Article Text

Abstract
Objectives Patients often suffer from disturbed sleep in hospital. Poor-quality sleep in hospitalised patients has been associated with significant morbidity and pharmacological sleep aids are often prescribed. The objective of this systematic review is to evaluate the comparative efficacy and safety of pharmacological interventions used for sleep in hospitalised patients.
Setting/participants We searched MEDLINE, Embase, the Cochrane database and grey literature for prospective studies that evaluated sleep in hospitalised adults after a pharmacological intervention.
Primary and secondary outcome measures Two reviewers assessed studies for inclusion and extracted data for efficacy outcomes, including sleep efficiency, sleep latency, sleep fragmentation and objectively measured sleep stage distribution. Risk of bias was assessed and meta-analyses were planned contingent upon homogeneity of the included studies.
Results After screening 1920 citations, 15 studies involving 861 patients were included. Medications studied included benzodiazepines, nonbenzodiazepine sedatives, melatonin, propofol and dexmedetomidine. Five studies were deemed to be of high quality. Heterogeneity and variable outcome reporting precluded meta-analysis in most cases. No consistent trends with respect to sleep efficiency, quality or interruptions were observed identifying a drug or drug class as superior to another or no treatment. Benzodiazepines appeared to be better than no treatment with respect to sleep latency, but this was not consistently demonstrated across all studies. Sleep stage distribution shows that sleep in hospital is dominated by stages N1 and N2.
Conclusions There is insufficient evidence to suggest that pharmacotherapy improves the quality or quantity of sleep in hospitalised patients suffering from poor sleep. No drug class or specific drug was identified as superior even when compared to placebo or no treatment. Although 15 studies were included, the quality of evidence was limited by their quality and size. Larger, better-designed trials in hospitalised adults are needed.
- SLEEP MEDICINE
- CLINICAL PHARMACOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The use of a validated systematic search strategy of multiple databases to identify relevant studies.
Article screening and data extracted independently by two investigators.
The research team consisted of physicians, pharmacists, an epidemiologist/methodologist, a sleep expert and pharmacotherapy specialists.
The studies included were typically small, outcomes were often measured subjectively and most studies did not have a standard approach to the evaluation of safety.
Not all drugs currently being used in clinical settings were identified in clinical trials and comparative trials were identified without placebo controls for many drugs.
Background
Sleep disturbances, including difficulty initiating sleep, fragmented and non-restorative sleep, occur in up to 50% of acutely ill hospitalised patients.1 Hospitalised patients routinely suffer from sleep disorders attributed to pathophysiological and environmental factors.2 ,3 In a study of 280 hospitalised elderly patients, 21% reported new-onset insomnia, 38% reported moderate or severe insomnia and 38% reported sleep disturbances during admission.4 The transient nature of acute illness coupled with the displacement and hospitalisation of patients represent unique features that differentiate insomnia associated with acute illness and hospitalisation from insomnia in otherwise healthy people. Sleep deprivation has been associated with poor wound healing, memory disorders, delayed ventilator weaning, delirium and mortality.5–8 Given the frequency of sleep disorders experienced by hospitalised patients and their associated outcomes, interventions to improve sleep are frequently attempted.1 ,9 ,10 Non-pharmacological interventions such as relaxation techniques and regulation of light/noise exposure are often tried to counter new-onset sleep disorders related to the environment.1 ,10 However, a systematic review of non-pharmacological interventions for sleep compared to no intervention (in hospitalised but non-critically ill patients) did not confirm a positive effect, citing a lack of high-quality studies.11 While environmental factors (related to light, noise and activity) are common in hospital and particularly in the intensive care unit (ICU), limiting the potential impact of these on sleep quality is not always easily accomplished. Accordingly, sedative and hypnotic pharmacotherapy is used in up to 88% of hospitalised patients.12
Currently, there are no evidence-based recommendations or guidelines to direct the choice of hypnotic drugs in the hospital setting, yet there are a plethora of agents that are used. The objective of this systematic review was to identify, synthesise and summarise the existing evidence on the efficacy and safety of pharmacological interventions used to improve sleep in hospitalised adults.
Methods
A protocol was developed prior to initiation of the review and was followed throughout the review process. The protocol is available from the authors electronically upon request.
Selection of studies
The Population, Intervention, Comparator, Outcome and Study design framework was used to formulate the research question for this systematic review.13 The population of interest was hospitalised adults in an attempt to identify acutely ill patients. Studies of patients in any acute care ward of a hospital (including medical, surgical and critical care units) were sought and non-hospitalised patients (ie, healthy volunteers, outpatients and long-term care facility residents) were excluded. We also excluded studies conducted solely in patients diagnosed with a primary psychiatric illness or sleep apnoea as these patient populations exhibit different baseline sleep patterns irrespective of environment.1 Interventions of interest for this systematic review included any pharmacological intervention for sleep used alone or in combination. This included benzodiazepines, antidepressants, antihistamines, imidazopyridines (eg, zolpidem), pyrazolopyrimidines (eg, zaleplon), cyclopyrrolones (eg, zopiclone), anticonvulsants (pregabalin/gabapentin), barbiturates, α-2-adrenergic agonists, antipsychotics, melatonin or melatonin receptor agonists and natural health products. Studies involving drugs that are no longer commercially available in any country were excluded. No restrictions on dose for any agent were employed. Comparators of interest included placebo, no treatment or any other intervention.
Efficacy outcomes of interest were sleep efficiency, sleep latency, sleep interruptions and sleep stage distribution measured by any means, including polysomnography, bispectral index monitoring (BIS), actigraphy, sleep questionnaires for patient self-reporting or direct observation by a third party. However, studies solely relying on patient self-reporting for sleep outcomes of interest were excluded as subjective reports are poorly correlated with objective measures and biased by systematic over-reporting.14 ,15 Sleep efficiency is defined as hours spent asleep divided by period of observation (in hours) by study investigators, while sleep latency represents the duration of time taken to fall asleep. Sleep fragmentation is defined as the number of arousals or awakenings in a designated sleep period. Sleep stage distribution refers to the proportion of time a patient spends in each sleep stage in a given period of observation. Secondary clinical outcomes included length of stay, duration of mechanical ventilation, presence of delirium, occurrence of infection, cognitive function, pain, glucose control, hypertension, myocardial infarction and mortality. Safety outcomes of interest included overall occurrence of adverse events, serious adverse events, including those deemed life threatening, and withdrawal or discontinuation of therapy due to adverse events. Study design comprised randomised controlled trials of pharmacological interventions for sleep. Additionally, comparative cohort studies and prospective case series were included only if sleep was evaluated using polysomnography. The language of publication was restricted to English or French.16
Literature search strategy
Relevant studies were identified using a sequential search approach. Initially, an informal scoping exercise was conducted to identify potentially relevant trials in Ovid MEDLINE with key words such as ‘sleep’, ‘insomnia’, ‘drug therapy’ and ‘in-patient’. Relevant studies identified in the scoping exercise were provided to an information specialist to develop and validate a search strategy for Ovid MEDLINE, Embase and Cochrane from inception to 21 March 2016. The search strategy was peer-reviewed using PRESS (Peer Review of Electronic Search Strategies) by a second information specialist and validated using the studies identified in the scoping exercise.17 The detailed search strategy is provided in online supplementary appendix 1. In addition, the reference lists of included studies and reviews were screened.
Supplementary appendix
Grey literature was searched via conference proceedings and abstracts (Canadian Sleep Society, American Academy of Sleep Medicine and European Sleep Research Society) for the last 5 years, as well as clinical trial and systematic review registries, and Google Scholar.18
Titles and abstracts were independently reviewed for eligibility by two investigators (AM and SK). Full-text articles identified as potentially eligible at first-level screening were obtained and reviewed for eligibility independently by the same two reviewers. Discrepancies were resolved by discussion and consensus. The process of study selection was documented using a PRISMA flow diagram.19
Data extraction and risk of bias assessment
Study level data were extracted using a predesigned and piloted data collection form by one author (AM) and checked by a second (SK). Means and SDs were estimated using established methods when only medians and ranges were available from an included study.20 ,21 In addition to the clinical and safety outcomes, extracted study data included the following: study authors, year and journal of publication, country of study performance, funding source, group sample sizes, study inclusion criteria, age distribution, gender distribution, patient setting in hospital and relevant concomitant medication use. Risk of bias was assessed using the Cochrane Risk of Bias tool22 for randomised controlled trials and the Newcastle-Ottawa Scale23 for cohort studies. Risk of bias was not assessed for prospective case series, as the risk of bias is inherently high.
Synthesis of available studies
Clinical and methodological heterogeneity of the included studies was carefully considered to determine whether meta-analysis would be conducted. Clinical heterogeneity was assessed by comparing study populations, interventions and outcome measurements between studies.24 Methodological heterogeneity was assessed by comparing methods for intervention assignment, allocation concealment and blinding, as well as the extent of and reasons for loss to follow-up. If heterogeneity was not identified between trials and reporting of clinical outcomes was amenable to meta-analysis, a random-effects model was employed to calculate pooled risk ratios for dichotomous outcomes (ie, adverse events) and pooled mean differences for continuous outcomes (ie, sleep efficiency) using RevMan V.5.3 (the Nordic Cochrane Center, the Cochrane Collaboration, Copenhagen, Denmark).25 ,26 Studies were to be pooled by drug and by drug class and compared with active controls or placebo separately depending on the availability of data. In the event that 10 or more studies were pooled for any outcome, funnel plots would be created and visually inspected to assess for publication bias.22
The PRISMA statement and its 27-item checklist were used in developing the summary of findings for this review. A completed PRISMA checklist is provided in online supplementary appendix 2.19
Supplementary appendix
Results
Characteristics of included trials
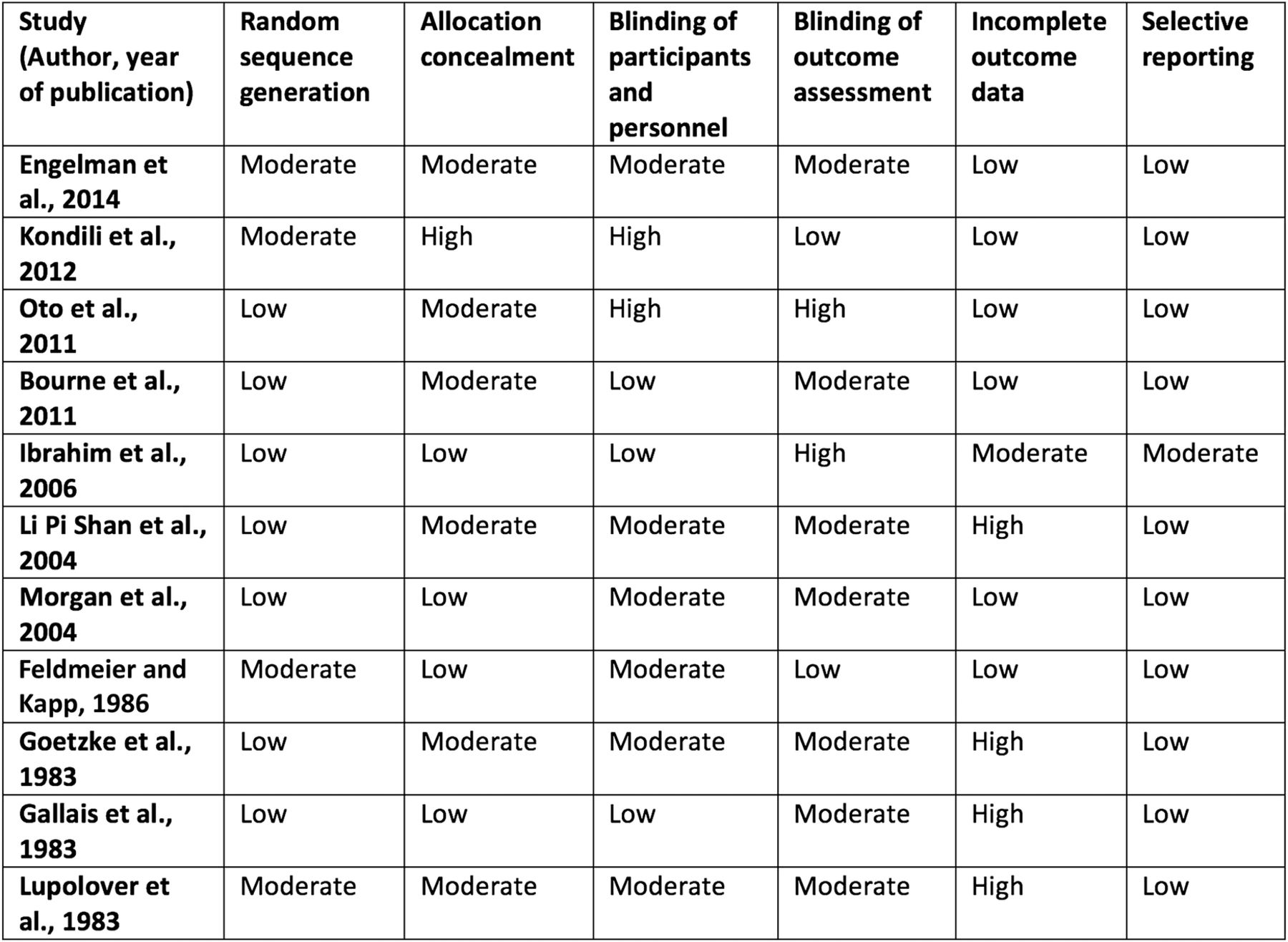
Our search strategy identified a total of 1920 citations, from which 11 randomised controlled trials, 2 prospective cohort studies and 2 case series, totalling 861 patients, met criteria for this review (figure 1). Twenty-eight studies were excluded because the only method of sleep assessment was via patient self-report. Eight studies were conducted in the ICU and included patients requiring mechanical ventilation. Seven studies were conducted in acute care hospital wards and included medical and surgical patients suffering from inadequate sleep. Six studies measured sleep using polysomnography, two used BIS and the remaining measured sleep using either third-party observation or a combination of third-party observation and patient self-report (tables 1 and 2). Medications studied included benzodiazepines, melatonin, propofol, zolpidem, zopiclone and dexmedetomidine. In most studies, the intervention was administered in the evening and sleep was evaluated over night; however, two of the ICU-based studies evaluated sleep while on continuous infusions of sedatives. Study durations ranged from 24 hours to 14 days. Seven of the randomised controlled trials had a high risk of bias in at least one criteria, which affected their overall quality (figure 2). The prospective cohort studies included were of high quality (figure 3).
Study characteristics: randomised controlled trials
Study characteristics: cohort studies and case series

Process of study identification and selection. *Prospective cohort studies not using polysomnography to measure sleep. RCT, randomised controlled trial.

Risk of bias for randomised controlled trials using the Cochrane risk of bias tool. Risk of bias assessed as low, moderate or high for each category.

Risk of bias for prospective cohort studies (NewCastle-Ottawa Scale).
Sleep efficiency
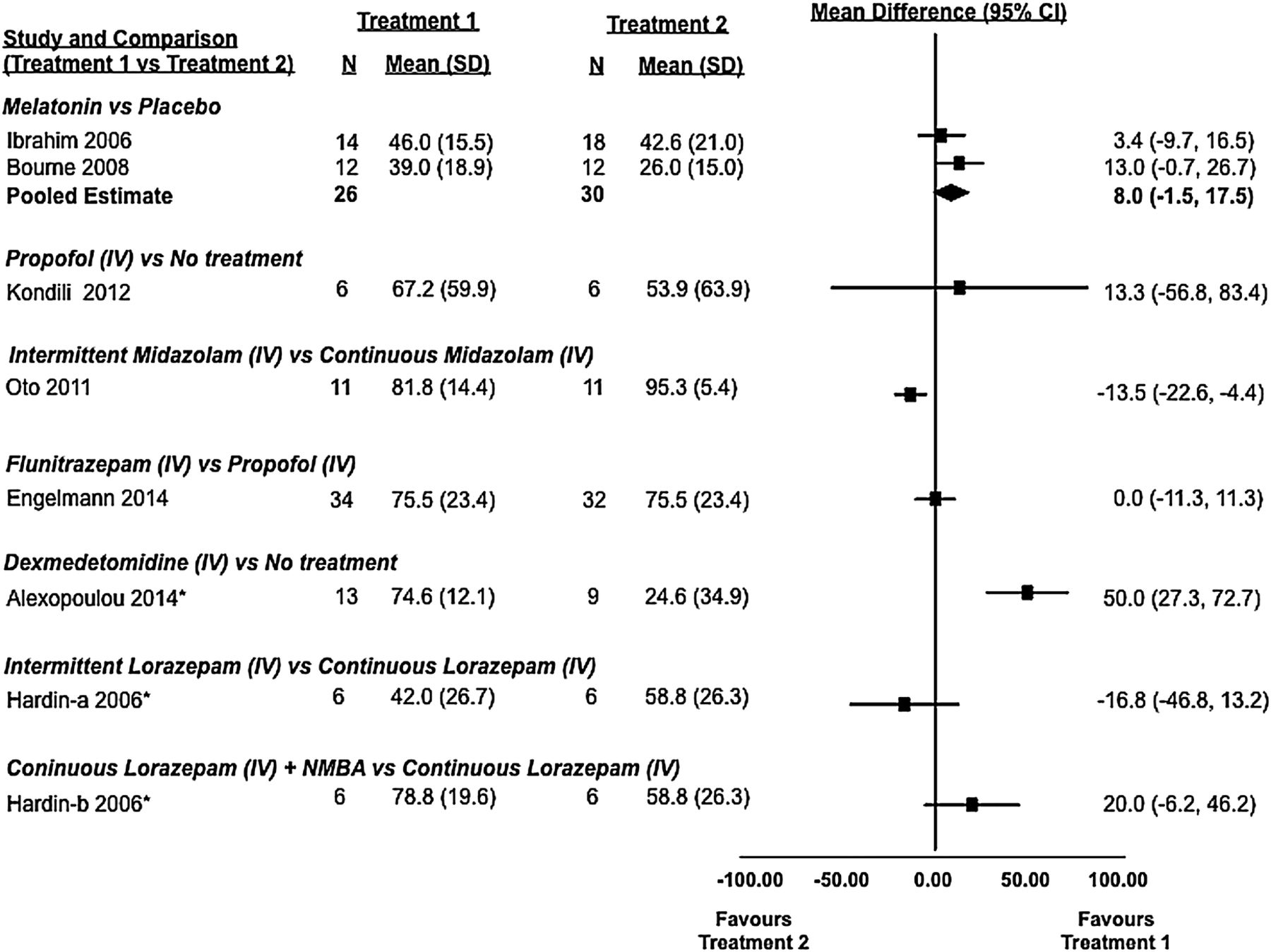
Sleep efficiency was evaluated in seven studies (five randomised controlled trials27–31 and two cohort studies32 ,33), of which two31 ,32 identified statistically significant differences (table 3, figure 4). Alexopoulou et al32 evaluated sleep with polysomnography in 13 of 16 enrolled patients over the course of three nights in a prospective crossover cohort study. On nights 1 and 3, patients received no treatment, while on night 2, they received dexmedetomidine. Polysomnography was not consistently viable, and only 10 patients contributed to the reported analysis, which showed that sleep efficiency was improved with dexmedetomidine (77.9% (SD 65.6–80.2%)) when compared to no treatment (15.8% (6.4–51.6%), p=0.002). In a study by Oto et al,31 two different dosing strategies for midazolam were compared in a randomised controlled trial of 22 critically ill patients. Both groups received sedation with a continuous infusion of midazolam, but one group had their infusions interrupted during the day. Sleep efficiency as measured by polysomnography was statistically significantly improved (p=0.047) in the group that did not have their infusion interrupted during the day (97% (91.1–97.8%) vs 81% (73.3–91.1%)). In a similar trial of 18 patients by Hardin et al,33 critically ill adults were administered lorazepam via continuous infusion or an interrupted dosing strategy; unlike in the previous study, differences between groups were not statistically significant (table 3, figure 4).
Summary of study findings, by outcome

Sleep efficiency: observed differences from randomised and non-randomised studies and from active and inactive controlled studies (7 studies and 188 patients). Sleep efficiency was defined as the number of hours spent asleep divided by the total hours of observation. In some studies, mean and SD values were estimated using an approached described in the Methods section. *, non-randomised study; iv, intravenous; NMBA, neuromuscular blocking agent.
Two randomised controlled trials (Bourne et al27 and Ibrahim et al28) that compared melatonin with placebo failed to show a statistically significant difference in sleep efficiency as measured by BIS or nurse observation. Similarly, two trials by Engelmann et al30 and Kondili et al29 comparing propofol to flunitrazepam and no treatment did not show statistically significant differences with respect to sleep efficiency as measured by BIS and polysomnography, respectively. Only the two placebo-controlled melatonin trials (total of 56 patients) were amenable to pooling of this outcome that revealed a non-statistically significant trend in favour of melatonin when compared to placebo (mean difference of 8.0% (95% CI −1.5% to 17.5%)).
Sleep latency
Sleep latency was evaluated in five studies. Owing to variability in assessment and reporting metrics between studies, forest plots were not created, and the appropriateness of meta-analysis was deemed low. Sleep latency data are reported for each study in table 3.
Two randomised controlled trials, Feldmeier and Kapp34 (n=50) and Gallais et al35 (n=51), compared the effects of midazolam and oxazepam to placebo. One randomised controlled trial by Lupolover et al36 (n=78) compared midazolam to oxazepam. Sleep latency was measured by third-party observation or patient questionnaire in all three studies. The studies by Feldmeier and Kapp and Gallais et al reported a statistically significant reduction in sleep latency with midazolam (15 mg orally) compared to placebo (median difference of 30–53%, p<0.05); however, only Feldmeier and Kapp34 found oxazepam (15 mg orally) to be superior to placebo (median difference 16%, p<0.05). Gallais et al35 found midazolam 15 mg orally to be superior to oxazepam 50 mg orally (table 3) as did Lupolover et al36 (15 mg doses for midazolam and oxazepam), but only after 3 days of treatment (table 3).
Two randomised control trials evaluated sleep latency with triazolam.37 ,38 Morgan et al (n=357) compared triazolam to zolpidem and placebo, while Goetzke et al (n=79) compared it to brotizolam and placebo. In both cases, drug therapy (any) appeared to be superior to placebo with respect to sleep latency; however, no statistical analysis was provided by Goetzke et al.38 No statistically significant differences were identified between the active arms of either study (table 3).
Sleep fragmentation
Sleep fragmentation was evaluated in five studies: three randomised controlled trials29–31 and two cohort studies32 ,33 (table 3, figure 5). Variability in treatments studied precluded the opportunity for meta-analysis. Two randomised controlled trials studied the effect of propofol on the number of awakenings compared to flunitrazepam30 or no treatment.29 Engelmann et al30 (n=66), using BIS, found that propofol (median: 0.6 arousals per hour of sleep) was associated with statistically significantly fewer sleep interruptions than flunitrazepam (median: 1.1 arousals per hour of sleep in critically ill patients, p=0.041). However, Kondili et al29 (n=12), using polysomnography, found insufficient evidence of a difference between patients receiving propofol (median (IQR) 4.8 (1.3–14.6) awakenings per hour of sleep) and those receiving no treatment (median (IQR) 8.1 (2.9–16.2) awakenings per hour of sleep).
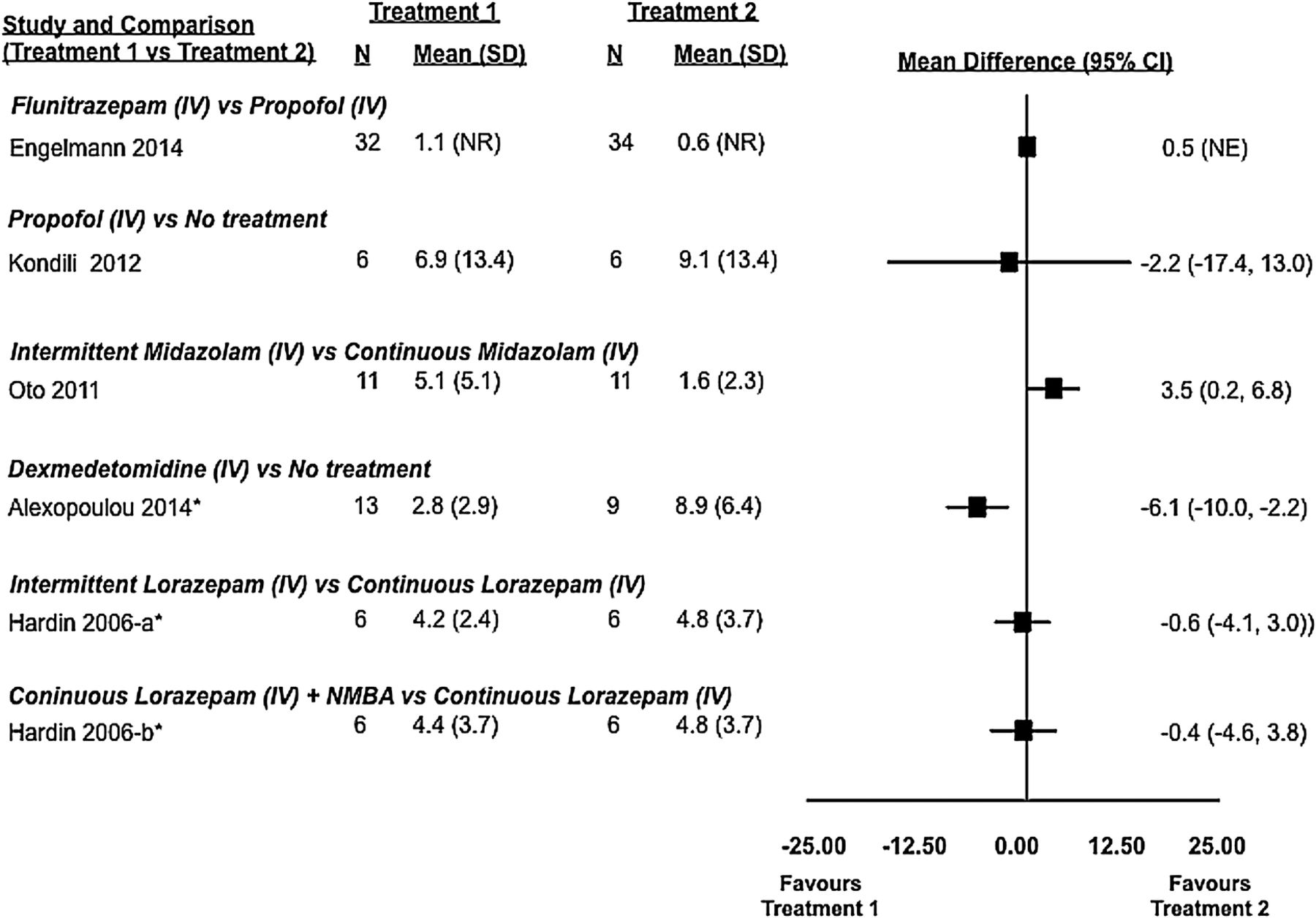
Sleep fragmentation: observed differences from randomised and non-randomised studies and from active and inactive controlled studies (5 studies and 125 patients). Sleep fragmentation was defined as the number of arousals or awakenings per hour of sleep. In some studies, mean and SD values were estimated using an approached described in the Methods section. *, non-randomised study; iv, intravenous; NE, not estimable; NMBA, neuromuscular blocking agent; NR, not reported.
Dexmedetomidine compared to no treatment was found to statistically significantly reduce the number of sleep interruptions in critically ill patients. Using polysomnography, Alexopoulou et al32 (n=23) found that patients receiving infusions of dexmedetomidine had a median of 2.2 (IQR 1.6–4.5) awakenings per hour, while those receiving no treatment had a median of 7.1 (IQR 1.6–4.5) awakenings per hour (p=0.0023).
Two trials comparing different dosing strategies for benzodiazepines in critically ill patients yielded conflicting results. Oto et al31 found that continuous infusions of midazolam were associated with fewer awakenings when compared to infusions incorporating daytime interruptions, while Hardin et al33 found no difference between continuous infusions of lorazepam (with and without a neuromuscular blocker) and an intermittent dosing strategy.
Sleep stage distribution
Two randomised control trials,29 ,31 two cohort studies32 ,33 and two case series39 ,40 evaluated sleep architecture using polysomnography in a total of 74 patients. Treatment effects from comparative studies are shown in figure 6, while data for all studies are found in table 3. Irrespective of treatment allocation, patients in hospital primarily experience light non-restorative sleep, corresponding to stages N1 and N2. Only Hardin et al (continuous infusion of lorazepam with or without neuromuscular blocker vs interrupted infusion) reported a proportion of sleep as stage N3 (restorative sleep), where stage N3 represented 32–50% of total sleep but insufficient evidence of a difference between groups. No other trial using polysomnography was able to describe meaningful amounts of stage N3 sleep. Rapid eye movement (REM) sleep was only described with midazolam infusions interrupted during the day (6.8%), continuous infusions of midazolam (2%), interrupted lorazepam infusions (3.6%) and the no treatment arm of the study by Kondili et al (1.4%).29 ,31 ,33 ,39 Given the variability in studied treatments, study designs and the limited number of overall studies, meta-analysis was not attempted.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sleep architecture: observed differences from randomised and non-randomised studies and from active and inactive controlled studies (4 studies and 59 patients). Sleep stage distribution defined as percentage of total sleep time patients spent in each stage. In some studies, mean and SD values were estimated using an approached described in the Methods section. *, non-randomised study; cont, continuous dosing; DEX, dexmedatomidine; int, intermittent dosing; iv, intravenous; LOR, lorazepam; MID, midazolam; NE, not estimable; NMBA, neuromuscular blocking agent; No Trt, no treatment; PRO, propafol.
Secondary outcomes
Delirium was not assessed in the included studies; however, Ibrahim et al28 evaluated agitation using the Riker Sedation-Agitation Scale and found no difference between melatonin (n=14) and placebo (n=18) groups. Cognitive function was evaluated in the study by Li Pi Shan and Ashworth41 using the mini mental state examination, and no difference was found between lorazepam (n=9) and zopiclone (n=9). Narcotic requirements were evaluated in the study by Oto et al.31 While more patients (9/11=81.8%) in the group assigned to midazolam infusions with daily interruption required opioids than those assigned to the continuous infusion group (4/11=36.4%), there was no difference in median dose between groups. In the study by Hardin et al33 (n=18), patients assigned to continuous infusions of lorazepam (n=6) required significantly more morphine (0.48±0.52 mg/kg/day) than those assigned to interrupted infusions (0.11±0.13 mg/kg/day) (n=6) or continuous infusions with neuromuscular blockade (0.14±0.32 mg/kg/day) (n=6) (p=0.031). No other differences were found between groups.
Duration of mechanical ventilation, length of stay, occurrence of infection, glucose control, hypertension, myocardial infarction and mortality were not described in any included study.
Safety
No study reported occurrence of serious life-threatening events. Seven of the 15 studies did not report any safety information in the methods or results. Of the remaining eight,27 ,30 ,34–38 ,41 no study reported any difference with respect to adverse events between the active treatment groups compared to the placebo or no treatment arms.
Engelmann et al30 reported that three patients developed respiratory depression after flunitrazepam administration requiring the insertion of a nasopharyngeal airway but not withdrawal from the study. One patient receiving dexmedetomidine in the study by Alexopoulou et al32 had the study drug discontinued for bradycardia (heart rate <50 bpm).
Patient conditioning, defined as somnolence or alertness the morning following administration of hypnotics, was reported in five studies. Four reported no differences between drugs and/or placebo.34 ,37 ,38 ,41 The study by Lupolover et al36 described an improved state on awakening by patient self-report in those taking midazolam compared to oxazepam.
Headache and nausea were the most commonly reported adverse events. Discontinuation of therapy due to nausea was only observed in the placebo group of Morgan et al.37 Allergic type skin reactions were reported in two patients—one was associated with triazolam; the other, described as pruritus, occurred in a patient with pancreatitis and whether the reaction was attributed to benzodiazepines or placebo was not specified in the study.36 ,38
Discussion
In this review, we set out to summarise the existing evidence and compare studies looking at the efficacy and safety of various pharmacological agents for sleep. Fifteen studies encompassing 861 patients met our inclusion criteria; however, clinical and methodological heterogeneity and variable outcome reporting were judged to preclude performance of reliable meta-analyses in all cases except for two trials comparing melatonin to placebo with similar methods for evaluating sleep efficiency. An apparent reduction in sleep latency with pharmacotherapy when compared to placebo or no treatment has been demonstrated although not consistently across all studies evaluating this metric. Sleep efficiency and sleep fragmentation were not shown to be improved by pharmacological therapy when compared to placebo or no treatment. This is in keeping with expert opinion that pharmacological agents, while somewhat effective for sleep onset insomnia, are ineffective for maintaining sleep.42
Furthermore, sleep architecture in hospital, as measured by polysomnography, is dominated by stage N1 and N2 sleep. Restorative N3 sleep or REM sleep was found to be rare regardless of pharmacological intervention. When sleep is highly fragmented, it is common to observe a predominance of N1 sleep, as an arousal in an epoch of sleep on the EEG results in the sleep stage being scored back to stage N1.43 Stage N3 sleep was observed only in a single study, in patients receiving continuous or intermittently administered lorazepam.33 A paucity of N3 sleep is not unusual in middle-aged or elderly populations, where N3 typically constitutes only 5–10% of sleep.44 Furthermore, the sleep stages are influenced by the medications studied. Benzodiazepines, for example, are potent suppressors of N3 sleep, and increase the presence of sleep spindles.45 Spindles are the hallmark of N2 sleep, so it is common to see increased N2 sleep and decreased N3 sleep with benzodiazepines. Concurrent opioids will also decrease N3 sleep.46 The large percentage of N3 sleep seen in the study in which lorazepam was used is surprising given the intervention is known to suppress N3 sleep.33 Furthermore, this finding is not replicated in any other studies. A possible explanation is that N3 sleep is commonly overscored. REM sleep was only observed in four studies, independent of drug or placebo allocation. REM sleep can also be influenced by current and prior medications. There is evidence to suggest that benzodiazepines decrease REM sleep.47 Sleep stage distribution is also influenced by prior sleep episodes and medications. For example, recent sleep deprivation will increase N3 sleep and REM sleep.48 Lastly, recent medication use prior to the polysomnography recording may influence sleep stages (ie, recent discontinuation of REM-suppressant, such as a barbiturate, antidepressant or alcohol, will result in REM rebound). In summary, the disappointing performance of the sedatives in effecting greater amounts of N3 and REM is in part due to the well-known effect of these drugs on sleep stages. In addition, the medications administered and discontinued, as well as prior sleep during the run-in period, can influence sleep architecture, and although some of the trials were randomised, it is possible that these factors could be confounding the results given the small sample sizes. It is also important to recognise that while medication may influence the quality of sleep in hospital, severity of illness and environmental factors are important confounders. Severity of illness among patients included in this review ranged from critical illness requiring mechanical ventilation to admissions for elective surgery. Severity of illness was not described in some studies. Although our study selection strategy was designed to identify acutely ill adults, their variability in severity of illness within this group is still large. Furthermore, most studies did not describe the presence, or evaluate the impact, of environmental factors such as noise, light and interruptions to provide care that contribute to insomnia in hospital. Attempts to minimise or standardise the influence of environmental factors (ie, use of earplugs or eye covers, ‘quiet times’ in the unit) were not documented or, perhaps, attempted. Given the results of our review and others of non-pharmacological interventions, a multimodal approach that involves minimisation of environmental factors, pharmacotherapy and treatment of the underlying disease would be worthy of future study.
The lack of high-quality randomised controlled trials is one of the limitations of this review. The diversity of outcome reporting and the high degree of methodological heterogeneity prevented statistical pooling of the results in almost all circumstances. Major sources of clinical heterogeneity included large variability in drug dosing (ie, oxazepam dosing ranged from 15 to 50 mg per dose), severity of illness in hospital and the method by which sleep was evaluated. Only 6 of the 15 studies included used polysomnography which is considered the gold standard for sleep evaluation. Only two of these were randomised controlled trials, which speaks to the practical difficulty in using polysomnography in large trials and sick patients. In fact, 28 potentially eligible trials were excluded at second-level screening because the sole measure of sleep outcomes relied on patient self-reporting. We elected to exclude these studies as self-reporting has been demonstrated to correlate poorly with objective assessments and is associated with systematic bias.14 Furthermore, the general lack of safety outcome reporting does not allow a thorough evaluation of risk. Given paucity of convincing efficacy data, the relatively high potential for adverse events with these classes of drugs and the vulnerability of the population being studied future studies must systematically evaluate risk in order for clinicians to adequately assess the risk/benefit relationship of these interventions. Language restriction to English and French may also be considered a limitation although others have shown that this restriction may have little to no impact on findings.16
It is also important to recognise the paucity of placebo-controlled trials in this setting. An evidence-based approach to clinical trial design would suggest that placebo-controlled trials that evaluate the efficacy of drug therapies be conducted in advance of comparative trials. While placebo-controlled trials are available in healthy volunteers and otherwise healthy community-based patients, the aetiology of sleep disturbances is not the same as that of the acutely ill patient sleeping in a hospital bed. Similarly, the outcomes of such trials cannot be extrapolated to this population either. Given that the majority of hospitalised patients receive pharmacological sleep aids in hospital in the absence of evidence to suggest that they are helpful and safe, well-designed trials are needed. Future studies must be randomised, employ a placebo arm, use standardised definitions of sleep-related outcomes and evaluate sleep using objective measures such as polysomnography.
Conclusions
While sleep is universally recognised as an essential body function to enable the restoration of physiological systems, sleep disturbances are common in hospitalised patients. A variety of pharmacological agents are used in the majority of these patients with the presumption that they improve the quality and quantity of sleep; however, this review suggests that the low-to-moderate quality evidence available does not support this notion. While drug therapy may be associated with falling asleep faster (although not consistently demonstrated), there is no evidence that drug therapy improves the more important outcomes of sleep efficiency or quality. This may be due to the fact that drug therapy is truly ineffective or that the quality of existing trials is inadequate to show a difference. It is evident that larger, better quality trials are needed to definitively answer this question. Future trials must use standardised definitions for sleep-related outcomes, objectives methods for measurement, a placebo arm and systematically evaluate risk. At this time, there is insufficient evidence to support the current usage of pharmacotherapy for the treatment of sleep disturbances among hospitalised adults.
Acknowledgments
The authors acknowledge Risa Shorr MLS, an information specialist, for her assistance in developing and validating our search strategy. The authors also acknowledge Dr Dean Fergusson for reviewing the manuscript.
References
Footnotes
SK and AM contributed equally to this work and would like to be recognised as coprimary authors.
Contributors All authors (SK, AM, BH, LB, ER, EM and VL) contributed to the study protocol. SK and AM were responsible for abstract screening, study selection and data extraction. BH, SK and AM performed the analysis and all authors contributed to the interpretation of results and writing of the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data were extracted from previously published papers which are referenced in the manuscript.