Article Text

Abstract
Objectives To compare expression of interleukin (IL)-1β and tumour necrosis factor (TNF)-α in the conjunctiva of diabetic and non-diabetic patients with symptomatic moderate dry eye.
Setting and participants Nineteen diabetic patients with dry eye, 15 non-diabetic patients with dry eye and 14 diabetic patients without dry eye were recruited. The relative expression of IL-1β and TNF-α in conjunctival impression cytology (CIC) specimens was evaluated using immunofluorescent staining and in conjunctival biopsy specimens using immunohistochemical staining.
Results The diabetic dry eye group showed significantly higher grades of metaplasia than the non-diabetic dry eye and diabetic without dry eye groups (both p<0.05). There was no significant difference in the concentration of IL-1β and TNF-α in CIC specimens between the three groups (p=0.504 and p=0.310, respectively). The mean levels of IL-1β and TNF-α in conjunctival biopsy specimens from the diabetic dry eye group was significantly increased compared with the non-diabetic dry eye and diabetic without dry eye groups (p=0.002, p<0.001; p=0.001, p<0.001, respectively). Interestingly, IL-1β- and TNF-α-positive cells were mainly located in the basal layer of the conjunctival epithelium, and rarely seen in the apical conjunctival epithelium in the three groups. The levels of both IL-1β and TNF-α did not correlate with conjunctival squamous metaplasia grades.
Conclusions Levels of IL-1β and TNF-α in conjunctival biopsy specimens were increased in diabetic patients with dry eye, while levels of IL-1β and TNF-α in apical conjunctival epithelium were similar in the CIC specimens. These findings suggest that the inflammatory response is not limited to the surface of conjunctival epithelial cells, and is more serious in the basal layer of the epithelium, which may play an important role in the pathogenesis of dry eye in diabetic patients.
- dry eye
- diabetes
- conjunctiva
- inflammatory cytokine
- IL-1β
- TNF-α
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study only investigated interleukin (IL)-1β and tumour necrosis factor (TNF)-α in conjunctiva of diabetic patients with dry eye. Other inflammatory cytokines were not investigated.
It would have been better if the study included a group of patients without diabetes or dry eye. Also, the sample size is not large enough.
Introduction
As defined by the International Dry Eye Workshop (DEWS) in 2007, dry eye is a multifactorial disease of the tears and ocular surface, which results in discomfort, visual disturbance and tear film instability. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.1 The pathogenesis of dry eye has not been clearly established. However, there is increasing evidence that inflammation plays an important role in dry eye syndrome.2 ,3 Studies have shown elevated levels of inflammatory cytokines such as interleukin (IL)-1, IL-6, IL-8 and tumour necrosis factor (TNF)-α in the tear film and conjunctival epithelium.4 ,5 In a botulinum toxin B-induced murine dry eye model study, IL-1β and TNF-α were significantly upregulated in the corneal and conjunctival epithelia.6 Moreover, the symptoms and signs of dry eye improved markedly with topical anti-inflammatory agents such as corticosteroid and cyclosporin A.7 ,8
Systemic diseases such as diabetes can lead to dry eye by a variety of mechanisms.9 ,10 However, there has been no documented study on cytokine levels in the conjunctiva of diabetic patients with dry eye. In this study, we investigated the levels of IL-1β and TNF-α in the conjunctiva of diabetic and non-diabetic patients with dry eye, and compared the results with those from diabetic patients without dry eye. In conjunctival squamous metaplasia, the epithelium shows abnormal differentiation with reduced goblet cell density and decreased or abnormal expression of differentiation-associated antigens. Whether inflammation of the ocular surface is associated with conjunctival squamous metaplasia grades in diabetic patients with dry eye is not yet clear. The correlation between IL-1β and TNF-α levels in conjunctival biopsy specimens and conjunctival squamous metaplasia grades in diabetic patients with dry eye was also analysed.
Patients and methods
All subjects were recruited from Tianjin Medical University Eye Hospital. The study followed the tenets of the Declaration of Helsinki and was approved by the Tianjin Medical University Institutional Review Board. The Institutional Review Board approved the consent procedure. Before examination, each patient gave written informed consent. Three groups of patients were studied: diabetic with dry eye; non-diabetic with dry eye; diabetic without dry eye. Age and gender of each group were matched. The demographic characteristics of these patients are presented in table 1. The diagnostic criteria of dry eye used in this study primarily comply with those defined by the Japanese Dry Eye Society in 2006.11 Inclusion criteria for moderate dry eye were determined according to the Ocular Surface Disease Index (OSDI) questionnaire: OSDI ≤32 and ≥13; break-up time (BUT) ≤10 s; or Schirmer I test ≤5 and ≥2 mm.12
Demographic characteristics of study patients
The following resulted in exclusion from the study: history of ocular surgery and laser treatment; use of topical eye drops for the preceding 3 months; use of systemic medications affecting dry eye; contact lens wear; abnormalities in the cornea, conjunctiva or eyelid; any major systemic diseases, other than diabetes mellitus, affecting tear secretion. All patients underwent ophthalmological examination, and the examinations were performed in both eyes in each subject. The data for the worst eye were taken for analysis. The test of tear film, BUT, was repeated three times and the average was recorded. The Schirmer test was performed without anaesthesia, and the length of wet filter paper (in mm) was recorded. The data are shown in table 2.
Tear break-up time (TBUT) and Schirmer test results for study patients
Age is expressed as mean±SD: non-diabetic dry eye vs diabetic without dry eye, p=0.795; non-diabetic dry eye vs diabetic dry eye, p=0.059; diabetic without dry eye vs diabetic dry eye, p=0.1.
Impression cytology
After topical anaesthesia with 0.5% proparacaine hydrochloride, strips of cellulose acetate filter paper (MFS membrane filters; Advantec MFS, Dublin, California, USA; 6.2 mm diameter) were applied to the temporal bulbar conjunctiva adjacent to the corneal limbus, pressed gently with blunt, smooth-tipped forceps for 2–3 s, and then removed. The specimen was fixed in 4% paraformaldehyde for more than 10 min and stained with periodic acid–Schiff. Five random areas of each sample were photographed using an optical microscope. Finally, the outcomes for a single sample score were averaged. The degree of squamous metaplasia was graded from 0 to 3 as described by Nelson.13
Conjunctival impression cytology (CIC) samples for immunofluorescence
Impression cytology specimens were obtained from the upper temporal side of the conjunctiva, 1 mm behind the limbus after instillation of topical anaesthesia. The CIC samples were obtained using a sterile, single-packed Biopore membrane (Millicell CM 0.4 μm PICM 03050; Millipore, Bedford, Massachusetts, USA). The sample was fixed in 4% paraformaldehyde, left at room temperature for more than 15 min, washed three times with phosphate-buffered saline (PBS), and incubated with blocking serum. The sample was then divided into three parts. Antibody to IL-1β and TNF-α (mouse polyclonal IgG; Santa Cruz Biotechnology) was applied to two parts of the membrane overnight at 4°C. The next day, the membranes were washed three times (10 min each) in PBS and incubated for 1 hour with fluorescein isothiocyanate-conjugated secondary antibody at room temperature. The third part served as a negative control, treated only with antibody diluent and secondary antibody. Specimens were counterstained with Hoechst 33342 nuclear staining dye (1:1000; Molecular Probes, Eugene, Oregon, USA) for 5 min and mounted. Sections were visualised with a fluorescence digital microscope (Olympus, Tokyo, Japan). Positive epithelial cells were counted in 10 different fields. At least 50 cells were counted, and the data expressed as percentage of positive cells. The whole slide was screened and counted as positive if at least one positive cell could be detected.
Immunohistochemistry of conjunctival biopsy specimens
Conjunctival biopsy specimens were obtained from the upper temporal conjunctiva of all the patients the next day. After fixation, endogenous peroxidases were quenched with 0.3% H2O2 in PBS for 10 min. After the sections had been blocked with 20% normal serum in PBS for 45 min, mouse monoclonal antibodies to IL-1β and TNF-α were applied separately and incubation carried out. After the sections had been washed, they were incubated with biotinylated secondary antibodies. The samples were then incubated with 3,3′-diaminobenzidine (NovaRed; Vector Laboratories) peroxidase substrate and counterstained with Mayer's haematoxylin. Some sections were treated with the secondary antibody alone as a control. IL-1β- and TNF-α-positive cells were counted over a length of 1500 µm of the conjunctival epithelium. The results were expressed as the number of positive cells per linear 300 µm.
Statistical analysis
Statistical analyses were performed using SPSS V.19.0. One-way analysis of variance was used to compare the cytokine levels in the biopsy specimens and the conjunctival squamous metaplasia grades between groups. The Fisher exact test was used to compare the cytokine levels in CIC specimens between groups. Spearman correlation coefficients were calculated for the correlation between cytokine levels in biopsy specimens and conjunctival squamous metaplasia grades. p Values of <0.05 were considered significant.
Results
Conjunctival impression cytology
The squamous metaplasia results for the three groups are given in table 3. The average grade of conjunctival squamous metaplasia was significantly higher in the diabetic dry eye (1.78±0.28) group than the non-diabetic dry eye (1.35±0.34) and diabetic without dry eye (1.29±0.34) groups (both p<0.05). Impression cytology specimens from the subjects are shown in figure 1.
Squamous metaplasia grades and IL-1β and TNF-α levels in conjunctival biopsy specimens

(A) Impression cytology specimen from a non-diabetic patient with dry eye showing large epithelial cells and increased nucleocytoplasmic ratio. (B) Specimen from a diabetic patient without dry eye showing increased nucleocytoplasmic ratio. (C) Specimen from a diabetic patient with dry eye showing multinucleated and small nuclei (arrow), even pyknotic or absent nuclei. Scale bar=20 µm.
Immunofluorescent staining of the IL-1β and TNF-α cytokines in CIC specimens
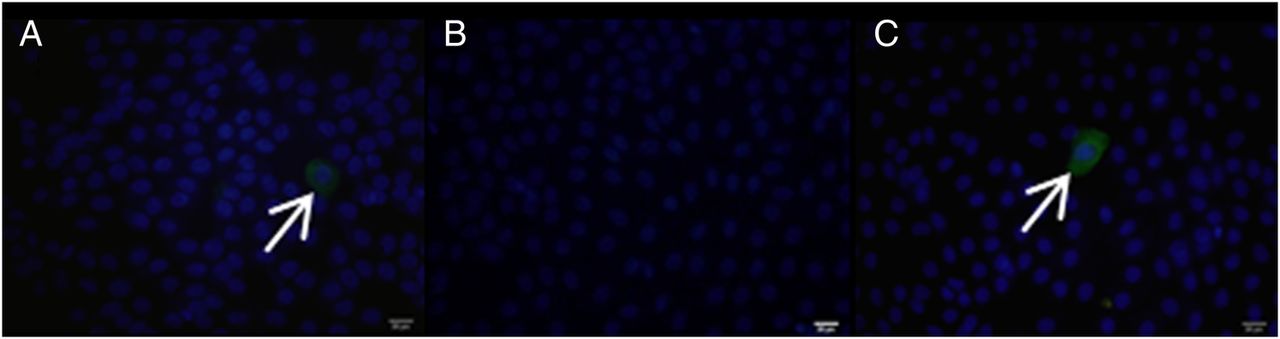
Immunofluorescence was used to evaluate the relative levels of expression of IL-1β and TNF-α in apical conjunctival epithelium. IL-1β- and TNF-α-positive cells were barely detectable in all three groups (figures 2 and 3). IL-1β and TNF-α expression did not differ significantly between the three groups (p=0.504; p=0.310). The mean percentages of IL-1β- and TNF-α-positive cells are shown in table 4.
IL-1β and TNF-α cytokines in conjunctival impression cytology specimens
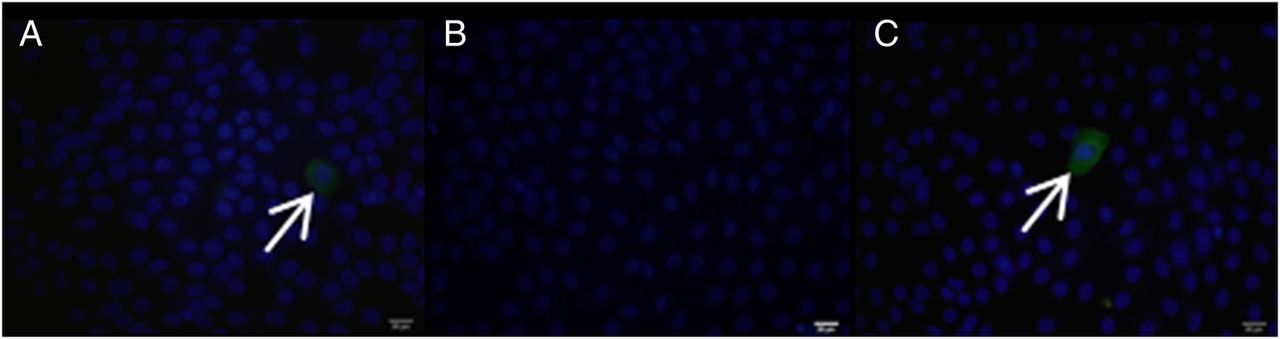
Expression of interleukin (IL)-1β in conjunctival epithelial impression cytology samples (green, arrow). Nuclear staining: blue. (A) Specimen from a non-diabetic patient with dry eye. (B) Specimen from a diabetic patient without dry eye. (C) Specimen from a diabetic patient with dry eye. Scale bar=20 µm.
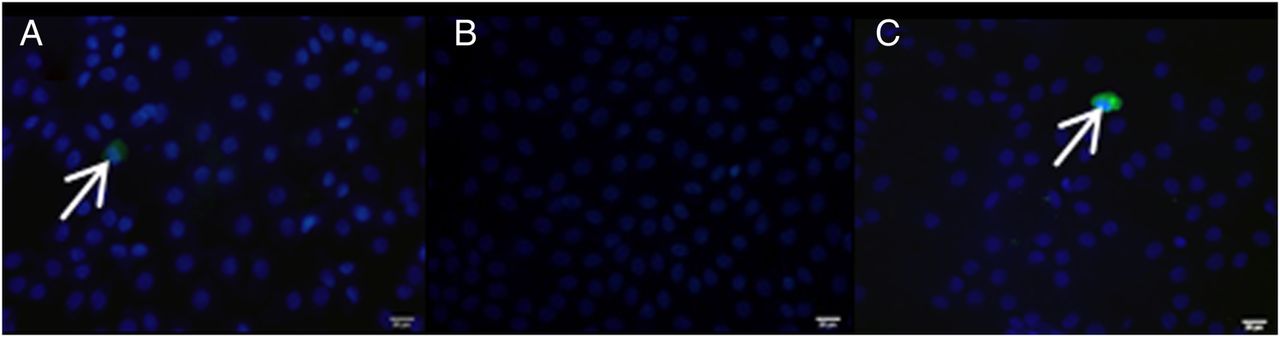
Expression of tumour necrosis factor (TNF)-α in conjunctival epithelial impression cytology samples (green, arrow). Nuclear staining: blue. (A) Specimen from a non-diabetic patient with dry eye. (B) Specimen from a diabetic patient without dry eye. (C) Specimen from a diabetic patient with dry eye. Scale bar=20 µm.
Immunohistochemical staining of IL-1β and TNF-α in conjunctival biopsy specimens
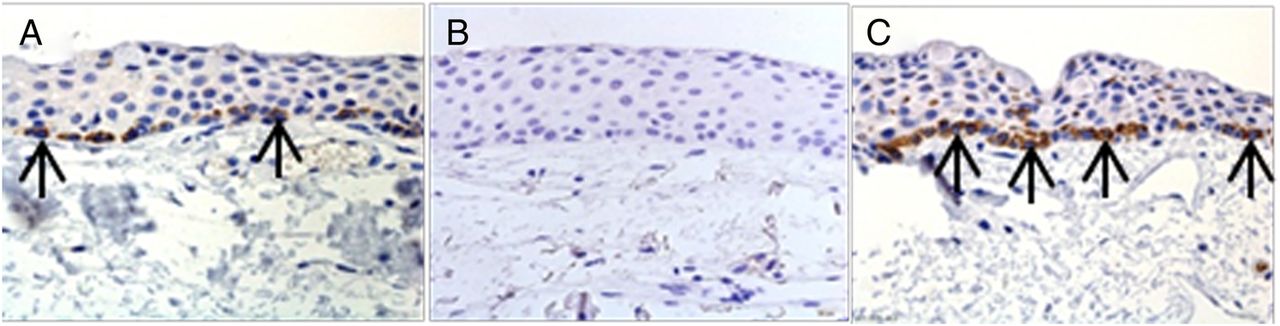
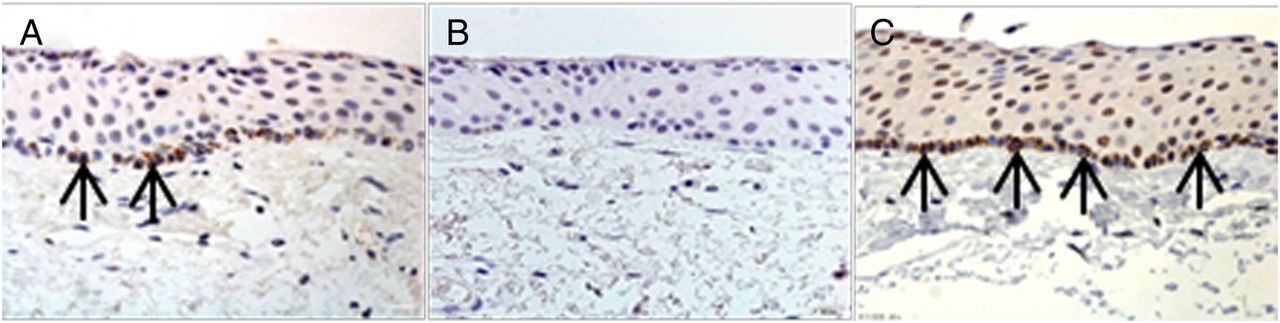
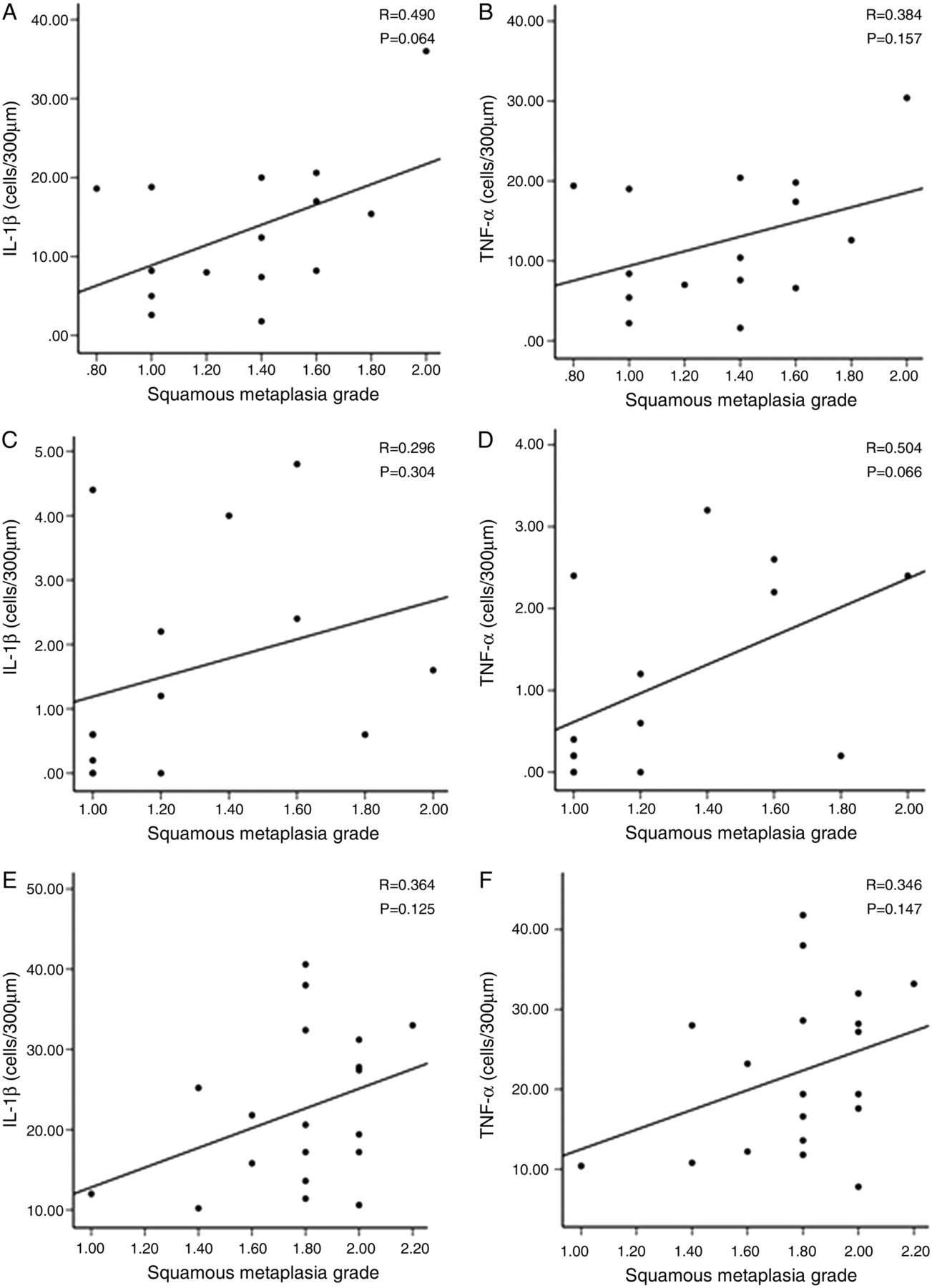
Immunohistochemical staining showed higher levels of IL-1β and TNF-α in the conjunctival epithelium of diabetic patients with dry eye than in that of non-diabetic patients with dry eye and diabetic patients without dry eye. The mean density of IL-1β- and TNF-α-positive cells is shown in table 3. Interestingly, the density of IL-1β- and TNF-α-positive cells was higher in the basal layer of the epithelium in all three groups (figures 4 and 5). The density of neither IL-1β- nor TNF-α-positive cells correlated significantly with the squamous metaplasia grades. The results of the correlation analysis between density of IL-1β- and TNF-α-positive cells and conjunctival squamous metaplasia grades are presented in figure 6.

Immunohistochemical analysis of interleukin (IL)-1β (arrow) in conjunctival tissue. Positive staining for IL-1β is observed in specimens from a non-diabetic patient with dry eye (A). IL-1β is barely detected in a diabetic patient without dry eye (B), and the strongest staining for IL-1β is observed in specimens from a diabetic patient with dry eye (C). Positive cells are in the basal layer of the epithelium. Scale bar=20 µm.
Immunohistochemical analysis of tumour necrosis factor (TNF)-α (arrow) in conjunctival tissue. Positive staining for TNF-α is observed in specimens from a non-diabetic patient with dry eye (A). TNF-α is barely detected in specimens from a diabetic patient without dry eye (B), and the strongest staining for TNF-α is observed in specimens from a diabetic patient with dry eye (C). Positive cells are in the basal layer of the epithelium. Scale bar=20 µm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between levels of interleukin (IL)-1β and tumour necrosis factor (TNF)-α and squamous metaplasia grades in the non-diabetic dry eye group (A for IL-1β, R=0.490, p=0.064; B for TNF-α, R=0.384, p=0.157), diabetic without dry eye group (C for IL-1β, R=0.296, p=0.304; D for TNF-α, R=0.504, p=0.066) and diabetic dry eye group (E for IL-1β, R=0.364, p=0.125; F for TNF-α, R=0.346, p=0.147). Neither IL-1β- nor TNF-α-positive cells correlated significantly with squamous metaplasia grades in the three groups.
Discussion
Diabetes mellitus can induce various kinds of ocular complications, such as cataract and diabetic retinopathy. Changes in tear film function and ocular surface induced by diabetes have been recognised.9 ,10 ,14 ,15 Many diabetic patients complain of dry eye symptoms, such as burning, foreign body sensation, dryness and blurred vision. An association between diabetes and dry eye has been proposed. In a randomised controlled trial carried out on 199 patients with type 2 diabetes, Manaviat et al16 reported a prevalence of 54.3%, using the diagnostic criterion that one of the tests, Schirmer or BUT, is pathological. Another study measuring tear osmolarity reported a prevalence of dry eye in 27.7% of diabetic patients.17 These results indicate that dry eye is a significant feature of the diabetic ocular surface disease. Previous reports also showed that dry eye correlated with the status of diabetic retinopathy, being more prevalent in people with proliferative diabetic retinopathy.14 ,17
Although the aetiology of dry eye in diabetic patients has not been clearly established, evidence exists to support the hypothesis that inflammation is a feature of all forms of dry eye.1 In this study, we investigated the levels of IL-1β and TNF-α in the conjunctiva of patients with moderate dry eye including diabetic and non-diabetic patients. We analysed the correlation between these cytokine levels and grades of conjunctival squamous metaplasia. IL-1β and TNF-α were chosen because they are the first wave of cytokines and stimulate cells to produce other factors that amplify the inflammatory response.18 ,19
The results of impression cytology analysis show that prominent squamous metaplasia existed in the diabetic dry eye group compared with the non-diabetic dry eye and diabetic without dry eye groups. In CIC samples from the diabetic dry eye subjects, larger and more polygonal epithelial cells were found and the nucleocytoplasmic ratios were increased. In some severe cases, multinucleated, pale-staining cytoplasm and small nuclei, even pyknotic or absent nuclei, were found. The mechanisms are not clear. Possible explanations for the findings are decreased trophic effects of trigeminal sensory nerves,20 ,21 changed composition of the tear film,10 and fluctuations and insufficiency of metabolic control.22 Conjunctival metaplasia did not significantly correlate with levels of IL-1β- and TNF-α-positive cells in the conjunctival biopsy specimens. Whether there is a correlation between conjunctival metaplasia and other inflammatory cytokines requires further study.
The levels of IL-1β and TNF-α in CIC samples were investigated. IL-1β- and TNF-α-positive cells were detected in immunostained CIC specimens in 6 of 19 diabetic dry eye patients. IL-1β-positive specimens could be seen in 2 of 14 diabetic patients without dry eye and TNF-α in 1 of 14 patients, suggesting that levels of IL-1β and TNF-α protein expressed in diabetic patients without dry eye are low and variable. Also, these cytokines may be just below the detection level of the assays performed. Very low levels of IL-1β and TNF-α were detected in all the positive specimens from the diabetic dry eye and non-diabetic dry eye groups, and specimens with strong staining intensity were observed in the diabetic dry eye group, whereas weak staining was found in the diabetic without dry eye group.
IL-1β and TNF-α levels were increased significantly in conjunctival biopsy specimens from diabetic patients with dry eye compared with non-diabetic patients with dry eye and diabetic patients without dry eye. Levels of IL-1β and TNF-α in conjunctival biopsy specimens from non-diabetic patients with dry eye were higher than in those from diabetic patients without dry eye. The mechanism of inflammatory cytokine production in patients with dry eye remains controversial.23 Animal model experiments show that desiccating environmental stress stimulates the production of inflammatory cytokines (such as IL-1β and TNF-α) from the ocular surface epithelium, and activates mitogen-activated protein kinase signalling pathways.24 ,25 Another study suggests that the hyperosmolar tear film stimulates the production and release of proinflammatory cytokines from the ocular surface epithelia.26 In our study, immunohistochemical staining of conjunctival biopsy specimens showed positive staining for IL-1β and TNF-α in specimens from patients with dry eye, especially those with diabetes. An interesting finding is that the density of positive cells was higher in the basal layer of the epithelium. Based on this finding, it is likely that basal conjunctival epithelial cells are the cellular source of the increased levels of inflammatory cytokines in patients with dry eye. Furthermore, this may be the consequence of the accumulation of advanced glycation end products (AGEs) in the basement membrane. AGEs may in some way activate proinflammatory cytokines leading to epithelial cell damage. Positive inflammatory cells are primarily located in the basal layer of the epithelium, which indicates that diabetic patients with dry eye and conjunctivitis may have more serious than clinical manifestations. It is possible that different areas of the conjunctiva release different amounts of inflammatory agents. The upper quadrant of the conjunctiva may have better protection from the upper eyelid than the lower quadrant. So, the upper part of the conjunctiva may suffer less from dry eye inflammation than the lower part.
In summary, our data indicate that IL-1β and TNF-α levels are significantly increased in the basal epithelium of diabetic patients with dry eye compared with non-diabetic patients with dry eye and diabetic patients without dry eye. This indicates that increased levels of inflammatory cytokines in the conjunctival epithelium may be an important factor in the pathogenesis of diabetic dry eye. Further studies are needed to establish an aetiological relationship between diabetes and dry eye.
References
Footnotes
CZ and LX contributed equally and are co-first authors.
Contributors Study concept and design: SZ, CZ and LX. Collection, management, analysis and interpretation of data: SZ, CZ and LX. Preparation, review and approval of the manuscript: SZ, CZ, LX, RW, YH, RY, LS, XL.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Medical Research Ethics Committee of Tianjin Medical University Eye Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.