Article Text

Abstract
Objectives The need for denture treatment in public health will increase as the population ages. However, the impact of dentures on nutrition, particularly overdenture treatment, remains unclear although the physical and psychological effects are known. We investigated whether treatment with a mandibular implant supported overdenture improves nutrient intake and markers of nutritional status better than a conventional complete denture in edentulous patients.
Design Systematic review and meta-analysis.
Methods Medline, EMBASE and the Cochrane Central Register of Controlled Trials were searched for eligible studies published up to April 2016. We included studies which compared the treatment effect of an overdenture to conventional denture on nutrition, in which primary outcomes included changes in intake of macronutrients and/or micronutrients and/or indicators of nutritional status. Two reviewers independently evaluated eligible studies and assessed the risk of bias. We used a fixed effects model to estimate the weighted mean difference (WMD) and 95% CI for change in body mass index (BMI), albumin and serum vitamin B12 between overdenture and conventional denture 6 months after treatment.
Results Of 108 eligible studies, 8 studies involving 901 participants were included in the narrative appraisal. Four studies reported changes in markers of nutritional status and nutrient intake after treatment with a prosthetic, regardless of type. In a meta-analysis of 322 participants aged 65 years or older from three studies, pooled analysis suggested no significant difference in change in BMI between an overdenture and conventional denture 6 months after treatment (WMD=−0.18 kg/m2 (95% CI −0.52 to 0.16)), and no significant difference in change in albumin or vitamin B12 between the two treatments.
Conclusions The modifying effect of overdenture treatment on nutritional status might be limited. Further studies are needed to evaluate the effectiveness and efficacy of denture treatments.
- implant-supported overdenture
- dental prosthesis
- meta-analysis
- nutrient
- nutrition assessment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first meta-analysis of the treatment effect of a mandibular implant supported overdenture compared with a conventional denture on nutritional status in edentulous patients.
This study has several limitations: small sample size, short follow-up period, target population and limited outcomes for nutrient intake or nutritional status in the included studies.
However, our narrative appraisal and quantitative analysis indicate important strategies for further studies of denture treatment on malnutrition.
Introduction
Nutrition is an important determinant of health, including immune function, cognitive function and mortality in the older population.1 The prevalence of malnutrition is increasing in this population, and a recent survey reported that as many as 46.2% of older adults were classified as at risk of malnutrition.2 The incidence of malnutrition is influenced by multiple biological, physiological and pathological factors, including dental status.1 Several observational studies have shown that intakes of nutritious foods, macronutrients and micronutrients, and nutritional status were lower in those who were unable to fully masticate due to teeth loss, ill fitting dentures or edentulousness.3–8
The prevalence of edentulousness is still high in some countries.9 Indeed, a survey from the WHO showed that as many as 78% of adults aged 65 years or older were edentulous.9 For the elderly edentulous, a conventional complete denture is effective for improving masticatory performance, appearance, and the ability to engage in social and interpersonal activities.10 Moreover, many studies report that prosthetic treatments modified dietary patterns and improved the variety of food intake.11–16 As adults aged 60 years or older may exceed more than 20% of the total population worldwide by 2050,17 the need for conventional denture treatment in public health will increase as the population ages.
Nevertheless, a default treatment for edentulous, namely a mandibular denture, sometimes loses stability and retention.18 The lack of stability and retention of the denture would lead to pain in eating, concerns about aesthetics and the negative impact of dentures in social situations. The mandibular implant supported overdenture, a removable prosthetic device that overlies and is supported by retained implants, was developed to solve these problems. Although the current cost of an overdenture is estimated to be 1.6–1.8 times higher than a conventional denture,18 treatment time does not differ much. Several studies have demonstrated the superiority of an overdenture over a conventional denture for both physical and psychological factors, including masticatory performance, denture stability, food avoidance and oral health related quality of life.12–15 ,19 Given that the psychosocial factors of dentures are considered to be as important as masticatory performance in determining food choice,20 these results indicate that treatment with an implant supported overdenture will encourage the intake of more kinds of foods than a conventional denture and thereby contribute to the improvement of nutritional status, albeit at some expense.
A number of studies reported that markers of nutritional status, such as the Mini Nutritional Assessment (MNA) and albumin, or intake of nutrients such as vitamin B12 and vitamin E, differed following overdenture treatment compared with conventional denture.13 ,15 ,19 In contrast, other studies showed no difference between overdenture and conventional denture in their effect on markers of nutritional status or nutrient intake.12 ,21–23 This inconsistency is exacerbated by the small sample sizes in some of these studies, which prevented assessment of the clinical effectiveness of overdenture treatment. Thus the effect of overdenture treatment on nutrition remains unclear.
Here we conducted a systematic literature review and meta-analysis to investigate whether overdenture treatment provides greater improvement in nutrient intake and markers of nutritional status than treatment with a conventional denture in edentulous patients.
Methods
We conducted a systematic literature review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.24 Our research question for this review was “Does treatment with a mandibular implant supported overdenture provide better improvement than a conventional denture in nutrient intake (macronutrients and micronutrients) or markers for nutritional status (body mass index (BMI), MNA and albumin) in edentulous patients?”
We searched Medline, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) for eligible studies. Medline was searched for papers published between 1946 and April 2016; EMBASE for those published between 1974 and April 2016; and CENTRAL for those published in issue 4, 2016. The search strategies for each database were constructed based on our primary outcomes and are shown in online supplementary appendix S1. We did not set a language restriction in the search.
supplementary appendix
We set the following eligibility criteria for literature screening: human subjects, with the study design of either a randomised control trial (RCT), cohort study or case control study. To be eligible, the intervention or exposure had to include a prosthetic treatment, such as a denture. Primary outcomes included change in intakes of macronutrients (ie, proteins, fats and carbohydrates) and/or micronutrients (eg, vitamins and calcium) and/or indicators for nutritional status. To assess nutritional status, we used BMI, MNA and albumin as markers because these are considered to be screening tools for malnutrition or nutritional markers.1 We additionally investigated the following efficacy of dentures as secondary outcomes: change in masticatory performance, denture stability, oral health related quality of life or food choice.
Two reviewers (TY and KI) independently screened titles and abstracts for eligible studies. Inter-examiner reliability was 0.73 by κ statistics. Full text articles were obtained for further screening if the information in the abstract met the eligibility criteria or if the abstract was not available. Studies were included in this review if a target prosthetic treatment was clearly stated; comparison of prosthetic treatments (ie, overdenture vs conventional denture) was adequately conducted; and the change in macronutrient intake, micronutrient intake and/or markers of nutritional status were evaluated between treatment groups. Studies were excluded if they examined reverse causation in the association between dental and nutritional status or if findings were only reported in a poster, guideline, letter or protocol. Disagreements over the eligibility of a study were resolved by discussion between the reviewers.
One reviewer extracted data from included studies and the second reviewer checked the data. The extracted data were as follows: study design, setting, inclusion criteria, principal health problem in the participants, other health problems, number of interventions/exposure participants and non-completers, number of control participants and non-completers, treatment received, outcomes measured and assessment method, and follow-up period. If the included study did not report the variability of quantitative estimates required for meta-analysis—that is, SD, SE or 95% CIs for an outcome—we contacted the corresponding author for additional information by email.
Two reviewers (TY and KI) assessed the risk of bias in the included studies using the Cochrane collaboration's tool.25 This tool consists of seven domains for the risk of bias—random sequence generation, allocation concealment, blinding of participants and study staff, blinding of outcome assessment, incomplete outcome data, selective reporting and other sources of bias. As this assessment tool is designed for RCTs and controlled before and after studies,25 we used it to assess the risk of bias for controlled studies. We also took account of other sources of bias. The reviewers independently assigned a judgement of ‘low risk’, ‘high risk’ or ‘unclear risk’ of bias. Disagreements were resolved by discussion between the reviewers.
Statistical analysis
The weighted mean difference (WMD) and 95% CI for change in BMI between overdentures and conventional dentures 6 months after treatment were estimated using a fixed effects model, on the basis that the included studies were similar in study design, participants, type of treatment received, outcome measured and length of follow-up. The analysis was repeated separately for change in albumin and change in vitamin B12. Heterogeneity between studies was tested by the I2 statistics.26 All statistical analyses were performed using Stata V.11.2 software (Stata Corporation, College Station, Texas, USA).
Results
Screening and selection
A flow diagram of the screening and selection of studies is shown in figure 1. The Medline, EMBASE and CENTRAL searches identified 1004 studies. After removal of duplicates, 776 studies were screened by title and abstract. Of these, 108 articles were retrieved to assess eligibility, of which 100 were removed based on our inclusion and exclusion criteria, leaving 8 studies for inclusion in the narrative appraisal. Of these eight studies, Morais et al15 reported the SD or 95% CI of mean differences between baseline and follow-up in each group. Upon request, Müller et al,19 Hamdan et al,21 Awad et al13 and Gjengedal et al12 provided additional information on the outcomes for this review. However, the outcome measures (anthropometric, macronutrient or micronutrient data) and assessment method (objective or subjective) differed between studies, and only three studies were therefore included in the meta-analysis.
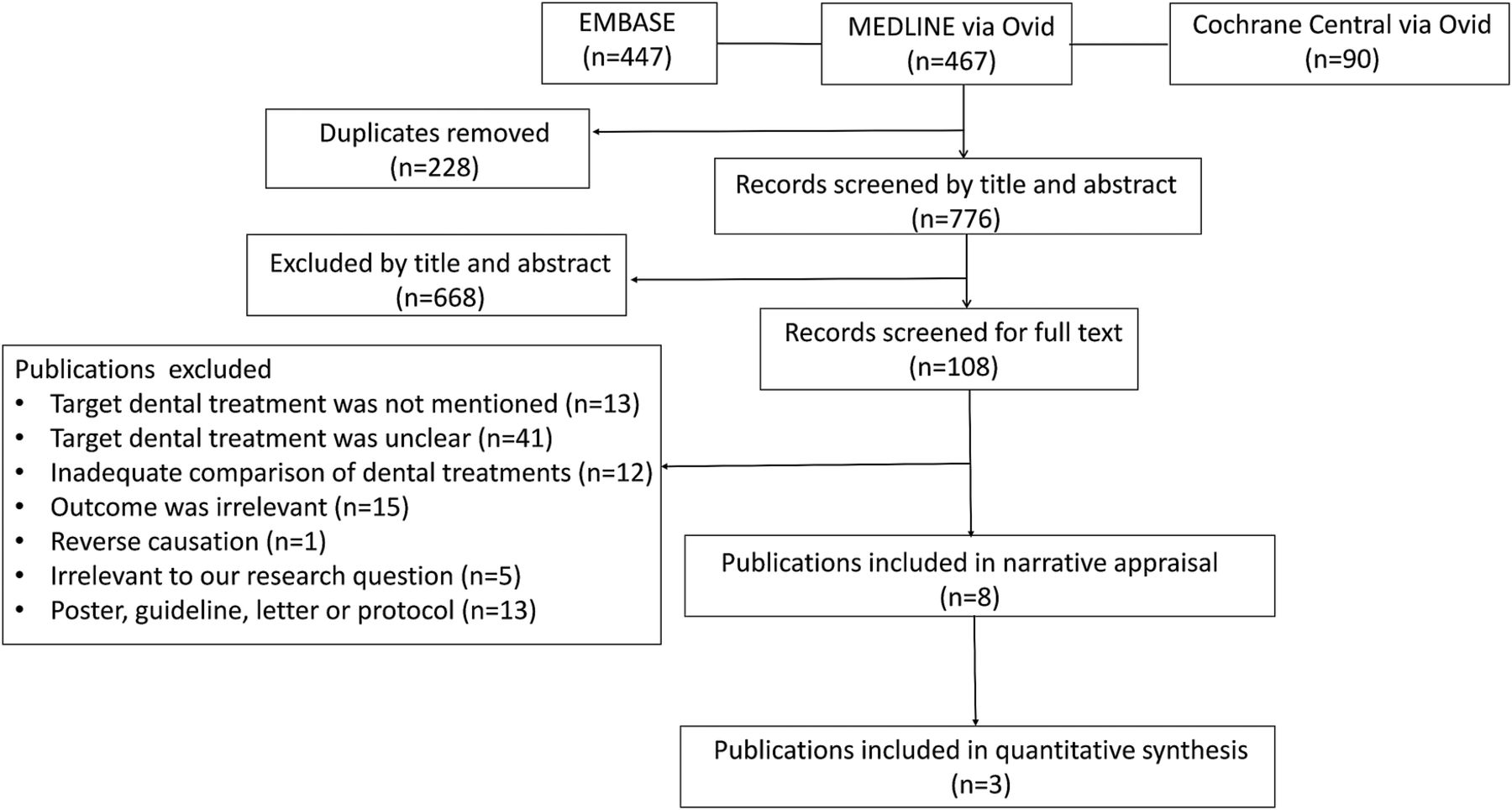
Flow diagram of screening and selection.
Characteristics of the included studies
Six RCTs12 ,13 ,15 ,19 ,21 ,23 and two prospective cohort studies22 ,27 investigated changes in nutrient intake and/or markers of nutritional status by interventional mandibular implant supported overdenture treatment (table 1). A total of 901 participants were included in this review. Five studies had a sample size of <100 participants and only three studies included over 100 participants (table 2).13 ,21 ,23 All studies were conducted in a hospital. One study focused on participants with diabetes.23
Characteristics of included studies
Intervention/exposure of included studies
Primary outcome
We divided outcome measures into three groups: macronutrient intake, micronutrient intake and markers of nutritional status (table 3).
Outcome of included studies
Macronutrient intake
Intakes of protein, total, saturated or unsaturated fat, and carbohydrate were measured as indicators of macronutrients. Four studies assessed a change in protein intake12 ,21 ,23 ,27 but found no significant differences in protein intake within or between groups, regardless of treatment type. In contrast, one study reported significant decreases in total fat after overdenture and conventional denture treatments (−1.5% energy in the overdenture group and −4.6% in the conventional denture group at 12 months).27 However, no differences were found between the groups. Three other studies found no significant difference in total, saturated or unsaturated fat within or between groups.12 ,21 ,23
For carbohydrates, one study with follow-up at 12 months or more found a significant increase in percentage contribution to energy intake by 1.2% in the overdenture group and 5.3% in the conventional denture group.27 In contrast, three other studies found no significant difference within or between groups.12 ,21 ,23
Micronutrient intake
Many different micronutrients were measured in the included studies. Here we focused on calcium, dietary fibre, magnesium and vitamins as indicators of micronutrients because some observational studies reported that these micronutrients were lower in those who were unable to fully masticate due to teeth loss, ill fitting dentures or edentulousness.3 ,6–8 With regard to micronutrient intakes measured by interview, questionnaire or both, none of the five studies found any differences in micronutrient intake within or between groups.12 ,21–23 ,27
Markers of nutritional status
Four studies assessed a change or difference in BMI as an indicator of nutritional status. Of these studies, one RCT with follow-up at 12 months reported a 0.41 kg/m2 decrease in BMI for both the overdenture and conventional denture groups using a linear mixed effects regression model, allowing for repeated measures and potential confounders.19 In contrast, three studies showed no significant change or difference in BMI between groups at the 12 month follow-up.13 ,15 ,22
One study evaluated a change in MNA as an indicator of nutritional status after prosthetic treatment but the result showed no significant change after treatment within or between groups.19
One study with follow-up at 6 and 12 months reported significant decreases in serum vitamin B6 in the overdenture and conventional denture groups.13 In contrast, one study with follow-up at 6 months showed an increase in serum vitamin B12 of 27.6 pmol/L and an increase in albumin of 1.1 g/L in the overdenture group.15
Assessment methods of macronutrients or micronutrients
Intakes of macronutrients or micronutrients were assessed using multiple pass 24 hour dietary recall by telephone interview or by a prospective food diary with dietician or technician follow-up. All dietary recalls were conducted by trained personnel using a structured template. Three studies reported that nutrient data were calculated from the collected information using validated computer programmes,12 ,21 ,23 but one study did not show the calculation method.27
Secondary outcome
Of the eight included studies, five examined the efficacy of an overdenture as a secondary endpoint. One study reported that overdenture treatment increased denture satisfaction (DS-VAS), oral health related quality of life (Oral Health Impact Profile-EDENT), maximum voluntary bite force and denture stability compared with conventional denture treatment.19 All four studies which investigated changes in food choice after intervention showed that overdenture treatment offered more choice of food items such as beef or whole fruit.12 ,13 ,15 ,22
Risk of bias
Online supplementary appendix S2 summarises the risk of bias in the included studies. All six RCTs reported an adequate method of random sequence generation. Of these, one study reported allocation concealment19 while the rest either did not report it or did not conduct it appropriately. For objective measurements, we considered that blinding of assessors was appropriately conducted. However, for questionnaires or interviews in nutritional assessment, most studies did not clarify whether the assessors were subject to blinding. Three studies reported methods for dealing with incomplete outcome data13 ,19 ,21 but three studies did not explain how this was dealt with. With regard to selective reporting, some studies did not sufficiently report baseline data or outcomes of interest.12
supplementary appendix
Meta-analysis
Three RCTs provided information on BMI, albumin and serum vitamin B12 required for data pooling. Moreover, subject characteristics of these three studies were similar,13 ,15 ,19 allowing us to conduct meta-analyses for the three outcome measures. Although Müller et al19 provided data for 3, 6 and 12 months, and Awad et al13 provided data for 6 and 12 months, we restricted analysis to data at 6 months’ follow-up, which included the study by Morais et al.15 A total of 322 participants were included. Results showed no significant difference in change in BMI between an overdenture and conventional denture (WMD=−0.18 kg/m2; 95% CI −0.52 to 0.16; p=0.44) (figure 2). Similarly, there was no significant difference in change in albumin (WMD=−0.23 g/L; 95% CI −0.79 to 0.34; p=0.73) (figure 2) or vitamin B12 (WMD=−11.16 pmol/L; 95% CI −30.43 to 8.12; p=0.43) (online supplementary appendix S3). No heterogeneity was observed between studies (I2=0%). Publication bias was not tested since fewer than five studies were included.

{kind=link}
{kind=link}
Forest plot of change in body mass index (BMI kg/m2) and albumin (g/L) 6 months after treatment. CD, complete denture; IOD, implant supported overdenture; WMD, weighted mean difference.
supplementary appendix
Discussion
We conducted a systematic review and meta-analysis to investigate whether treatment with an implant supported overdenture improves nutrient intake and nutritional status compared with a conventional denture in edentulous patients. To our knowledge, this is the first meta-analysis of the treatment effect of overdenture on nutritional status. A narrative appraisal suggested that some markers of nutritional status and intake of nutrients changed after treatment, regardless of prosthetic treatment type. However, we found no report of significant differences in nutrient intake or nutritional markers between treatments. Similarly, our meta-analysis showed no significant change in nutritional status between the two treatments at 6 months after treatment among an older population. Although our hypothesis was not proven, our review and analysis indicate important strategies for further studies on malnutrition treatment.
Our hypothesis was that overdenture treatment facilitates the intake of a variety of foods, which in turn leads to better nutritional status than with conventional denture treatment. In particular, the increased consumption of meat facilitated by an overdenture might lead to an increase in serum vitamin B12.28 However, our narrative appraisal and quantitative analysis showed no evidence of a difference in nutritional change between these treatments. Rather, our pooled estimates suggested that the treatment effect on nutrient intake was opposite to the expected direction; namely, conventional denture treatment might have been associated with slightly more favourable levels of albumin and vitamin B12 than overdenture treatment.
We speculate that overdenture treatment had less or no effect on nutritional status compared with a conventional denture for the following three reasons. First, the modifying effect offered by the treatment may be limited because all enrolled participants were aged 65 years or older; in other words, eating patterns and nutritional status might be more strongly impacted by declines in biological, physiological and sensory function with aging than by prosthetic treatments.1 ,29 Second, a 6 month follow-up period may not be long enough for longer term users of conventional dentures to adapt to the new overdenture treatment. More specifically, learning new motor skills or adapting existing motor patterns requires neuroplasticity, particularly in older persons,30 and the modification of eating patterns by overdenture treatment in our older participants might not have been sufficient to produce a measurable change in nutritional status in the short term. Finally, prosthetic rehabilitation alone may not have the effect of exerting a change in nutritional status. Since nutritional inadequacy in older persons can result from multiple factors—physiological, pathological, sociological, and psychological1 ,31—older populations may require a multidisciplinary approach to improving nutritional status. To prevent and treat malnutrition in older persons, the Nutrition and Dietetics Guideline recommends, based on high level evidence, that food provision methods be modified or feeding support be provided by health care assistants.32 Given that our narrative appraisal and other systematic review showed that denture stability, denture satisfaction or food choice were improved by overdenture treatment compared with a conventional denture,12 ,13 ,15 ,18 ,19 ,22 a prosthetic approach in combination with these interventions might support an improvement in nutritional status among older adults at risk of malnutrition.
A mandibular two implant supported overdenture costs more than a conventional denture. According to an RCT that investigated the cost effectiveness of oral health related quality of life,33 the equalised annual costs were estimated at 625 Canadian dollars for an overdenture versus 399 dollars for a conventional denture, with the inclusion of aftercare. Another RCT estimated that the mean direct cost of overdenture treatment was 2332 Canadian dollars, or 2.4 times higher than conventional denture treatment.34 As the two treatments have similar time and cost requirements,35 the utility of overdenture treatment might be limited with regard to nutrition improvement.
Several limitations of this study warrant mention. First, we could not assess the impact of treatment on those who require nutritional therapy due to malnutrition, since the participants were likely to have been generally healthier than individuals in hospitals or healthcare institutions.1 Considering that many older adults are classified as at risk of malnutrition,2 generalisation of our results requires further study into the effects of prosthetic treatments on nutrition among an at risk population. Second, our use of BMI, albumin and serum vitamin B12 only as outcome measures might not have provided a full evaluation of nutritional status. It is true that BMI predicts disease risk in those who are underweight or obese, but measurement in older adults can be confounded by a loss of height caused by vertebral collapse or a change in posture caused by loss of muscle tone.1 Measurement can be further confounded by the presence of ascites and oedema.1 Moreover, the direction of a change in BMI can be either a positive or negative outcome, depending on the baseline characteristics of the individual participant, and pooled data can be difficult to interpret. Instead, measurement of skinfold thickness and muscular circumference of the arm would provide a better anthropometric assessment of nutritional status, although our review found that only a few studies investigated these indicators.1 Similarly, serum albumin can predict mortality in older people but is influenced by other factors such as inflammation and infection.1 In contrast, transferrin, saturated/unsaturated serum cholesterol and trace elements are more sensitive indicators of malnutrition.1 Future studies of the effect of prosthetic treatment on nutrition in older populations should therefore use these sensitive markers for anthropometric assessment of nutritional status in place of BMI and albumin.
Third, the quality of the included studies varied. Random sequence generation was adequately conducted in all RCTs but five of the studies did not report or conduct allocation concealment appropriately. Furthermore, most studies did not provide sufficient statistical consideration for incomplete data, or intention to treat analysis and statistical multiplicity. These issues might have led to the overestimation of treatment effect in these studies. Finally, since only three studies were included in the meta-analysis, the small sample size might not have been adequate for precise estimation of the pooled effect size and might have limited the generalisation of the study. In addition, we could not assess the possibility of publication bias due to the limited number of studies pooled.
Conclusions
We conducted a systematic review and meta-analysis of the effect of implant supported overdenture treatment on nutrient intake and nutritional status in edentulous patients. The narrative appraisal and meta-analysis demonstrated that, compared with conventional denture treatment, overdenture treatment did not have a greater effect on changes in BMI, albumin or vitamin B12 6 months after treatment among the older population. Considering cost effectiveness, the utility of overdenture treatment might be limited with regard to nutrition improvement. However, these present and previous results indicate that a multidisciplinary approach which includes overdenture treatment might support an improvement in nutritional status among older adults. Further intervention trials or observational studies are needed to evaluate the long term effectiveness and efficacy of denture treatments on nutrition in the wider population.
Acknowledgments
We thank Dr Harald Gjengedal, Dr Francois Herrmann, Professor Frauke Müller, Professor Martin Schimmel, Dr Nader Hamdan, Dr Manal A Awad and Professor Jocelyne Feine for providing additional data included in the meta-analysis. We thank Professor Bob Cumming for providing advice on discussion about geriatric medicine. We thank Jeremy Cullis for providing advice on the systematic literature search. We also thank Dr Guy Harris of DMC Corp for his review of the manuscript.
References
Footnotes
Contributors TY conceived and designed the study; TY and KI performed the reviews; TY extracted the data; KI and CMYL checked the extracted data; TY and CMYL analysed the data; TY wrote the manuscript; CMYL contributed to the initial revision of the manuscript; ALCM and SS contributed to the critical revision of the manuscript; and TY had primary responsibility for the final content. All authors read and approved the final manuscript.
Funding This research was partially supported by Mie University Hospital Seed Grant Program and Research Fund of Mie University.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.