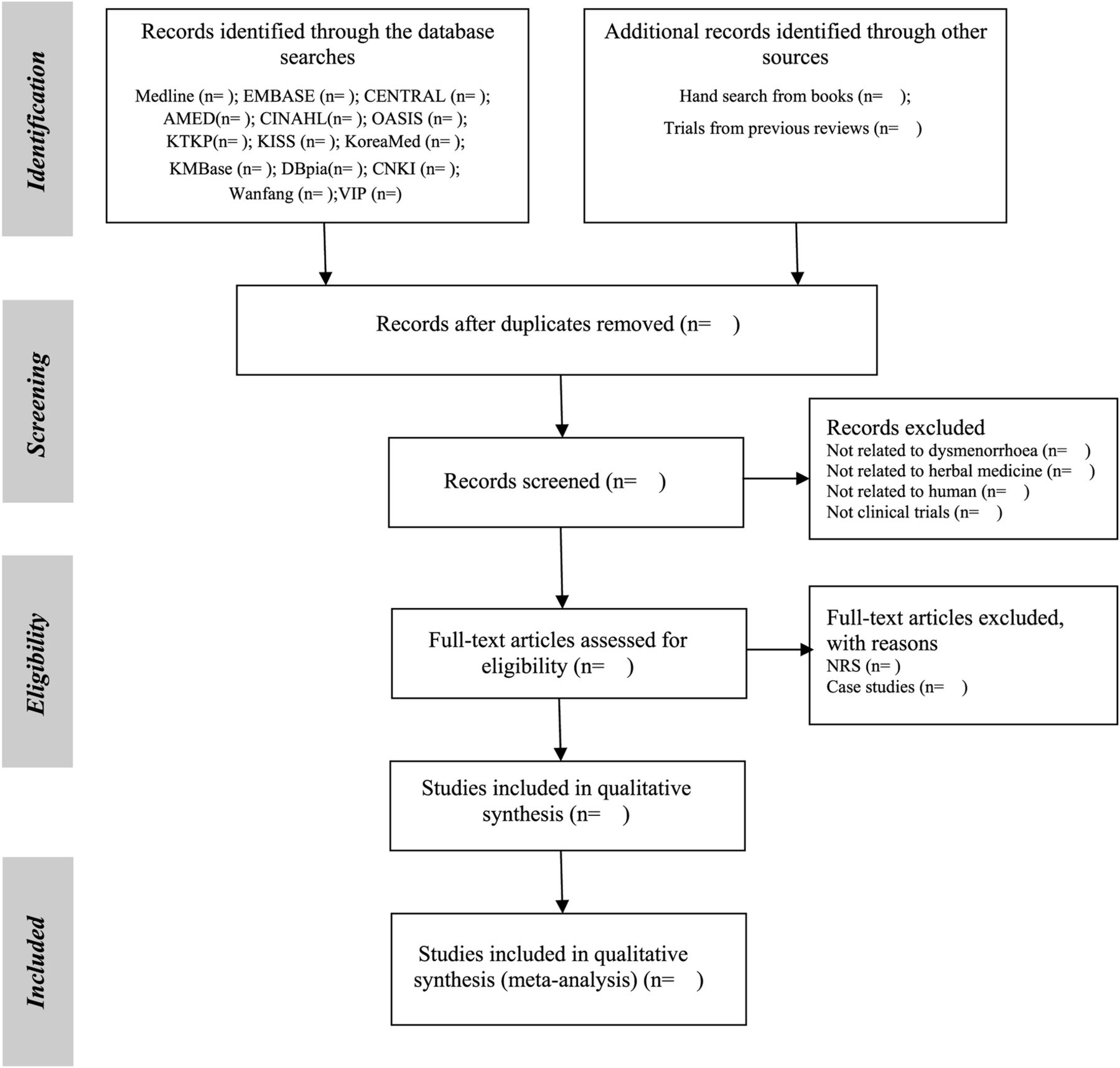
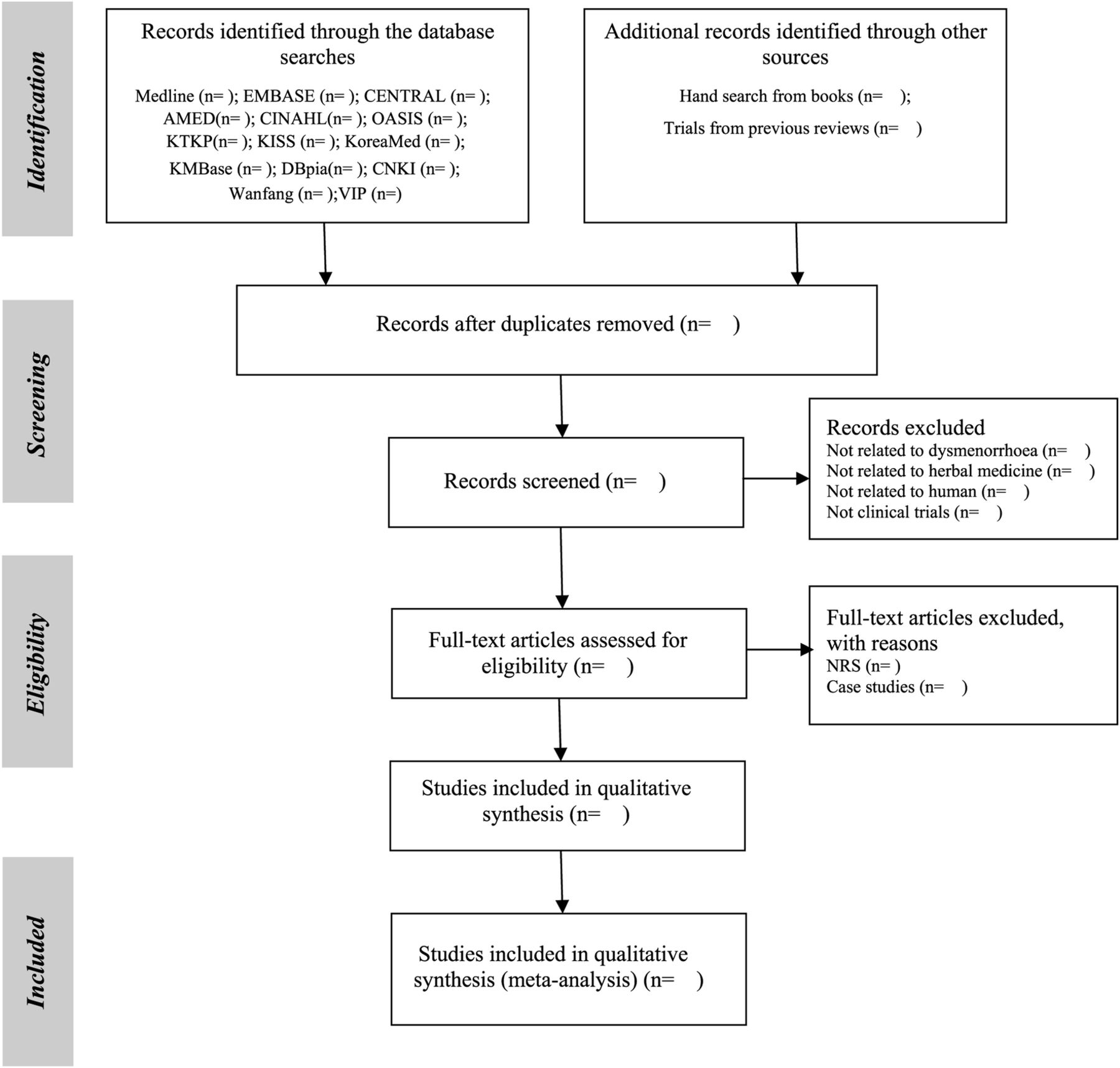
The following databases will be searched from inception to the current date: Medline, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), AMED and CINAHL. We will also search six Korean medical databases (OASIS, Korean Traditional Knowledge Portal (KTKP), Korean Studies Information Service System (KISS), KoreaMed, Korean Medical Database (KMBase) and DBpia) and three Chinese databases including CNKI (ie, China Academic Journal, China Doctoral Dissertations and Master's Theses Full-text Database, China Proceedings of Conference Full Text Database and Century Journal Project), Wanfang and VIP. Furthermore, we will conduct non-electronic searches of conference proceedings, our own article files, and nine Korean traditional medical journals (Journal of Korean Medicine, Journal of the Korean Acupuncture and Moxibustion Society, Korean Journal of Acupuncture, Journal of Acupuncture and Meridian Studies, Journal of Pharmacopuncture, Journal of Oriental Rehabilitation Medicine, Journal of Korea Chuna Manual Medicine for Spine and Nerves, Korean Journal of Oriental Physiology and Pathology and Journal of Korean Oriental Internal Medicine). The search strategies that will be applied to the Medline database and CNKI are presented in online supplements 1 and 2. Similar search strategies will be applied to the other databases.
Supplemental material
Study selection will be documented and summarised in a PRISMA-compliant flow chart (http://www.prisma-statement.org) (figure 1).
{kind=link}
PRISMA diagram for the included studies. NRS, non-randomised studies.
Types of study
All prospective randomised controlled trials (RCTs) will be included if they are randomised studies of GBH formula as the sole treatment or as an adjunct to other treatments, as well as if the control group received the same treatment as the intervention group. Trials comparing GBH formula with any type of control intervention will also be included. No language restrictions will be imposed. Hard copies of all articles will be obtained and read in full.
Data extraction and quality assessment
Hard copies of all articles will be obtained and read in full. Two authors (SJP and JAL) will perform the data extraction and quality assessment using a predefined data extraction form (see online supplements 3–5). Any disagreement among the authors will be resolved by discussion between all of the authors. When the data are insufficient or ambiguous, MSL will contact the corresponding authors by e-mail or telephone to request additional information or clarification. The data screening and selection process will be performed independently by an author who is fluent in Chinese (JHJ). The risk of bias will be assessed using the assessment tool for the risk of bias from the Cochrane Handbook V.5.1.0, which includes random sequence generation, allocation concealment, blinding of the participants and personnel, blinding of the outcome assessments, incomplete outcome data, selective reporting and other sources of bias.17 Our review will use ‘L’, ‘U’ and ‘H’ to indicate the results of the assessments: ‘L’ indicates a low risk of bias, ‘U’ indicates that the risk of bias was unclear, and ‘H’ indicates a high risk of bias. Disagreements will be resolved by discussion between all of the authors. When disagreements regarding selection cannot be resolved through discussion, the arbiter (MSL) will make the final decision.
Data collection and synthesis
Outcome measures
Primary outcomes
Change in symptoms as indicated on a 100 mm visual analogue scale
Pain duration (hours) according to the McGill questionnaire
Improved effectiveness including total treatment efficacy—that is, the number of patients whose PD symptoms improve
Secondary outcomes
Quality of life as measured using a validated questionnaire
Impact of symptoms as measured with validated questionnaires
Adverse events
Information related to GBH usage
Pattern type in response based on TKM or TCM theory
Range of dosage of GBH in each study
Duration of treatment
Details of formula compositions
Assessment of bias in the included studies
We will independently assess the bias of the included studies according to the criteria of the Cochrane Handbook, V.5.1.0: random sequence generation, allocation concealment, the blinding of participants and personnel, the blinding of outcome assessments, incomplete outcome data, selective reporting and other sources of bias.17
Data synthesis
The differences between the intervention and control groups will be assessed. For continuous data, we will use the mean differences (MDs) with 95% CIs to measure the treatment effects. We will convert other forms of data into MDs. In the case of outcome variables with different scales, we will use the standard mean difference (SMD) with 95% CIs. For dichotomous data, we will present the treatment effects as relative risks (RRs) with 95% CIs. We will convert other binary data into RR values.
We will use the GRADEpro software of Cochrane Systematic Reviews to create a Summary of Findings table. When disagreements regarding the selections cannot be resolved through discussion, the arbiter (MSL) will make the final decision.
All of the statistical analyses will be conducted using the Cochrane Collaboration's software programme Review Manager (RevMan) V.5.3.5 for Windows. For studies with insufficient information, we will contact the corresponding authors to acquire and verify the data whenever possible. When appropriate, we will pool the data across studies for a meta-analysis using fixed or random effects.
Unit of analysis issues
For crossover trials, the data from the first treatment period will be used. For trials in which more than one control group is assessed, the primary analysis will combine the data from each control group. Subgroup analyses of the control groups will be performed. Each patient will be counted only once in the analyses.
Addressing missing data
Intention-to-treat analyses that include all of the randomised patients will be performed. For patients with missing outcome data, carry-forward of the last observed response procedure will be used. The individual patient data will be sought from the original source or the published trial reports when the individual patient data are initially unavailable.
Assessment of heterogeneity
We will use the random- or fixed-effects model for the meta-analysis according to the data analysis. I2 tests will be used to evaluate the heterogeneity of the included studies, and I2 >50 will be considered indicative of high heterogeneity. When heterogeneity is observed, we will conduct subgroup analyses to explore the possible causes.18
Assessment of reporting biases
If a sufficient number of the included studies (at least 10 trials) are available, we will use funnel plots to detect reporting biases.19 However, funnel plot asymmetries are not identical with publication biases; therefore, we will attempt to determine the possible reasons for any asymmetries, such as small-study effects, poor methodological qualities, and true heterogeneities in the included studies.19 ,20
Discussion
Among the alternative approaches, GBH, also known as Guizhi-Fuling-Wan (pill), is a widely used remedy for PD and has been employed since ancient times in East Asia.13 ,21 ,22 GBH was first prescribed in the Essential prescriptions from the golden cabinet (Jin Gui Yao Lue) by Zhang Zhongjing of the Han Dynasty (206bc–220ad).23 The five ingredients of GBH are ramulus cinnamomi cassiae, sclerotium poriae cocos, cortex moutan radicis, semen pruni persicae and radix paeoniae lactiflorae, and these ingredients are combined in a ratio of 1:1:1:1:1. GBH is applied to remove blood stasis and masses in the abdominal region to promote blood circulation.15 ,24 There are various forms of GBH such as pills, capsules, tablets and decoctions. All types of GBH will be included in this study. Currently, no systematic reviews of the effects of GBH formula on PD have been published. This systematic review will provide a summary of the current evidence related to the effectiveness of GBH formula in the treatment of the symptoms of PD. In particular, we will consider special features of interventions in full reviews of GBH for PD. Although many systematic reviews have been conducted for herbal medicine, important information on its usage was not extracted and has been missed.25 Therefore, we will identify subtypes that this remedy is particularly useful for (eg, certain pattern types based on TKM or TCM theory), identifying a range of dosages, modifications used to improve effectiveness, or comparing duration of treatment in full review of this protocol. The original GBH formula was composed of the five herbs mentioned above; however, primary studies show high heterogeneity in ingredients of GBH. Therefore, we will investigate the composition of each formula used in the primary studies. This evidence will be useful to practitioners, patients and health policy makers regarding the use of acupuncture in PD treatment.
References
Footnotes
Contributors JAL and SJP conceived the study, developed the criteria, searched the literature, performed the data analysis, and wrote the protocol. JAL, JJ and JC conducted the preliminary search. JJH and MSL assisted in searching the Chinese literature and extracting the data. All authors have read and approved the final manuscript.
Funding JAL, JJ, JHJ and JC were supported by a grant from the Korea Institute of Oriental Medicine (K16111). MSL was supported by Korea Institute of Oriental Medicine (K162921).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We will share any data needed. However, there are no additional unpublished data from this study.