Article Text

Abstract
Objectives The objective of this study was to analyse how hospitalisation after the age of 60 affected individuals' health-related quality of life (HRQoL). The main hypothesis was that a hospital admission in old age can be seen as a proxy of ill health and possibly as a health divider, separating life into a healthy and an unhealthy part. The extent to which this is true depends on which disease individuals face and how functional ability and HRQoL are affected.
Settings This was a longitudinal study, based on an older cohort of individuals who participated in the Stockholm Public Health Cohort (SPHC) survey in 2006; the survey took place in Stockholm, Sweden. Information regarding hospitalisations and deaths, which is available through Swedish administrative registers, was linked to the survey from the National Patient Register and Cause of Death Register.
Participants 2101 individuals, 65+ years old at inclusion, with no previous hospitalisations at baseline (2006), were followed for 4 years until 2010 (end of follow-up).
Primary and secondary outcome measures HRQoL was assessed through a utility index derived from the EuroQol 5D questionnaire, at baseline and at 2010. The change in HRQoL after admission(s) to the hospital was estimated as the difference between the 2010 and 2006 levels using linear regression, also considering several covariates.
Results A single hospitalisation did not reduce individuals' HRQoL, either for men or women. On the other hand, multiple any-cause hospitalisations reduced HRQoL between 3.2% and 6.5%. When looking into hospitalisations for specific causes, such as hip fractures, a decrease in HRQoL was observed as well; however, conclusions regarding this were impeded by the small sample size.
Conclusions Hospital admissions in old age may indicate a shift from a healthy life to a life of compromised health when considering their frequency and cause over a period of time.
- quality of life
- EQ5D
- hospitalization
- morbidity
- Sweden
- older people
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We investigate how morbidity, measured through hospital admissions, has an impact on the health-related quality of life (HRQoL) in older age.
We follow a rather large sample (2101 individuals from the Stockholm Public Health Cohort), 65+ years old at inclusion, between 2006 and 2010.
HRQoL was measured using a utility index, derived from the EuroQol 5D (EQ5D) instrument.
Owing to data availability, HRQoL information was available only at two time points, in 2006 at the start of the study, and in 2010, at the end of follow-up.
Multimorbidity resulted in HRQoL deterioration, while only one hospitalisation was shown to possibly have a temporary effect, not leading to long-term HRQoL reduction.
Any-cause hospital admissions may be useful markers for the advent of a period of life with compromised quality of life; the number and frequency of hospitalisations, as well as their cause, could better determine the HRQoL outcome after morbidity.
Introduction
The health of the ageing population is an important focus of health policy, with geriatric medicine aiming to enhance the general well-being of the older people by postponing chronic diseases and mortality to later stages in life.1
From previous studies, we know that mortality rates have declined in all ages up to around 100 years, resulting in an extension of life expectancy among the older people. In addition, the age at which individuals face their first hospital admission after the age of 60 years has increased and incidence rates of important diseases have declined over time.2–6 This speaks in favour of improved health among the older people and raises a hospitalisation event to a potential health marker indicating a shift from healthy to sick life. However, the extent to which this is true depends on which disease individuals face, their medical history and how their everyday life is affected.
Health-related quality of life (HRQoL) is one useful measure focusing on individuals' physical, psychological and social aspects of living, as well as role functioning and activities of daily living.7 It represents the elements of life that are directly affected by morbidity, hence indicating whether a hospitalisation event representing morbidity in old age could be associated with the start of an unhealthy period of life. There are different instruments from which HRQoL can be inferred; one of the most frequently used instruments,8 which evaluates the health status of individuals and then converts it to an HRQoL measure, utility, is the EuroQol 5D (EQ5D) scale.9 This is a generic instrument and is suitable to be administered to older respondents,10 also with cognitive function limitations.11
This study looks into how the HRQoL of individuals aged 65–85 years is affected by the presence of morbidity, and whether this association varies by the number and cause of events, gender and age. Its aim was to establish whether a hospitalisation, used as a proxy for morbidity among the ageing population, could be considered as a marker for a shift from a life in full health into living with compromised health.
Material and methods
Study material
In 2006, individuals between ages 18 and 84 years, residing in Stockholm county in Sweden, were invited to participate in the Stockholm Public Health Cohort (SPHC) survey.12 For ages between 65 and 84 years, a specific questionnaire was sent out and 6713 responded (74.2%).12
Additional information was linked from national administrative registers to the survey data after informed consent was obtained from study participants; hospital admissions were collected from the National Patient Register.13 Death information was collected from the Cause of Death Register.14 The linkage was performed by Statistics Sweden using the unique personal identification number, each individual residing in Sweden has.
Baseline demographic characteristics and indicators of health status of individuals were collected for everyone answering the survey at baseline to determine whether any differences occurred among those who responded to the 2010 follow-up survey with respect to age, gender, educational level15 or health status (% of hospitalisations). Educational level was available from the Swedish registers, and was divided into three levels: basic (compulsory 9 years), secondary (12 years) and higher education.16 The maximum number of hospitalisation events, their cause, and the time since the last hospitalisation were based on information from the National Patient Register.13
HRQoL was assessed through the utility index; utility is a well-established proxy of the HRQoL of individuals.17 It is a number ranging between 1 (perfect health) and 0 (death/health state with very poor quality of life); it was calculated using a preference-based instrument that measures the health status of individuals, the EuroQol 5D (EQ5D).9 EQ5D is a non-disease-specific instrument comprising the following five dimensions: mobility, self-care, usual activities, pain and anxiety/depression. Each question has three possible distinct responses: ‘no problems…’, ‘some problems…’, and ‘I am unable to…’. These five questions with their responses were included in the 2006 and 2010 SPHC surveys. Their combination with the three-level responses gives 243 possible health states, which were transformed into a utility value using special weights that are specific for the EQ5D health states and are derived from a normal population in the UK.18 In addition to the utility index, the five dimensions of EQ5D describing the health status of individuals were analysed separately in order to explore the association of the change in HRQoL with the change in the health status of individuals.
Setting
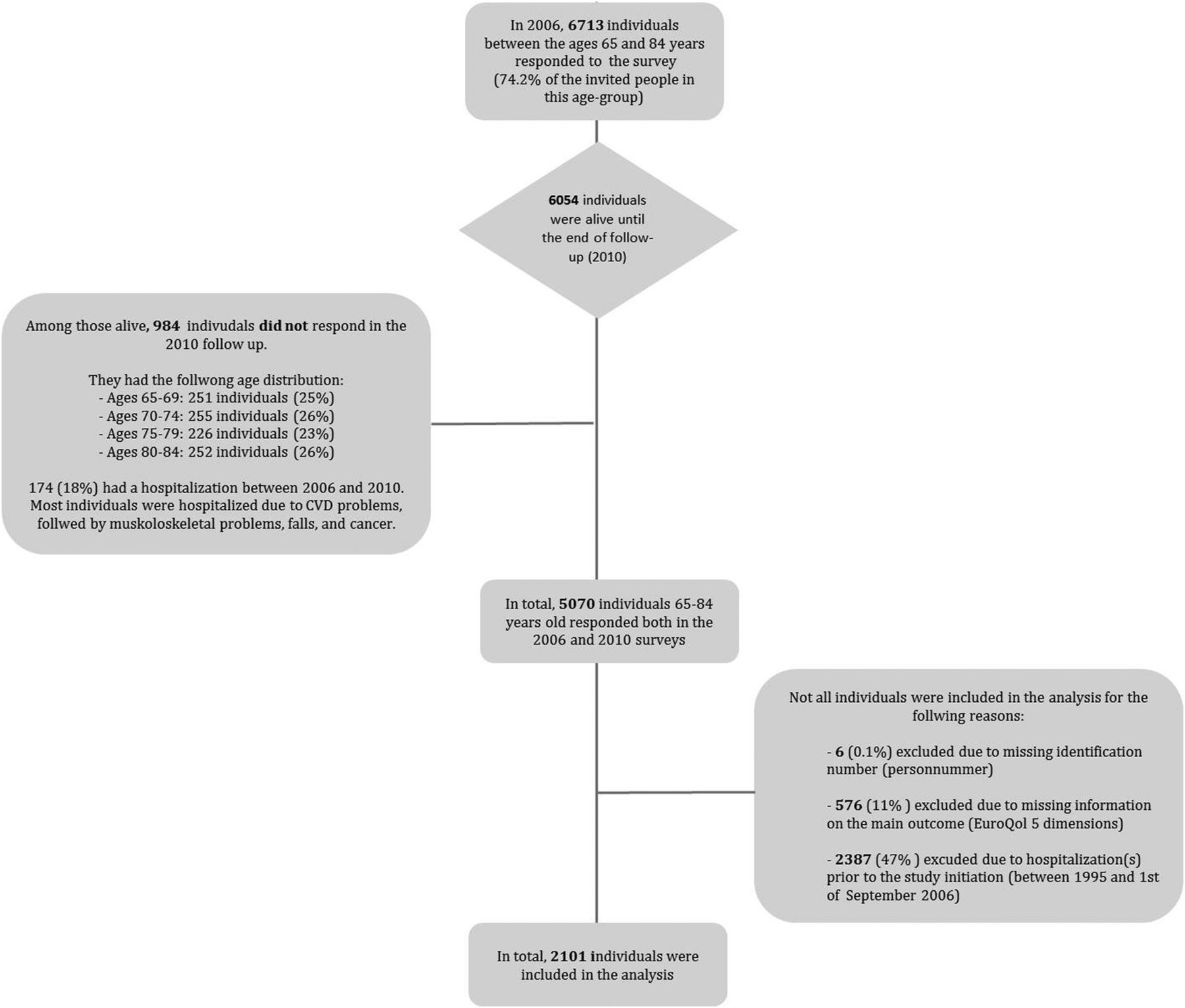
In figure 1, the study cohort and the number of study participants included in the analysis, as well as the numbers and reason for exclusion, are displayed. Of 6713 individuals who responded in the 2006 survey for the ages 65–84 years, 76% responded in the 2010 follow-up survey. Individuals with missing information on the EQ5D questions in 2006 or 2010 were excluded (n=576). In addition, individuals with hospitalisation(s) prior to study initiation (September 1, 2006) were excluded, to minimise the impact that already compromised health could have on the baseline utility measurement.

Flow chart of the study. CVD, cardiovascular disease.
Statistical analysis
The main outcome measure was the change in HRQoL, measured through utility, between 2006 (baseline) and 2010 (follow-up), based on one or subsequent hospitalisations. Utility was estimated for hospitalisations of any cause and for specific diagnoses, identified using the International Classification of Diseases (ICD), V.10: hip fractures (S72 excluding codes S72.3, S72.4 and S72.9), myocardial infarction (MI, I21 and I22), stroke (I60-I69), any cardiovascular disease (CVD, I00-I99) and any cancer (C00-C97). The minimum duration of hospitalisation was set to one night to exclude admissions to the hospital with no clinically proven illness.
The association between the change in utility and hospitalisations was first studied using descriptive statistics (bar charts). This analysis was stratified in four age groups: 65–69, 70–74, 75–79 and 80–84 years, and by gender. Then, each of the five dimensions of the EQ5D instrument, describing the utility index, was also linked with the presence of hospitalisations to determine which dimension was most likely associated with the change in utility after an admission to the hospital.
In addition, a linear regression model was used to measure the additional change in utility for hospitalised men and women, compared to non-hospitalised men and women, controlling also for covariates possibly influencing the crude associations. The covariates were: age, education, utility at baseline, maximum number of hospitalisation events and time since last hospitalisation.19 A forward stepwise approach was used to define the full model and the most relevant covariates; continuous variables in the linear regression were modelled by means of natural cubic splines.20
Sensitivity analysis
Analysis was conducted to determine whether the association between the change in utility and hospitalisations was influenced by the exclusion of individuals with a hospitalisation prior to 2006. Moreover, analyses were performed using another cohort within the SPHC, with a baseline at 2002 and a follow-up in 2010 to determine whether the follow-up time (4 years vs 8 years) would influence the study outcome. In addition, sensitivity analysis was conducted to estimate whether variability in the EQ5D measure would influence the association under study.
Results
In table 1 descriptive statistics of the 2101 individuals included in the analysis are presented. The majority were between the ages 65 and 69 years and had a secondary education. No statistically significant differences were observed in the number of hospitalisations between 2006 and 2010, or in the baseline utility, either between age groups or between gender; men: 0.854 baseline utility; women: 0.879 baseline utility.
Demographic characteristics of the study cohort
Change in utility between 2006 and 2010 for no, one, two and three/more hospital admissions of any cause is presented in figure 2 for men and women in different age groups. Results from the linear regression (crude and adjusted models) are presented in table 2. The covariates of the fully adjusted model and the graphs of the cubic splines are available on request.
Predicted change in utility from the linear regression, comparing individuals with and without any hospitalisation, for any-cause and disease-specific hospitalisations, by gender
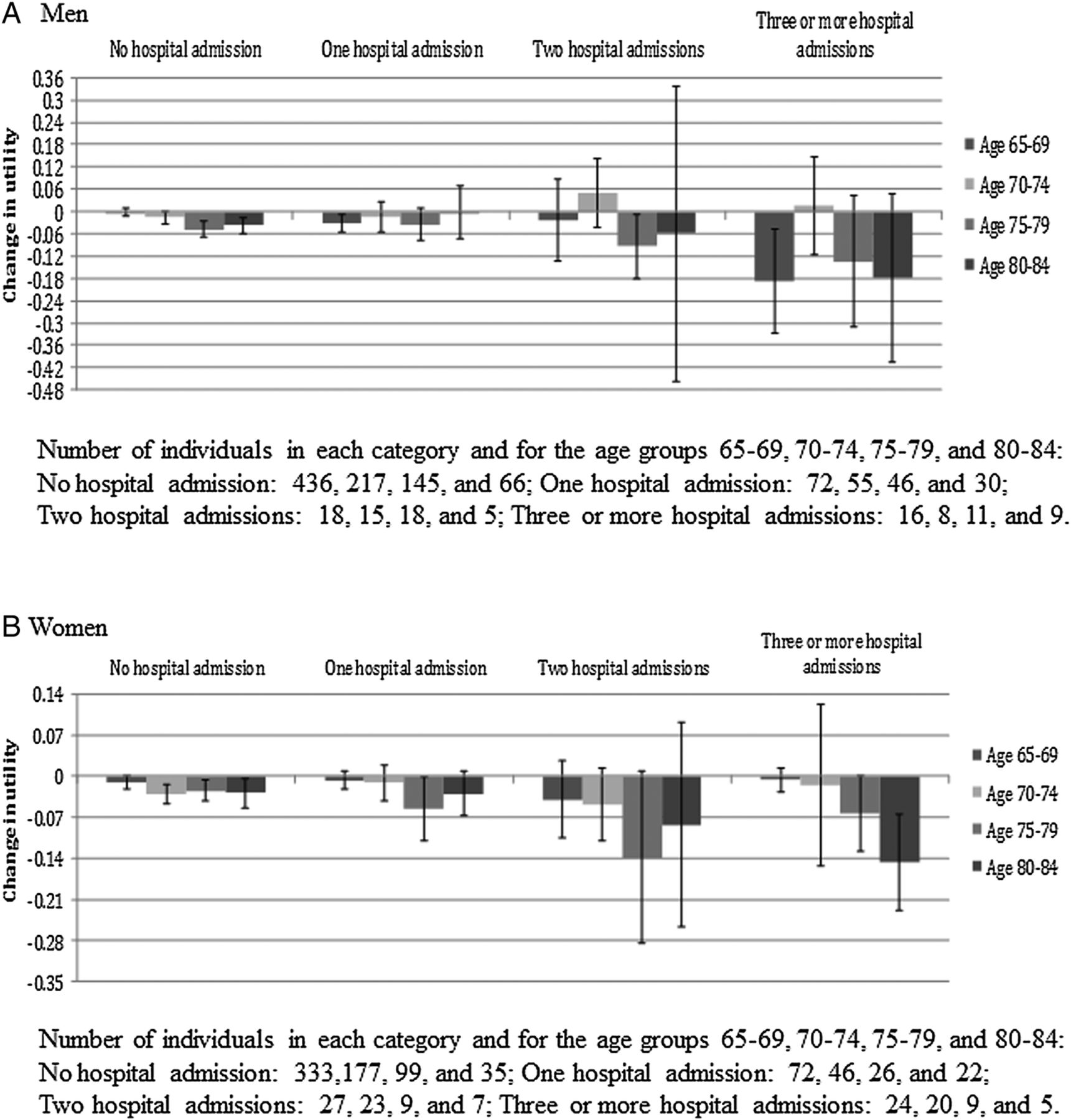
Change in utility, by hospitalisation status (any cause) and age group, for men and women separately.
A decrease in utility between 2006 and 2010 was observed for both hospitalised and non-hospitalised individuals (figure 2). Experiencing just one hospitalisation did not reduce the utility much for any of the age-groups, except for 65 to 69-year-old men and 75 to 79-year-old women. Among men, neither of the two hospitalisations had a clear impact on utility. However, women experiencing two hospitalisations had a higher utility reduction compared to women never hospitalised, or women with only one hospitalisation, especially among 75 to 79-year-olds. For both men and women, a clear effect of hospitalisation on utility was observed for three or more hospitalisations. Adjusting for age at start of the study, educational status, utility at baseline, maximum number of hospitalisation events and the time since the last hospitalisation in the linear regression, the additional utility decrease due to hospitalisations was 6.5% and 3.2% from baseline for men and women, respectively.
Looking into the utility dimensions and how each item contributed to the utility change after hospitalisation revealed that mobility problems had a slightly higher contribution, followed by pain, usual activities, anxiety/depression and self-care. The prevalence of severe mobility and self-care problems, as well as issues with usual activities, increased with the presence of multiple hospitalisations (data not shown but are available on request).
In figure 3, the change in utility, for men and women, after a hospitalisation for specific diseases is presented. No age stratification was possible due to the low sample size for some of the diseases. In table 2, the disease-specific estimates of the linear regression model are presented. A hip fracture hospitalisation resulted in a larger decrease in utility compared to the other diseases (MI, stroke, cancer and CVD; figure 3), however, the analyses were based on few events. MI, CVD and cancer were associated with 1.9% decrease in utility from baseline, compared to individuals non-hospitalised for these diseases. Again, the utility decrease could be explained mainly by the worsening of mobility and anxiety/depression problems.

{kind=link}
{kind=link}
{kind=link}
Change in utility, by hospitalisation status for specific diseases, compared to other and no hospitalisations, by gender. CVD, cardiovascular disease; MI, myocardial infraction.
Sensitivity analysis
The demographic characteristics of individuals not included in the analysis due to hospitalisation(s) prior to the 2006 survey did not differ significantly from those of the analysis sample. Their utility at baseline (2006) was on average lower compared to that of individuals included in the analysis, 0.845, 0.839, 0.836 and 0.799 for the age groups 65–69, 70–74, 75–79 and 80–84, respectively. For those excluded, the estimated additional utility decrease due to hospitalisation(s) between 2006 and 2010 was measured at −0.049 (95% Confidence Interval (CI): −0.088 to −0.009) for men and at −0.024 (95% CI −0.067 to −0.019) for women.
When using a different cohort, the 2002–2010 Stockholm Public Health cohort, and applying the same assumptions to conduct the analysis, no evident changes were noted for neither the demographic characteristics of the cohort nor for the conclusions drawn from the analysis (data not shown but available on request).
Discussion
This study explored to what extent hospitalisation(s) could be considered a potential marker for a shift from healthy life to a life with impaired health by quantifying the change in the HRQoL of individuals, measured using a utility index.
The initial HRQoL of all individuals was measured at the beginning of the study, in 2006, when participants were morbidity-free. During the 4-year follow-up, multiple hospitalisations were shown to affect individuals' HRQoL; the reduction varied nonlinearly, depending on the age group and gender, with older men and women experiencing a higher utility reduction. Looking into specific diagnoses, the decrease was more pronounced for hip fractures, even though no conclusions could be drawn from this association due to the few hip fracture cases observed during the study period.
No significant decrease in HRQoL was observed among those hospitalised one time, compared to those not hospitalised, which is in line with our previous studies where we have observed that there was no significant accumulation of long-term frailty after one hospitalisation; a decreased risk for subsequent hospitalisations was found in the ageing population over the years.3 Improvements in the efficiency of healthcare over time in Sweden could perhaps partly explain why no accumulation of long-term frailty after one hospitalisation was observed.
Since the change of the utility index, which was used as a proxy for HRQoL is difficult to interpret, it is helpful to look into the impact hospitalisations had on the five health dimensions comprising the utility index. This analysis revealed that the increase in moderate, and in cases severe, mobility problems, followed by increase in moderate and severe self-care, usual activities, pain and anxiety/depression problems, contributed to the decrease in HRQoL.
Our findings about the decline in HRQoL after morbidity can be confirmed when synthesising information from previously published literature. In a study conducted in Gothenburg, Sweden, HRQoL was found to decrease with the presence of two or more health conditions commonly present among 77-year-olds.21 Another study involving 85-year-old individuals residing in Linköping, Sweden revealed that those hospitalised at least one time 12 months prior to the study had more problems with mobility, self-care, usual activities and pain compared to those not hospitalised.22 The presence of prominent diseases among the older people, such as angina pectoris, hypertension, neck/shoulder/low back pain, was also found to impact the reported HRQoL in a study conducted in Stockholm county in Sweden.7
The decrease in HRQoL that we observed over the 4-year period (6.5% decrease for men and 3.2% for women; see table 2 for disease-specific events), associated with any-cause and disease-specific hospitalisation(s), was lower compared to the HRQoL decrease due to a cardiovascular event that another study in Sweden has found (annual decrease of 9.8%—no gender stratification available).23 That study, however, was based on individuals who already had cardiovascular problems, whereas in our analysis individuals were morbidity-free at baseline. This could explain the difference in the findings.
In general, the small decrease in HRQoL that is observed with only 1 or in cases 2 hospitalisations in our study could be due to the low sensitivity of the measure of health we use, that is, hospitalisations do indeed capture morbidity cases, but morbidity may also occur without hospitalisation. In fact, when looking into one specific diagnosis, for example, hip fractures, the sensitivity increased and we were able to observe a larger HRQoL change due to hospitalisation(s).
In addition, even if our study and previous studies indicate that hospitalisations, at least multiple ones, are the entry point of a period of life with compromised HRQoL, the time since the last hospitalisation event was shown to have a negative correlation with the decrease in HRQoL. In other words, the longer the time since the last hospitalisation, the higher the recovery from morbidity; therefore, HRQoL is expected to increase again, showing in this way a lower change. Therefore, the HRQoL decrease associated with hospitalisation(s) from our study is expected to be lower compared to the 1-year HRQoL decrease indicated by Lindgren et al.23 Results from another study in the USA and Canada, in which the relation between a hospitalisation and HRQoL was examined in patients with atrial fibrillation using a similar methodology to our study, present an effect of the same magnitude with our findings regarding the impact of hospitalisation(s) on HRQoL.24
Strengths and limitations
To the best of our knowledge, this is the first study in Sweden that uses this methodology to connect recorded morbidity, measured by hospitalisations in older ages, with the change in HRQoL. Since the study examined whether a hospitalisation could be a marker of the beginning of a period of life with impaired health, the inverse association, that is, looking into the HRQoL levels of the population and predicting the risk of a hospitalisation, was not studied. Regardless of the direction of the association, a causal effect of hospitalisation(s) on HRQoL (and vice versa) would not be implied, mainly due to the nature of this association.
In this study, the change in HRQoL was estimated through a utility index, and was stratified in different age categories in a large population-based sample, allowing the generalisation of our findings to the older population in Sweden. Still, no measurements of HRQoL were available for the respondents who were severely ill at the start of the study and who did not survive until 2010, which is a limitation with regard to the possibility to generalise our findings to the very ill.
On the other hand, our choice to exclude individuals with hospitalisations prior to the study initiation resulted in a more homogeneous study base, strengthening the causal pathway between a hospitalisation and a decline of HRQoL; their reported HRQoL at the beginning of the study may have been influenced by the presence of the previous diseases/hospitalisation and thus violates the causal pathway of hospitalisation and change in HRQoL.
Another distinct advantage of our study is the use of national registers to obtain information regarding healthcare usage. Not relying on the study participants to recall past hospitalisation events eliminates the recall bias from our data, providing in this way reliable information regarding the year and the cause of morbidity.
In this study, it would be difficult to separate between-person age differences from within-person changes due to the high intravariability in the measures.25 ,26 However, in this study, no such approach was taken, but instead we modelled the effect of morbidity on HRQoL. Any intravariability in the HRQL measure should be similar in the two groups at baseline. We also performed a sensitivity analysis by investigating the same association in another cohort and the results were similar (data not shown but available on request).
Another limitation in this study is that we had a follow-up period of 4-year of HRQoL regardless of when the hospital admission occurred. An ideal situation would have been to have measurements of HRQoL with the same time interval after a hospital admission for all individuals and also at several time points. However, when any cause hospitalisations were considered, the sample was large enough to be able to adjust for the time since the hospital admission. At the same time, it is expected that HRQoL decreases directly after a hospital admission and it was not primarily this effect that we wanted to capture in this study, rather the long-term effect in order to evaluate to what extent life after a hospital admission could be considered healthy or not.
Finally, in this study, we used a common and multiply validated, questionnaire to describe the health status of individuals and estimate the utility index, which represents the HRQoL of the respondents. EQ5D is a generic instrument that is shown to be sensitive to capture change in many diseases,8 among the older population as well,11 and can be used as a predictor of morbidity and mortality.27 However, it is constructed to capture pertaining disability, but not periodically. The period individuals reported their discomfort, pain, mobility and mental health problems was for ‘the past week’. Therefore, the hospitalisations that would lead to long-term disability would be stronger associated with a change in utility, and therefore HRQoL, compared to those where the disability is only temporary. This is seen in our study by the fact that being hospitalised for a hip fracture results in a larger decline in HRQoL than, for example, a myocardial infarction. It was also confirmed by a previous Swedish study, conducted in 1997 in Göteborg, Sweden, where they found that HRQoL, especially the emotional and social dimensions, was not much influenced by morbidity until individuals accumulated a significant amount of disability.21
Conclusions
HRQoL among those 65 years and older in Sweden was not affected by one hospital admission. Multiple hospital admissions, mirroring an accumulation of health problems, and hospitalisations for specific diagnosis resulted in a decline in HRQoL of 3.2–6.5%. Therefore, hospital admissions in old age may indicate a shift from a healthy life into a life of comprised health when considering their frequency and cause over a period of time.
References
Footnotes
Contributors KK, PF, AA and KM, were involved in the conception and design of the study. KK and PF performed the analysis of the data. KK, PF, AA and KM were involved in the interpretation of the results. KK and KM drafted the manuscript and all authors (including KK and KM) contributed with critical revisions to the contents of the manuscript. The final version of the manuscript was approved by all authors.
Funding Received from the Swedish Research Council for Health, Working Life and Social Research (Forskningsrådet för hälsa, arbetsliv och välfärd, FORTE) (grant number: 2011–0843), and the Swedish Society of Medicine (Svenska Läkaresällskapet).
Competing interests None declared.
Ethics approval Ethics approval for this study was obtained from the Regional Ethics Committee in Stockholm, Dnr 2011/136–31/5.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.