Article Text

Abstract
Objectives To evaluate the efficacy and safety of intra-articular (IA) bupivacaine administered for pain relief after joint arthroplasty.
Design Meta-analysis.
Methods A systematic review was conducted to identify the randomised controlled trials using IA bupivacaine for postoperative pain relief from MEDLINE, Cochrane Library and EMBASE databases (up to October 2015). The standardised mean difference (SMD), the relative risk (RR) and their corresponding 95% CIs were calculated using the RevMan statistical software.
Results A total of 11 randomised controlled trials were included. Statistically significant differences between IA bupivacaine and placebo were observed for the mean visual analogue scale (VAS) values (SMD −0.55; 95% CI −0.89 to −0.22; p<0.001) and narcotic consumption (SMD −0.32; 95% CI −0.55 to −0.08; p=0.008) during the period of 24 hours postoperatively and narcotic consumption during the period between 24 and 48 hours postoperatively (SMD −0.32; 95% CI −0.55 to −0.08; p=0.009). However, there was no significant difference in the mean VAS pain score during the period between 24 and 48 hours postoperatively (SMD −0.09, 95% CI −0.30 to 0.11; p=0.37) and in the incidence of adverse effects 24–72 hours postoperatively (RR 0.97; 95% CI 0.60 to 1.57; p=0.91).
Conclusions The administration of IA bupivacaine after joint arthroplasty is effective for pain relief without increasing adverse effects.
- PAIN MANAGEMENT
- Analgesics
- Intra-articular
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first meta-analysis that examined the efficacy and safety of intra-articular (IA) bupivacaine versus placebo after joint arthroplasty.
All included studies adopted the randomised placebo-controlled design.
The findings provide comprehensive conclusions on the effects of IA bupivacaine after joint arthroplasty.
Substantial heterogeneity was observed.
The included studies involved a wide variety of bupivacaine doses and anaesthetic techniques.
Introduction
Along with the ageing process and the development of medical technologies, joint arthroplasty has become one of the most common surgical procedures that can greatly improve the quality of patients' life by providing pain relief, functional improvement and deformity correction.1 ,2 The annual report of the National Joint Registry showed that the number of total hip arthroplasty (THA) and total knee arthroplasty (TKA) had reached 15 000 in 2011 in England and Wales;3 in the USA, patients receiving TKA had doubled between 1999 and 2008.4 However, this procedure is often accompanied with a variable degree of pain.5 The uncontrolled postoperative pain can result in a multitude of consequences, including decreased satisfaction of patients, delayed recovery with declined range of motion of the joint, prolonged hospital stay, as well as increased risk of thromboembolism.6 ,7 Therefore, aggressive pain control during the early postoperative period is essential and various analgesic techniques can be used for pain management after joint arthroplasty,8 such as peripheral nerve blockade, epidural anaesthesia, local infiltration analgesia and narcotics. Among these techniques, the use of narcotics is the most popular one, but in association with multiple side effects, including respiratory depression, drowsiness, nausea and vomiting, pruritis, reduced gut motility, and urinary retention. Thus, it is of significant importance to develop an effective measure of pain management to mitigate both pain perception and narcotic usage without intensifying side effects.
Intra-articular (IA) injection of local analgesics is one of the most widely used pain control techniques due to its convenience of operation and practicality.9 The local anaesthetic is injected into the IA cavity after the surgical wound or joint capsule closure from where it can spread into the muscles and soft tissues, so as to relieve postoperative pain.10 Bupivacaine, the most common local anaesthetic used during orthopaedic surgery,11 is characterised by prolonged period of active effectiveness.12 However, some existing studies10 ,13–16 suggested that IA bupivacaine could generate a better pain relief effect and requires less narcotic usage than a placebo for joint arthroplasty, while some others17–22 failed to reach any positive results. Therefore, it is necessary to confirm whether IA injection of bupivacaine in joint arthroplasty is effective and safe. Thus, the objective of the present study is to evaluate the efficacy and safety of IA bupivacaine after joint arthroplasty by conducting a systematic review and meta-analysis of randomised placebo-controlled studies. It was hypothesised that IA injection of bupivacaine after joint arthroplasty could improve pain control and reduce narcotic usage without intensifying side effects.
Materials and methods
Search strategy
This systematic review and meta-analysis was conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.23 The MEDLINE/PubMed database, Cochrane Library and EMBASE database were searched to retrieve the relevant studies that compared bupivacaine with placebo for patients who received IA injection after joint arthroplasty from inception to October 2015. The search terms were ‘Arthroplasty’, ‘replacement’, ‘bupivacaine’ and ‘randomised controlled trials’. The specific search strategies were illustrated in the ‘ online supplementary appendix’. No restriction was imposed. The references and reviews of the retrieved studies were also assessed.
Supplementary appendix
Study selection
The articles retrieved from preliminary search were independently analysed by two reviewers (YC and TY), and the ones meeting the following criteria were included in the analysis: (1) joint arthroplasty procedure; (2) patients who received bupivacaine intra-articularly after the joint arthroplasty procedure; (3) placebo was administrated in the control group; (4) other analgesics were neither added in the experimental nor in the control group; (5) randomised controlled trials (RCTs) and (6) written in English. The exclusion criteria were as follows: (1) case reports, reviews, animal trials, in vitro studies, letters, retrospective studies and other non-RCTs; (2) no placebo control group; (3) additional analgesics were administered in either the experimental or the control group; (4) data were not available for meta-analysis and (5) non-English literature.
Data extraction
The available data and the quality of article were assessed by two reviewers independently (YC and TY). The following study characteristics were retained during the review: first author, year of publication, number of patients in each group, method of administration, volume of injected fluid, concentration of bupivacaine, epinephrine usage, intra-articular injection time, type of surgery and type of anaesthesia. If there were more than two groups in one study, data were only extracted from the bupivacaine and the placebo groups. The means and SDs were manually measured by using the GetData V.2.20 software if they were provided in figures (Website of GetData software. http://getdata-graph-digitizer.com/).
The primary outcome of our interests was the effects of intra-articular bupivacaine for postoperative pain control. The postoperative pain intensity was measured by the visual analogue scale (VAS). All VAS scores were converted to a scale ranging from 0 to 10. The secondary outcome of interests included the amount of narcotic consumption and the adverse reactions after operation. All kinds of narcotic consumptions, such as meperidine and hydromorphone, were converted into morphine equivalents for subsequent analysis15 ,19 ,21 ,22 (One study13 adopted a single-dose IA injection 24 hours after surgery, so this analysis considered the data of narcotic consumption at 24 hours after injection as the narcotic consumption for 24 hours postoperatively).
The two independent researchers (YC and TY) used a Cochrane's risk of bias tool to determine the methodological quality of the included studies. Seven types of potential risks of bias were evaluated: random sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment, incomplete outcome data, selective reporting and other biases. If the number of low risk of a study was more than four, it was considered to be a high-quality study, otherwise, a low-quality study. In order to improve the objectivity of the results, information including journal titles, authors, institutions and origins were concealed from the reviewers. Meanwhile, disagreements were resolved by discussion, and a third reviewer (CZ) was consulted if necessary.
Statistical analysis
The Review Manager V.5.2 software (RevMan V.5.2, The Cochrane Collaboration, Oxford, UK) was used for data analysis. For continuous outcome measures, postoperative pain intensity reporting on VAS and narcotic consumption after surgery, the standardised mean difference (SMD) was calculated with corresponding 95% CIs. Dichotomous data, the adverse effects, were displayed as relative risks (RR) and as their 95% CIs. Pain intensity was reported at different follow-up time points in the various studies, and some studies only provided the mean VAS pain score. In order to facilitate and standardise the pooling of data, the mean and SD of VAS scores for 24 hours and for 24 –48 hours postoperatively of each study were computed. Inverse variance was used as the statistical method to pool the results including VAS and narcotic consumption across all studies, while the pooling of results of adverse effects was carried out using the Mantel-Haenszel test. Studies not providing the data of incidence of adverse effects or the number of patients who suffered from adverse effects would be used for qualitative meta-analysis.
The homogeneity of effect size across trials was tested by Q statistic (p≤0.05 was considered heterogeneous). If significant heterogeneity was observed among studies, the random-effects model would be used, otherwise the fixed-effects model would be employed. We also examined the I2 statistic, which measures the percentage of the total variation across studies which results from heterogeneity rather than chance (I2≥50% was considered moderately or highly heterogeneous). Since the type of arthroplasty, the usage of epinephrine, the methodological quality of included studies and the time of bupivacaine injection were inconsistent among various studies, a sensitivity analysis was further conducted to explore the possible causes of heterogeneity and to examine the influence of various exclusion criteria (the factors aforementioned) on the overall risk estimate. Meanwhile, subgroup analyses based on different methods of administration (single-dose or continuous injection) were performed to evaluate the source of heterogeneity.
Begg's tests24 and funnel plots were used to assess publication bias. STATA V.12.0 (StataCorp LP, College Station, Texas, USA) was used to perform Begg's tests. The p<0.05 was considered to be statistically significant, unless otherwise stated.
Results
Characteristics of included studies
A total of 1567 articles were identified in the preliminary search. Thirty-one full texts were assessed and 11 articles10 ,13–15 ,17–22 ,25 were included in the final analysis (figure 1). All trials were placebo-controlled RCTs with a total of 866 patients (440 in the bupivacaine group and 426 in the control group). The overall characteristics of the 11 included studies are presented in table 1. The methodological quality of each trial is shown in figures 2 and 3. Three trials were judged to be low-quality studies.19 ,20 ,22
Characteristics of the included studies

Flow diagram of screened, excluded and analysed publications.
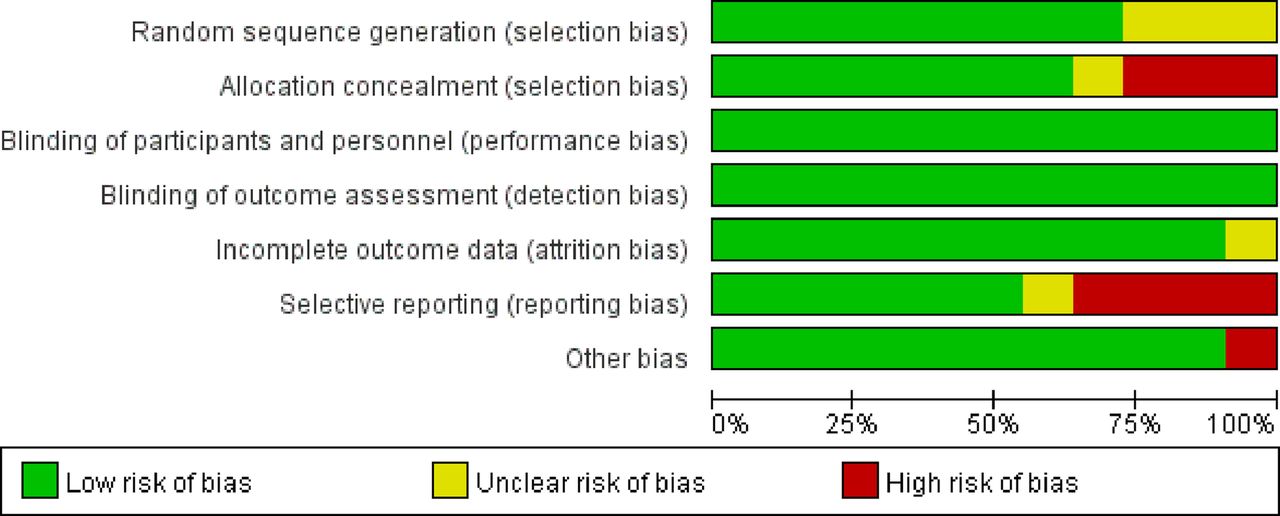
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
VAS values
Eight trials10 ,13 ,15 ,17 ,19–22 including data from 679 patients were eligible for the assessment of postoperative pain scores (VAS).
During the period of 24 hours postoperatively, data provided by eight studies10 ,13 ,15 ,17 ,19–22 were pooled and analysed by the random-effects model. Overall, the comparison between the bupivacaine and the placebo group showed that the mean VAS scores of bupivacaine was significantly lower (SMD −0.55; 95% CI −0.89 to −0.22; p<0.001). Substantial heterogeneity was observed (p<0.001; I2=75%). The results are presented in figure 4. Sensitivity analyses explored the potential sources of heterogeneity in the comparison between bupivacaine and placebo and investigated the influence of various exclusion criteria on the overall risk estimate. Table 2 demonstrates that the results were stable and reliable. Subgroup analyses of single-dose and continuous injection showed that IA bupivacaine was more effective than placebo in terms of pain relief (figure 4).
Sensitivity analyses

Forest plot of meta-analysis: mean VAS values of total and subgroup studies during the period of 24 hours postoperatively (0–10 points). VAS, visual analogue scale.
During the period between 24 and 48 hours postoperatively, the data provided by five studies15 ,17 ,19 ,21 ,26 were pooled and analysed by the fixed-effects model. Overall, there was no significant difference between bupivacaine and placebo in terms of pain relief (SMD −0.09, 95% CI −0.30 to 0.11; p=0.37), and no substantial heterogeneity was observed (p=0.45, I2=0%; figure 5). The sensitivity analyses which explored the influence of various exclusion criteria showed that the results were stable and reliable (table 2). Subgroup analyses of single-dose and continuous injection also showed no significant difference between bupivacaine and placebo in terms of the mean VAS scores (figure 5).
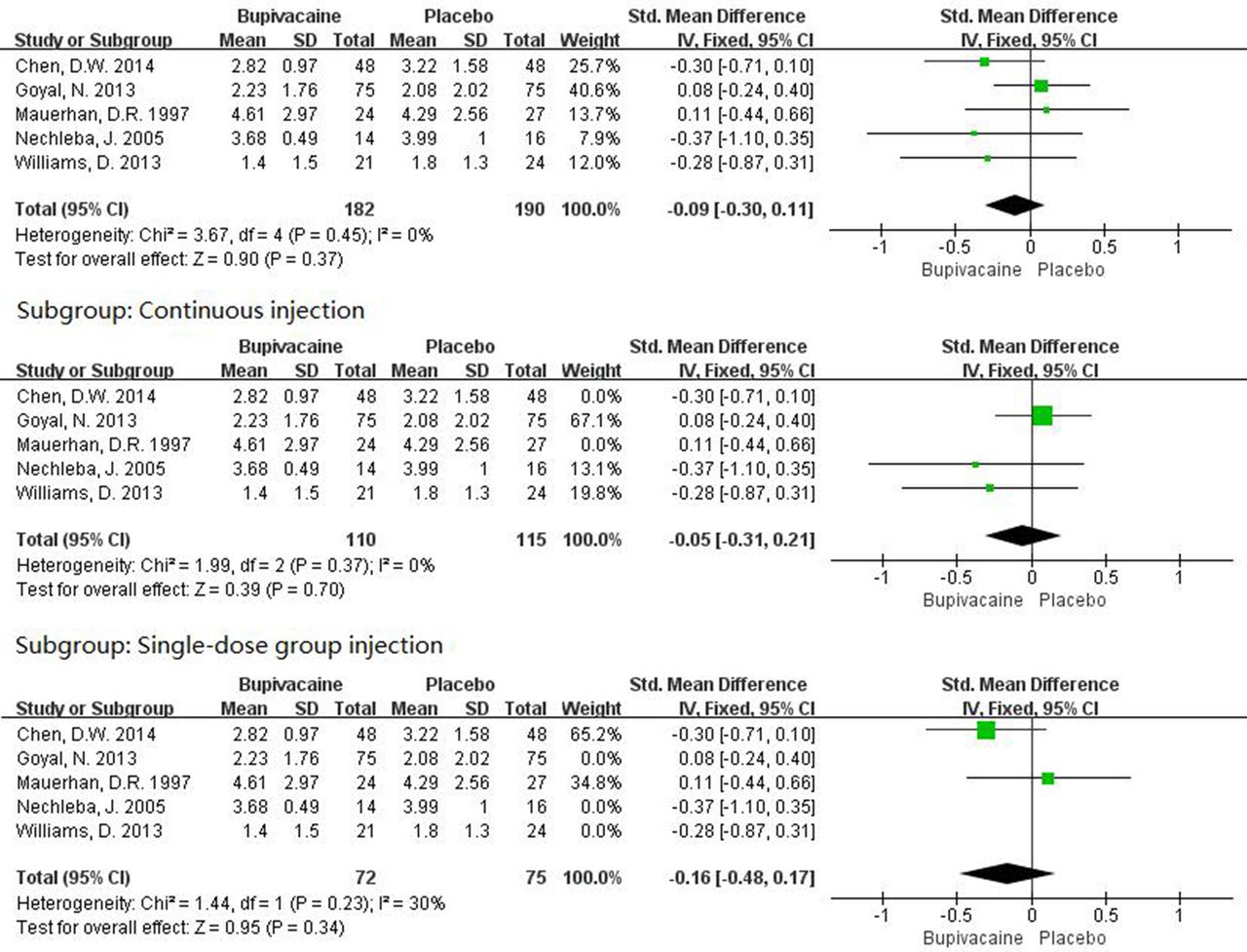
Forest plot of meta-analysis: mean VAS values of total and subgroup studies during the period between 24 and 48 hours postoperatively (0–10 points). VAS, visual analogue scale.
The funnel plot did not show any substantial asymmetry (figure 6). However, the power of this result may not be reliable because of the relatively small number of included studies. The Begg's rank correlation test did not indicate any publication bias among the included studies (p>0.05).
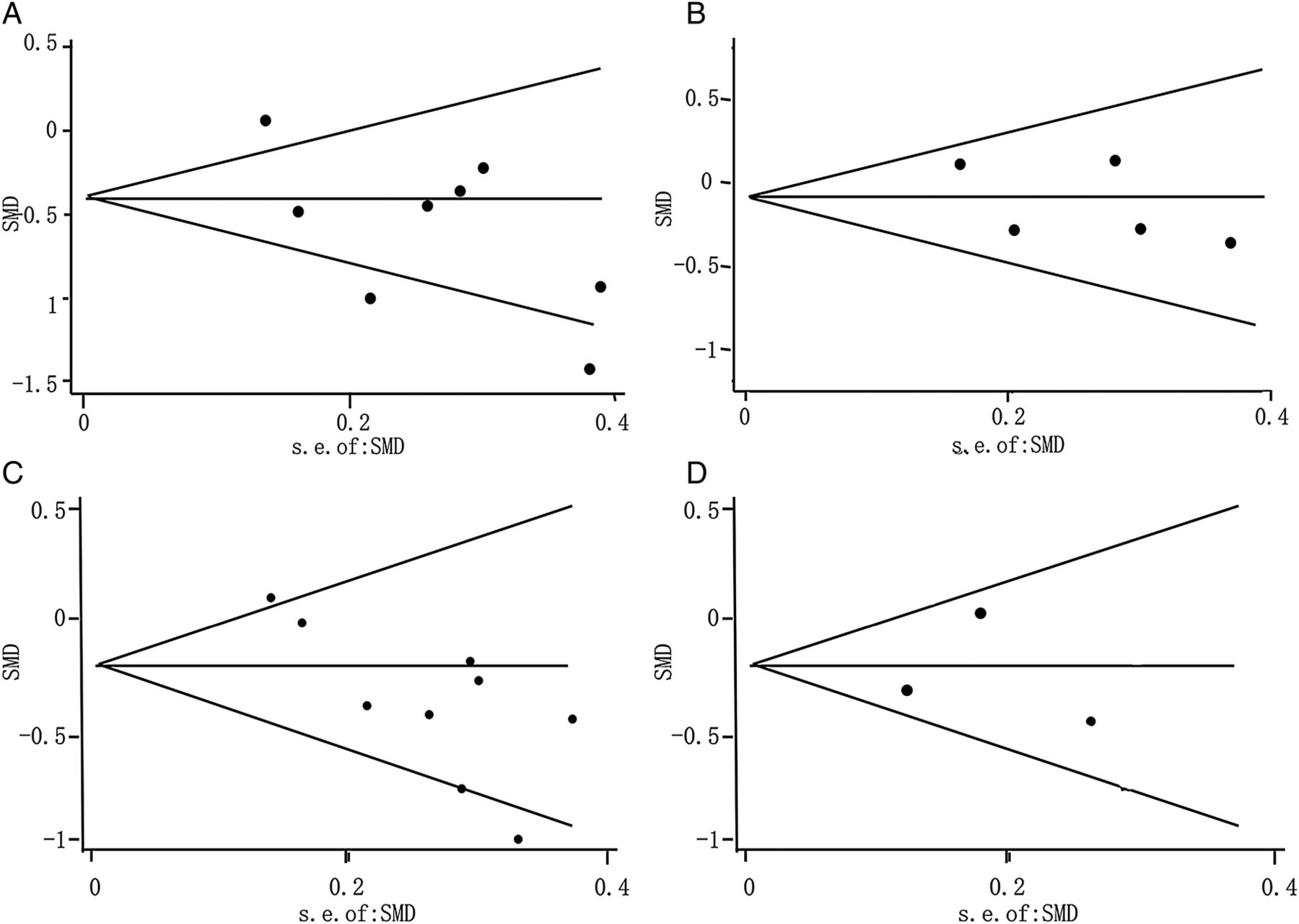
Funnel plot of meta-analysis: (A) Mean VAS values during the period of 24 hours postoperatively. (B) Mean VAS values during the period between 24 and 48 hours postoperatively. (C) Narcotic consumption during the period of 24 hours postoperatively. (D) Narcotic consumption during the period between 24 and 48 hours postoperatively. SMD, standardised mean difference; VAS, visual analogue scale.
Narcotic consumption
A total of nine studies14 ,15 ,17–22 ,25 reported narcotic consumption during the period of 24 hours postoperatively. The random-effects model was used for data analysis. Overall, narcotic consumption of the bupivacaine group was lower than that of the placebo group with statistical significance (SMD −0.32; 95% CI −0.55 to −0.08; p=0.008), meanwhile, significant heterogeneity was observed (I2=55%; p=0.02). The results are presented in figure 7. Sensitivity analyses which explored the influence of various exclusion criteria showed that the results were stable and reliable (table 2). Specifically, the substantial heterogeneity in narcotic consumption was materially changed by excluding the study involving an IA injection at 24 hours postoperatively (p=0.11; I2=40%). The single-dose injection subgroup showed a difference approaching to significance between the two groups in terms of narcotic consumption (p=0.06), while the continuous injection subgroup presented no significant difference between the two groups (figure 7).

Forest plot of meta-analysis: narcotic consumption of total and subgroup studies during the period of 24 hours postoperatively.
During the period between 24 and 48 hours postoperatively, the data provided by three studies15 ,17 ,18 were pooled. The fixed-effects model was employed for analysis. Overall, the narcotic consumption of the bupivacaine group was also lower than that of the placebo group with statistical significance (SMD −0.32; 95% CI −0.55 to −0.08; p=0.009), and no substantial heterogeneity was observed (p=0.45, I2=0%; figure 8).

Forest plot of meta-analysis: narcotic consumption during the period between 24 and 48 hours postoperatively.
The funnel plot did not show any substantial asymmetry (figure 6). However, the power of this result may not be reliable because of the relatively small number of included studies. The Begg's rank correlation test did not indicate any publication bias among the included studies (p>0.05).
Adverse events
A total number of seven articles13 ,15 ,17–19 ,22 ,25 reported side effects including nausea, vomiting, hypotension, urinary retention, sedation, pruritus and respiratory depression. Data from only five studies13 ,17–19 ,22 could be pooled. The random-effects model was used for analysis. There was no significant difference in terms of adverse effects between the IA bupivacaine group and the placebo group (RR 0.97; 95% CI 0.60 to 1.57; p=0.91; figure 9). Sensitivity analyses which explored the influence of various exclusion criteria showed that the results were stable and reliable (table 2). The funnel plot did not show any substantial asymmetry (figure 10). However, the power of this result may not be reliable because of the relatively small number of included studies. The Begg's rank correlation test did not indicate any publication bias among the included studies (p>0.05). In addition, another two studies,15 ,22 where the data were not available for quantitative meta-analysis, showed no significant difference in terms of the incidence of adverse events between the two groups.

Forest plot of meta-analysis: adverse effects.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of meta-analysis: adverse effects. RR, relative risk.
Discussion
This systematic review and meta-analysis of 11 RCTs was conducted to assess the efficacy and safety of IA bupivacaine after joint arthroplasty, in comparison with placebo. The most important findings were that IA bupivacaine was significantly better than placebo in relieving postoperative pain during the period of 24 hours postoperatively with less narcotic consumption and without intensifying side effects. However, for the VAS values during the period between 24 and 48 hours postoperatively, no statistically significant difference was observed.
The large, deep incision commonly used in joint arthroplasty can cause considerable surgical damage, and movement and reflex muscle spasms often exacerbate postoperative pain.27 Bupivacaine, an amide-based local anaesthetic, produces a blockade of peripheral nerves28 and is extensively applied in the management of pain after orthopaedic surgeries. Thus, the primary objective of the present systematic review and meta-analysis was to identify whether IA bupivacaine could provide a superior analgesic efficacy when compared with placebo. As a result, the bupivacaine group showed lower mean VAS scores and lower narcotic consumption during the period of 24 hours postoperatively, which was consistent with some previous findings.10 ,13–15 ,25 However, with respect to the comparison between bupivacaine and placebo, an opposite result was found in some other studies.17–22 A variety of factors may contribute to such conflict. Ruwe et al29 suggested that patients with preoperative pain were more likely to experience postoperative pain, so preoperative pain was regarded as a significant variable in their study. The small sample size of some studies may be another reason leading to inconsistent results. There was a trend towards increased narcotic usage and higher mean VAS scores in the control group, but no statistical significance was found in these two studies.17 ,18 On the other hand, the use of analgesia protocol for the experimental and control group in some studies may impact postoperative analgesia.30 The analgesia protocol was so strong that analgesia outcomes were not significantly improved by adding bupivacaine.17
During the period between 24 and 48 hours postoperatively, no significant difference was observed in terms of the mean VAS value between the two groups. Several researches31 ,32 showed that bupivacaine could yield analgesia of immediate onset but only for a short duration (2–4 hours). These pharmacokinetic data may partly explain why no significant mean VAS value was observed 24 hours postoperatively. Second, the mean VAS value during the period of 24–48 hours postoperatively was lower than that during the period of 24 hours postoperatively, and the pain may be quite weak in this period, making it difficult to demonstrate any difference between the two groups.33 However, the lower narcotic consumption during the period between 24 and 48 hours postoperatively can still demonstrate the pain relief effect of IA bupivacaine to some extent.
The present study also conducted two subgroup analyses: single-dose injection and continuous injection. The single-dose subgroup showed similar results, while the continuous subgroup showed a lower mean VAS value which was reliable with no heterogeneity (I2=0%) and no significant narcotic consumption during the period of 24 hours postoperatively. One possible explanation for such results might be that the sample size was too small to detect a statistical difference. Another reason was that the continuous infection of bupivacaine might need to be accumulated to a certain extent to show therapeutic effect. Thus, significant lower narcotic consumption was observed in the bupivacaine group during the period between 24 and 48 hours postoperatively. In addition, all of the included studies involving continuous injection did not conduct any negative control patient cohort without using infusion pumps. Therefore, the psychological impact on the perceived pain with the use of infusion pumps was not considered in this study. Alford and Fadale34 had demonstrated the placebo effect of using infusion pumps. It could partly explain the negative results obtained from the two groups where infusion pumps were used. However, Yamaguchi et al35 showed that the pain control infusion pump with a constant flow of local anaesthetics over a period of time could generate the benefit of prolonged analgesia with fewer adverse effects. Hence, further examination is needed to determine which method (single-dose injection or continuous injection) is better.
In the present systematic review and meta-analysis, seven included studies had reported the occurrence of adverse effects, and no significant difference was detected. However, Chen et al13 reported an opposite finding that the incidences of nausea and vomit were higher in the bupivacaine group compared with the control group. Interestingly, no bupivacaine was detected in the plasma of any patient taken at 2 hours after surgery in their study and the incidences of nausea and vomit were high in both groups. Therefore, this result might be caused by the reason that the analgesia protocol for both groups contained too much opioid.36 In order to minimise these side effects, the implementation of aggressive strategies could be proposed to prevent opioid side effects (eg, prophylacticantiemetic therapy).37 Since joint arthroplasty removes the whole articular cartilage, the chondrotoxic effects of bupivacaine38 ,39 do not need to be considered. In conclusion, the present study validated the safety of IA bupivacaine.
This study has several strengths. First, this is the first meta-analysis that examined the efficacy and safety of IA bupivacaine versus placebo after joint arthroplasty. It is more powerful than previous RCTs and reviews. Second, all the included studies adopted a randomised placebo-controlled design, which improved the comparability between the two groups and reduced the risk of selection bias. Third, this study provides a comprehensive report on the effects of IA bupivacaine after joint arthroplasty. Based on the pooled evidence from 11 RCTs conducted in a wide range of geographical locations, the findings of this meta-analysis can be generalised to a broader population with sufficient external validity, in view of the different patient characteristics, baseline illness statuses and ethnicities.
Several limitations of the present study should also be acknowledged. The primary one lies in the substantial heterogeneity across trials, even though this study explored the possible sources of inconsistency by conducting a series of sensitivity and subgroup analyses and identified some of these sources (the substantial heterogeneity in narcotic consumption was materially changed by excluding the study with IA injection at 24 hours postoperatively (p=0.11; I2=40%)). The second limitation is that the included studies involved a wide variety of bupivacaine doses and anaesthetic techniques. However, the effect of such heterogeneity may not impact the overall findings, as it was consistent between the two groups and the influence on analgesia was equal within any included RCTs. Third, the time of VAS value evaluation differed among the included studies, so the present study was forced to convert the data to mean VAS value during the period of 24 hours and during the period from 24 to 48 hours postoperatively to make the data suitable for pooling. It may impact the accuracy of the results. In addition, the time period to access adverse effects outcome also differed among the included studies, so it was impossible to group them into one time period. Fourth, the number of included studies for each outcome was <10 in this meta-analysis, so the power of the tests for funnel plot asymmetry may be too low to distinguish chance from real asymmetry. At last, the number of studies providing data of the VAS value and narcotic consumption during the period between 24 and 48 hours postoperatively and data of adverse effects is relatively small. Therefore, more high-quality RCTs are needed to verify our results.
Conclusion
The present study suggested that the administration of IA bupivacaine is effective for pain relief after joint arthroplasty without intensifying side effects.
References
Footnotes
YC and TY contributed equally and are the first authors of this article.
Contributors GL, YC and TY selected the studies. GL wrote the manuscript. YC and TY helped in writing the manuscript. CZ, JW, XX, LL, XD and YZ reviewed the manuscript. All authors contributed to the design of the study.
Funding This work was supported by Hunan Provincial Innovation Foundation For Postgraduate (CX2014A005), the Fundamental Research Funds for the Central Universities of Central South University, the National Natural Science Foundation of China (numbers 81201420, 81272034 and 81472130), the Scientific Research Project of the Development and Reform Commission of Hunan Province ((2013) 1199).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.