Article Text

Abstract
Introduction Physical inactivity has been described as a global pandemic. Interventions aimed at developing skills in lifelong physical activities may provide the foundation for an active lifestyle into adulthood. In general, school-based physical activity interventions targeting adolescents have produced modest results and few have been designed to be ‘scaled-up’ and disseminated. This study aims to: (1) assess the effectiveness of two physical activity promotion programmes (ie, NEAT and ATLAS) that have been modified for scalability; and (2) evaluate the dissemination of these programmes throughout government funded secondary schools.
Methods and analysis The study will be conducted in two phases. In the first phase (cluster randomised controlled trial), 16 schools will be randomly allocated to the intervention or a usual care control condition. In the second phase, the Reach, Effectiveness, Adoption, Implementation and Maintenance (Re-AIM) framework will be used to guide the design and evaluation of programme dissemination throughout New South Wales (NSW), Australia. In both phases, teachers will be trained to deliver the NEAT and ATLAS programmes, which will include: (1) interactive student seminars; (2) structured physical activity programmes; (3) lunch-time fitness sessions; and (4) web-based smartphone apps. In the cluster RCT, study outcomes will be assessed at baseline, 6 months (primary end point) and 12-months. Muscular fitness will be the primary outcome and secondary outcomes will include: objectively measured body composition, cardiorespiratory fitness, flexibility, resistance training skill competency, physical activity, self-reported recreational screen-time, sleep, sugar-sweetened beverage and junk food snack consumption, self-esteem and well-being.
Ethics and dissemination This study has received approval from the University of Newcastle (H-2014-0312) and the NSW Department of Education (SERAP: 2012121) human research ethics committees. This study is funded by the Australian Research Council (FT140100399) and the NSW Department of Education.
Trial registration number ACTRN12615000360516; Pre-results.
- Physical fitness
- Adolescents
- Physical activity
- Behaviour change
- Resistance Training
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Strengths of the present study include the randomised controlled trial design, relatively large sample size and use of objective measures of health-related fitness and physical activity.
In addition, our study will utilise a range of implementation strategies to support intervention fidelity and detailed process data will be collected to help explain study findings.
Despite these strengths, it is important to acknowledge some limitations. First, the study duration is relatively brief. This decision was made pragmatically, as process data from our previous trials indicated that students and teachers preferred a 10-week programme format.
Finally, a more direct measure of body composition (ie, DEXA) would have been preferable to the use of body mass index for assessment of this health-related fitness component.
Introduction
Physical inactivity has been described as a global pandemic with far reaching health, social, economic and environmental implications.1 Importantly, regular participation in moderate-to-vigorous intensity physical activity (MVPA) is critical for maintaining and improving health-related fitness (ie, body composition, cardiorespiratory fitness, muscular strength and endurance, and flexibility),2 which is an important predictor of current and future health status.3 ,4 Yet, 80% of adolescents worldwide are failing to achieve the amount of physical activity needed to enhance health-related fitness.5 Of concern, there have been global secular declines in cardiorespiratory6 and muscular fitness7–9 among young people, which have coincided with a rise in youth obesity.10 Although the importance of cardiorespiratory fitness11 and a healthy body composition12 have been established for some time, recent evidence has demonstrated the unique health benefits of achieving and maintaining adequate muscular fitness.13 Consequently, a recommendation to participate in ‘muscle strengthening’ physical activity (eg, resistance training) now appears in youth physical activity guidelines in a number of countries.14–17
Schools are ideally placed to promote health-related fitness and physical activity in adolescent populations, as young people spend 6–7 h per day for 40 weeks of the year in schools, most of which have the facilities, equipment, qualified staff and curriculum to deliver health promotion interventions.18 Indeed, these settings have the potential to help students meet the recommended 60 min of daily MVPA and develop the knowledge, skills and confidence to be physically active into the future.18 ,19 However, schools are less likely to prepare young people for a lifetime of physical activity if their focus remains solely on traditional, competitive team sports and games.20 ,21 Such activities may be enjoyable for some and are indeed an effective way for young people to engage in MVPA, particularly for those with the requisite level of skill competency to be successful. However, team sports and games may not have strong carry over effects into adulthood, as many young people drop out of sport during adolescence.22 ,23 Moreover, adolescents have identified a desire to try a variety of non-traditional activities, including weight training and fitness classes.24 Considering the lack of emphasis on alternative physical activities within traditional physical education (PE) and school sport programmes,20 many young people may leave school ill-equipped to maintain a physically active lifestyle beyond the schooling years.
Lifelong physical activities “are typically performed individually or in small groups, involve minimal structure and minimal physical contact, are characterized by varying levels of intensity and competitiveness, and may be easily carried into adulthood and old age”.21 These activities can contribute substantially to adult physical activity. Indeed, health and fitness activities such as resistance training rank among the most popular sports and physical activities regularly performed by western adults.25 ,26 Although these activities are popular in relative terms, the overall prevalence of participation remains quite low. For example, just one in five adults in the USA report ‘exercising with equipment’27 and only 17% of Australian26 and 14% of English25 adults regularly engage in ‘fitness/gym’ and ‘health and fitness’ activities, respectively. Clearly, for some, health and fitness activities can form an integral part of an active lifestyle during adulthood. However, in addition to common barriers such as time and cost, many adults may feel they lack the competence to participate in these activities effectively.28 ,29 Given the capacity for schools to provide students with the skills and confidence to engage in lifelong physical activities,24 there is a clear rationale for school-based interventions that address adolescents' current and future physical activity needs.
Despite the potential for schools to influence students' health behaviours, previous school-based physical activity interventions have had mixed success and a number of limitations have emerged in the literature.30 ,31 First, few interventions have included strategies and components designed to promote muscular fitness, as recommended in national physical activity guidelines. Second, previous interventions have often been developed for ‘all’ students using a ‘one size fits all’ approach, regardless of their age and sex. Sex has emerged as a consistent moderator of school-based interventions, suggesting that subgroups such as males and females may benefit from different intervention strategies and sociocultural intervention tailoring.32 ,33 Third, previous interventions have often failed to include implementation strategies, which may contribute to poor intervention fidelity and null findings.34 Finally, the majority of interventions have been evaluated in small-scale efficacy trials and very few have been designed to be ‘scaled-up’ and disseminated.
Schools can help address the global pandemic of physical inactivity by employing a multicomponent approach that includes quality PE, physical activity within and beyond the school day, staff involvement, as well as family and community engagement.18 ,35 Such an approach should include evidence-based programmes that can be implemented within an overall health promotion framework. The Nutrition and Enjoyable Activity for Teen Girls (NEAT)36–38 and the Active Teen Leaders Avoiding Screen-time (ATLAS)39 ,40 programmes were developed specifically to support school-based physical activity promotion and obesity prevention efforts for girls and boys, respectively. The NEAT and ATLAS programmes reduced screen-time37 ,40 and improved body composition,38 muscular fitness,38 ,40 resistance training skill competency,40 and well-being41 in low-active adolescents. However, similar to other school-based interventions, the original NEAT and ATLAS programmes included a large number of intervention strategies, making them difficult to implement more broadly without the ongoing support of the research team.42 Using process evaluation data40 ,43 and feedback from the New South Wales (NSW) Department of Education, the programmes were refined to allow for implementation in typical secondary school settings. Therefore, the aims of this two-phased study are to (1) determine the effectiveness of the revised NEAT and ATLAS programmes in 16 schools using a cluster randomised controlled trial (RCT); and (2) evaluate the dissemination of these programmes throughout government-funded secondary schools in NSW, Australia over a 12-month period.
Methods
Study design
In the first phase of the study, the revised NEAT and ATLAS interventions will be evaluated using a cluster RCT. The intervention will target females and males in year 9 (third year of secondary school) in 16 coeducational, government-funded secondary schools in NSW Australia. Assessments will be conducted at baseline (April/June, 2015) and will be repeated postintervention at 6 months (October/December, 2015) and again at 12-month follow-up (April/June, 2016). Muscular fitness (primary outcome) and other study outcomes will be assessed at baseline, 6 months (primary end point) and 12 months. In addition to these assessments, accelerometer-measured physical activity will be assessed at 3 months (mid-intervention) to determine the effect of the intervention on physical activity during programme implementation. The design, conduct and reporting of this RCT will adhere to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)44 and Consolidated Standards of Reporting Trials (CONSORT) guidelines.45 Schools will be randomised to the NEAT and ATLAS intervention group or a wait-list control group for the 12-month study period. Schools in the control group will participate in usual practice (ie, regularly scheduled PE and co-curricular school sport) during the study period.
In the second phase of the study, the RE-AIM framework46 ,47 will be used to evaluate the dissemination of the interventions (ie, Reach into the student population, Effectiveness in changing student outcomes, Adoption based on teacher training and initiation of program delivery, Implementation fidelity, and Maintenance of student changes and program delivery beyond initial implementation). The research team will develop ‘train the trainer’ materials to enable dissemination of the NEAT and ATLAS interventions throughout government-funded secondary schools in NSW, Australia. The dissemination phase will not include a control group.
Sample size calculation
Sample size calculations have been based on estimated effect sizes for the primary outcome of muscular fitness assessed using the 90° push-up and standing long jump tests.48 Although the health benefits of muscular fitness are now well established,13 ,49 there is a lack of consensus regarding the clinical significance of changes in muscular fitness in young people. Based on our previous studies, we anticipate an effect size of d=0.4 for muscular fitness (adjusted between-group difference of ∼2 repetitions).40 ,50 In accordance with CONSORT guidelines,45 our power calculations were adjusted for the clustering of effects at the school level. We adjusted for clustering using a correction factor of [1+(m−1)×ICC], where m=participants per class and ICC=the intraclass correlation coefficient. Assuming an average class size of 20 participating students, two classes per school and an ICC for muscular fitness of 0.09,40 the correction factor is 2.7 (ie, 1+(20−1)×0.09). Allowing for an expected 10% loss to follow-up at 6 months and a further 10% loss at 12 months, the required sample size to achieve 80% power with α levels set at p<0.05 is 640 students from 16 schools (16 intervention classes and 16 control classes). The study will be adequately powered to detect significant between-group differences at the primary study end point (6 months) and at follow-up (12 months).
Setting and participants
The RCT will be conducted within 16 eligible government-funded secondary schools located within the Hunter, Central Coast and Sydney regions of NSW. To identify eligible schools, our research team will use the NSW Department of Education website ‘School Locator’ function to identify Government secondary schools within approximately 50 km of the University of Newcastle and the University of Sydney. Eligible participants will be adolescent males and females in year 9 attending 1 of the 16 recruited schools who do not have an injury or illness that would affect participation in a physical activity and resistance training programme. The programmes will be implemented within schools by members of the teaching staff at each school, who may be PE teachers or teachers of other subject areas. Female and male teachers will facilitate the NEAT and ATLAS programmes, respectively.
In the dissemination phase, all secondary schools in NSW will be eligible to participate and the programme will be open to students in years 9 and 10. The dissemination of the NEAT and ATLAS programmes will begin in October, 2015 (as requested by the department of education) and continue until October 2017. During this phase, the research team will aim to deliver two professional learning workshops per school term, resulting in a total of 16 workshops over the dissemination period. Overall, the research team will aim to recruit and train 240 teachers (ie, 15 teachers per workshop) to deliver the NEAT and/or ATLAS programmes in their schools.
Blinding and randomisation
In the cluster RCT, recruitment and baseline data collection will be conducted prior to randomisation, thereby concealing group allocation, and attempts will be made to blind research assistants to group allocation at the postintervention and follow-up time points (however, this is not always possible in school-based cluster RCTs). Following baseline data collection, schools will be match-paired based on size, geographical location and socioeconomic status (SES). Schools within each pair will then be randomised to either the intervention group or the wait-list control group by a researcher not involved in the current study using a computer-based random number producing algorithm. As such, schools randomised to the intervention condition will deliver both the ATLAS and NEAT programmes during the study period, whereas schools in the control condition will not deliver either programme until the completion of the 12-month study assessments. In the dissemination phase there will be no control group.
Intervention
Following the research evaluation of the NEAT36–38 and ATLAS39 ,40 programmes, the lead investigator was approached by the NSW Department of Education to develop a sustainable intervention model that could be disseminated across secondary schools in NSW. The Department of Education determined that the original NEAT and ATLAS programmes were too intensive and not sustainable without the support of the research team. Feedback from the Department of Education and examination of process evaluation data were used to guide the modification of intervention strategies. The following changes were made: (1) increased focus on resistance training (NEAT and ATLAS); (2) removal of nutrition workshops (NEAT), as these were considered too expensive and resource intensive; (3) removal of parent newsletters (NEAT/ATLAS) because they were not read extensively by parents/care givers; (4) text messaging strategy replaced with smartphone app (NEAT) to minimise cost; (5) removal of pedometer component (NEAT/ATLAS), as participant usage was low in NEAT and ATLAS; and (6) structured physical activity programme duration reduced to 10 weeks (NEAT/ATLAS) from 40 weeks (NEAT) and 20 weeks (ATLAS) to fit within one school term.
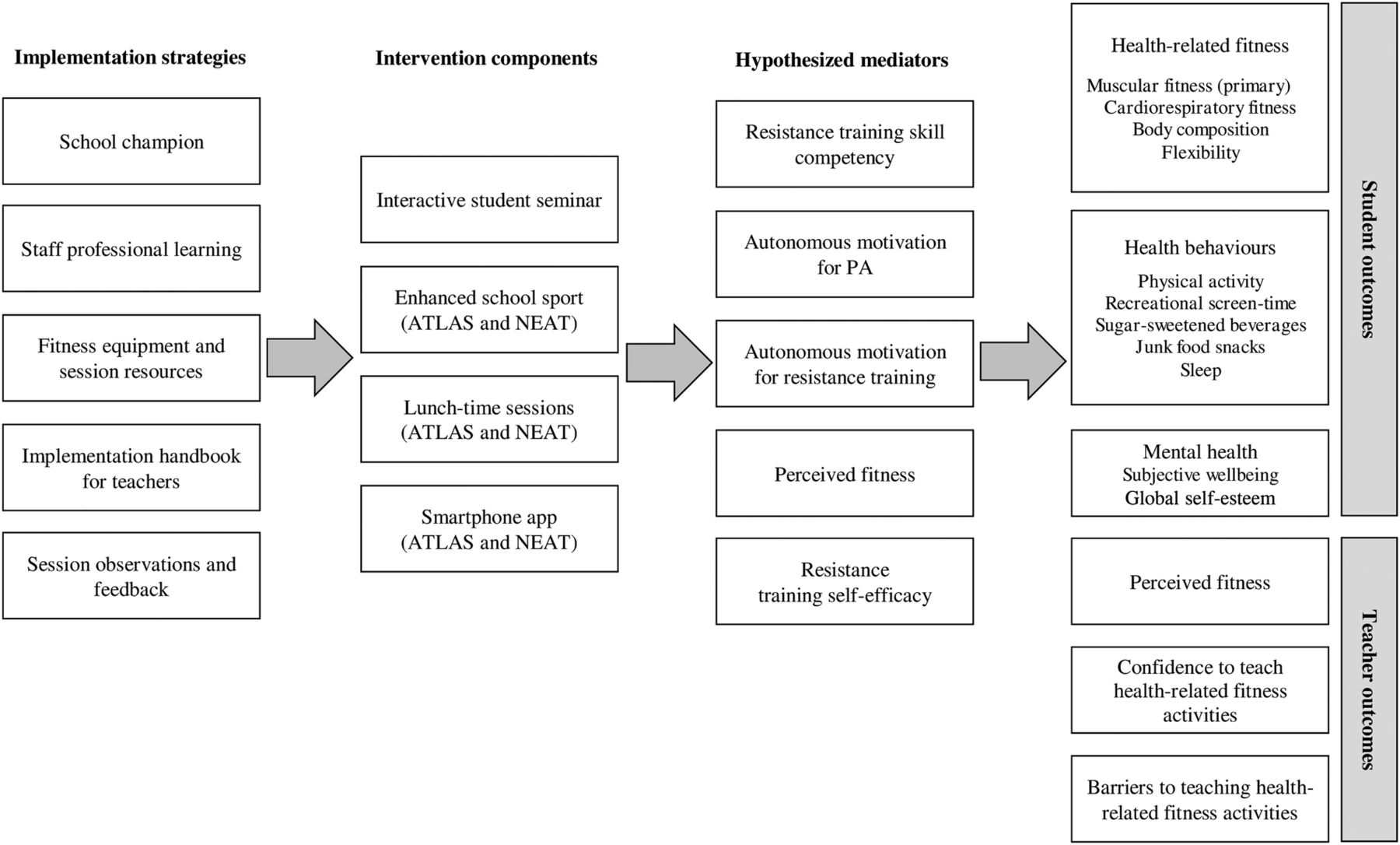
A summary of the revised NEAT and ATLAS implementation strategies and four gender-targeted intervention components is provided in figure 1. The following evidence-based implementation strategies will be used to ensure that the intervention is delivered as intended:51 (1) recruitment of school champions; (2) professional learning workshop for teachers; (3) provision of teacher handbook, session resources and fitness equipment; and (4) physical activity session observation and feedback. The intervention consists of the following components: (1) interactive student seminar; (2) structured physical activity programme; (3) lunch-time fitness sessions; and (4) web-based smartphone apps (separate apps for ATLAS and NEAT). Gender-targeted versions of the four intervention components were developed for girls (NEAT) and boys (ATLAS). A detailed description of the implementation strategies and intervention components for the NEAT and ATLAS programmes that will be delivered in the RCT and dissemination phases are provided in table 1.
Description and dose of implementation strategies and intervention components
{kind=link}
Implementation strategies, intervention components, hypothesised mediators and study outcomes. ATLAS, Active Teen Leaders Avoiding Screen-time; NEAT, Nutrition and Enjoyable Activity for Teens; PA, physical activity.
The NEAT and ATLAS interventions were guided by Social Cognitive Theory (SCT)52 and Self-Determination Theory (SDT).53 More specifically, the intervention was informed by the transcontextual model of motivation,54 which postulates that enhancing motivation for physical activity in one context (eg, PE) will promote motivation for physical activity in other contexts (eg, after school and on weekends).55 SDT has emerged as a popular and useful theoretical framework for modifying PE teachers' pedagogies and increasing adolescents' motivation for PE.56–59 In the current study, the teacher professional learning workshop will be used to provide teachers with strategies to satisfy students' basic psychological needs for autonomy (ie, sense of choice and volitional control), competence (ie, sense of mastery) and relatedness (ie, social connection with the teacher and fellow students).53 SDT will be operationalised using the ‘SAAFE’ (Supportive, Active, Autonomous, Fair and Enjoyable) teaching principles,60 which will be explained to teachers and reinforced using lesson observations and feedback. Consistent with SDT,53 satisfying these basic psychological needs should promote autonomous motivation for participating in health-related fitness activities. In regards to SCT, teachers will learn strategies for enhancing students' self-efficacy in resistance training and other health-related fitness activities (eg, providing encouragement, giving specific feedback on technique, modelling correct performance) and students will learn important behavioural skills such as physical activity self-monitoring and goal setting. These behavioural skills will be taught in the interactive seminar and embedded within the NEAT and ATLAS web-based apps.
The NEAT and ATLAS interventions include five evidence-based physical activity and nutrition messages, modified from the original interventions: (1) Move whenever you can; (2) Get some vigorous physical activity on most days; (3) Limit your recreational screen-time; (4) Avoid sugary drinks; and (5) Limit ‘sometimes’ foods. Although the messages are consistent for both adolescent girls (NEAT) and boys (ATLAS), they have been operationalised using a gender-targeted approach to enhance their relevance and salience. A range of sociocultural targeting strategies (surface and deep)33 ,62 were used to ensure that the NEAT and ATLAS interventions were appropriate for adolescent girls and boys (table 2). For example, the circuit cards and intervention resources featured pictures of young females (NEAT) and males (ATLAS). In addition, the content of the interactive seminars was designed to be relevant to boys and girls by recognising and focusing on established gender differences in specific health behaviours and motivational profiles. For example, research has shown that video gaming is typically a greater contributor to recreational screen-time for boys compared with girls, who tend to spend more time using social media.63
Sociocultural targeting strategies used in the NEAT and ATLAS cluster RCT
Study measures
In the cluster RCT, baseline, postintervention and follow-up assessments will be conducted by experienced research assistants and undergraduate student volunteers with a background in kinesiology or PE. To ensure consistency between assessors, a protocols booklet containing the instructions for each test was developed and will be used at all data collection periods. Prior to baseline, all assessors will attend a 2 h training workshop to familiarise them with the testing protocols. In the dissemination phase, the intensity of evaluation has been reduced due to the larger number and more distant schools that may participate.
Primary outcome (student)
Muscular fitness
Testing procedures and a demonstration from the assessor will be provided to participants prior to the conduct of the tests. Upper body muscular endurance will be assessed using the 90° push-up test.64 Consistent with the training principle of ‘specificity’, adaptions resulting from exercise will be specific to the type of training that is completed. As push-ups closely mirror one of the body weight exercises that will be delivered, this test is considered appropriate for evaluating changes in muscular fitness resulting from the intervention. In addition, this is a feasible field-based test that schools can use to evaluate programme effectiveness in the future, without the need for support from the research team. Using a cadence of 40 bpm (ie, one push-up every 3 s) participants lower themselves in a controlled manner from the start position until a 90° angle is formed at the elbow then push back up. The test concludes when participants either fail to maintain the movement with adequate form, fail to lower themselves to the required depth on three non-consecutive repetitions or on volitional failure. This test has acceptable test-retest reliability in adolescents (ICC (95% CI)=0.90 (0.80 to 0.95)).65 Lower body muscular strength will be assessed using the standing long jump test.66 Participants will begin with their toes behind a line marked at 0 cm and perform a maximal long jump, taking off and landing with two feet. The test will be performed twice, separated by a rest period of at least 15 s. The jump distance (in cm) will be recorded in line with the heel of the rearmost foot, with the longer of the two jumps recorded as the participant's final score. This test has been shown to be a valid and reliable method for assessing adolescents' lower body muscular strength.67
Secondary outcomes (student)
Body mass index
Height will be recorded using a portable stadiometer (Model no. PE087, Mentone Educational Centre, Australia) and weight will be measured using a portable digital scale (Model no. UC-321PC, A&D Company Ltd, Tokyo Japan). Body mass index (BMI) will be calculated using the standard equation (weight [kg]/height[m]2). Weight status will be determined according to age-specific and sex-specific BMI z-scores using the lambda-mu-sigma (LMS) method (International Obesity Task Force cut-offs).68
Cardiorespiratory fitness
Maximal aerobic capacity (ie, VO2 max) will be estimated using a submaximal step test protocol.69 Participants will be fitted with a heart rate monitor and asked to step up and down on a portable step (step height adjusted according to sex and standing height) for 3 min at a cadence of 88 bpm (ie, 22 ascents per minute). After 3 min, participants will be asked to stand still while their heart rate is recorded at 5, 10 and 15 s intervals. Recovery heart rate at 15 s will be calculated as the difference between the 15 and 5 s heart rate readings. Estimated VO2 max in mL/kg/min will be calculated using the regression equation reported by Francis and Feinstein.69 Using this approach, Francis and Feinstein reported a correlation coefficient of r=0.81 between estimated and actual VO2 max among a sample of 6–18-year-old youth.
Flexibility
Flexibility will be assessed using the FITNESSGRAM back-saver sit and reach test.64 Participants remove their shoes and sit with one leg extended against a portable trunk flexibility tester (Model no. PEO41, Sportime Ltd, Wisconsin, USA). Participants will be asked to extend forward as far as possible in a smooth and controlled manner whilst keeping the extended leg straight, head upright and palms facing downwards with fingers aligned. Participants will be instructed to gently push the measuring guide forward, pausing momentarily at the endpoint of the stretch. The measurement will be taken to the nearest 0.5 cm in line with the measurement guide and the test will then be repeated with the opposite leg extended.
Resistance training skill competency
Resistance training skill competency will be assessed using video analysis of the Resistance Training Skills Battery (RTSB).61 ,70 The RTSB includes six foundational RT movements completed in the following order: squat, push-up, lunge, overhead press (completed with 2 kg bar), front-support with chest touches, and suspended row. Each movement skill is performed twice (ie, two sets) for four repetitions and is scored by adding the total number of performance criteria (either four or five) successfully demonstrated during each set. The resulting skill score is therefore out of a possible 8 or 10, depending on the skill. An overall resistance training skill quotient is calculated by summing each of the six skill scores (possible range 0–56). Participants complete each exercise after viewing a standardised video demonstration of the skill pre-recorded on Apple iPads. The RTSB has demonstrated satisfactory construct validity, test-retest reliability (ICC (95% CI)=0.88 (0.80 to 0.93)),61 and interrater reliability70 in a sample of adolescents.
Physical activity
Stratified by school, a random subsample (50%) of students will wear GENEActiv wrist-worn accelerometers (Model GAT04, Activinsights Ltd, Cambridgeshire England). Participants will be instructed to wear the accelerometer continuously for seven consecutive days (even while sleeping, bathing and swimming). Valid wear-time will be classified as at least 10 h of data on at least 3 days. Mean weekday and weekend day MVPA will be determined using previously developed thresholds71 to classify physical activity into sedentary, light, moderate and vigorous intensity. In addition, all participants will be asked to self-report their total physical activity and participation in muscle strengthening physical activity using a validated measure.72 ,73
Recreational screen-time
A modified version of the Adolescent Sedentary Activity Questionnaire (ASAQ)39 ,74 will be used to determine time spent in screen-based recreation. The modified ASAQ addresses the issue of screen-multitasking75 by asking participants to report for each day of the week the ‘total time’ spent sitting using screens (of any kind) for the purposes of entertainment.
Sleep time and sleep quality
Sleep time and sleep quality will be assessed using items from the School Sleep Habits survey.76 Students will be asked to reflect on the past two weeks and report the ‘usual’ time they went to bed and the time they woke up on ‘school days’ and ‘weekends’ separately. School day and weekend day sleep onset latency (ie, the time taken to get to sleep) will be also assessed, with total sleep time calculated by subtracting the sleep onset latency from the total time between going to bed and waking. In addition, two items will be used to evaluate the quality of students' sleep (eg, How often do you think that you get enough sleep?). The Sleep Habits Survey has previously been validated against sleep diary report and actigraphy among adolescents.77
Sugar-sweetened beverage and junk food snack consumption
Two items from the NSW Schools Physical Activity and Nutrition Survey (SPANS)78 will be used to assess participants' regular intake of sugar-sweetened beverages (SSB's), which include fruit-based beverages (eg, orange juice), cordials, energy drinks and soft drinks (ie, soda). Consumption of junk food snacks (eg, biscuits, ice cream, cakes) will be assessed using a single item from the previously validated Australian Child and Adolescent Eating Survey.79
Global self-esteem
A five-item subscale from the Physical Self-Description Questionnaire (PSDQ) (short form)80 will be used to assess self-esteem. Students respond on a six-point scale (1=false, to 6=true) to how true each statement is for them (eg, overall, I have a lot to be proud of). The PSDQ has been validated previously.80
Psychological well-being
Diener et al81 psychological flourishing scale will be used to measure subjective well-being. Using a seven-point scale (1=strongly disagree, to 7=strongly agree), students respond to statements relating to indicators of ‘eudemonic’ well-being (eg, I lead a purposeful and meaningful life). Items in the scale are summed to create a composite well-being score (possible range 8–56). The validity of the measure has been established previously.81
Hypothesised mediators (student)
Autonomous motivation for physical activity
Autonomous motivation for physical activity will be assessed using the intrinsic and identified subscales from the Behavioural Regulations in Exercise Questionnaire-2 (BREQ-2).82 Students respond on a five-point scale to how true each statement is for them (1=Not true for me, to 5=Very true for me). Items are adapted to reflect participation in ‘physical activity’ rather than exercise specifically (eg, I value the benefits of physical activity). The factorial validity of the measure has been established previously.82
Motivation to participate in resistance training
To evaluate motivation for RT, an adapted version of the complete BREQ-2 will be used.82 Items are adapted to reflect participation specifically in resistance training (eg, I value the benefits of resistance training), rather than exercise more broadly. The complete BREQ-2 includes 19 items and five subscales corresponding to the motivational regulations outlined in SDT (ie, intrinsic motivation, identified regulation, introjected regulation, external regulation, and amotivation).
Perceived fitness
Perceived physical fitness will be self-reported using the International Fitness Scale (IFIS).83 The IFIS is a five-item instrument in which participants report perceptions of their ‘general fitness’ and four other specific fitness components (1=very poor, to 5=very good). The validity and test-retest reliability of the IFIS has been found to be acceptable among a sample of 9–12 year old youth.83 The IFIS will also be used to evaluate perceived fitness among participating teachers.
Resistance training self-efficacy
Self-efficacy for resistance training will be assessed using a four-item scale developed for use with adolescents.65 Participants report their agreement to each statement (eg, I have the skill and technique to complete resistance training exercises safely) using a five-point Likert scale (1=Strongly disagree, to 5=Strongly agree). Test-retest reliability for this scale has been found to be good (ICC (95% CI)=0.81 (0.64 to 0.90)).65
Secondary outcomes (teacher)
Confidence to teach health-related fitness activities
Teacher confidence to deliver health-related fitness activities will be assessed using an adapted version of an existing scale.84 The original items applied to a variety of learning activities which are typically taught as part of the PE curriculum. For the present study, the items are adapted to apply only to the teaching of health-related fitness activities.
Barriers to teaching health-related fitness activities
Perceived barriers to teaching health-related fitness activities will be evaluated using items adapted from an existing scale, originally applied to delivering the Health and PE curriculum.85 The adapted scale includes many of the same barriers as the original, but focuses instead on the delivery of health-related fitness activities. Additional barriers relevant for health-related fitness activities (eg, litigation concerns) were added to the scale and teachers can add barriers that are not already listed. Teachers respond to each potential barrier using a six-point scale (1=No barrier or does not inhibit, to 6=A major barrier or strongly inhibits).
Process evaluation
A process evaluation will be conducted to determine intervention fidelity and programme acceptability for the RCT and dissemination phases. Process measures will include: (1) teacher attendance and satisfaction with the professional learning workshop (workshop evaluation questionnaires); (2) number of NEAT/ATLAS physical activity sessions delivered (teacher logs and session observations); (3) student participation in the interactive seminars and lunch-time sessions (teacher logs); (4) student engagement with the web-based app (objective usage data); (5) NEAT/ATLAS session fidelity via observations (2 per teacher in RCT and 1 per teacher in dissemination phase); and (6) overall teacher and student satisfaction with the NEAT/ATLAS programmes (process evaluation questionnaire).
RE-AIM46 will provide a framework for the process evaluation of the NEAT and ATLAS interventions during the dissemination phase of the study. As shown in table 3, the RE-AIM framework will be applied to evaluate the interventions at both the organisational and individual levels. RE-AIM47 was operationalised as follows: (1) reach (individual level)—the absolute number, proportion and representativeness of students who participate in the NEAT/ATLAS interventions compared with those who declined and students' attendance at sessions and engagement with web-based app; (2) effectiveness (individual level)—the impact of the NEAT/ATLAS programmes on student health outcomes and behaviours; (3) Adoption (setting level)—the absolute number, proportion and representativeness of schools and teachers who are willing to deliver the NEAT/ATLAS programmes and the impact of the professional learning workshops on teacher outcomes; (4) Implementation (setting level)—the fidelity of the NEAT/ATLAS programmes delivered in schools; (5) Maintenance (setting and individual levels)—the long-term effects of the NEAT/ATLAS programmes on student health outcomes and behaviours, and the extent to which the NEAT/ATLAS programmes have become routine organisational practices within recruited schools.
Application of the RE-AIM framework to evaluate the dissemination of the NEAT and ATLAS interventions
Statistical analysis
Statistical analyses of the primary and secondary outcomes in the RCT phase will be conducted using linear mixed models in IBM SPSS Statistics for Windows, V.20.0 (2010 SPSS Inc., IBM Company Armonk, New York, USA), with α levels set at p<0.05. The models will be used to assess the impact of treatment (intervention or control), time (treated as categorical with levels baseline, 6 and 12 months) and the group-by-time interaction, using random effects to account for the clustered nature of the data. Although randomisation will occur at the school level, our statistical analyses will be adjusted for the clustering of effects at the class level. This is because our intervention will be delivered to students in classes and school-based studies have demonstrated that clustering at the school level is negligible after accounting from clustering at the class level.59 ,86 Mixed model analyses are consistent with the intention-to-treat principle, assuming the data are missing at random. The validity of this assumption will be explored by assessing relationships between missing and observed values of covariates and previous outcomes. Multiple imputation and/or pattern mixture modelling will be considered as a sensitivity analysis if the dropout rate is substantial. Three potential moderators (ie, sex, household SES, and initial weight status) will be explored using linear mixed models with interaction terms and subgroup analyses will be conducted if p<0.1.87 Hypothesised mediators of physical activity and sedentary behaviour change will be examined using multilevel linear analysis and a product-of-coefficients test that is appropriate for cluster RCTs. In the dissemination phase, within group changes will be explored using mixed models and descriptive statistics will be reported.
Ethics and dissemination
Ethics approval for RCT and dissemination phases was obtained from the Human Research Ethics Committee of the University of Newcastle, Australia (H-2014-0312) and the NSW Department of Education and Communities (SERAP: 2012121). School Principals, teachers, parents and students all provided informed written consent prior to enrolment. It is not expected that participants will be at any greater risk of adverse events than they would be when participating in other types of school-based physical activity. However, the teacher handbook includes a section for teachers to report any injuries or adverse events that may occur. Any amendments to the study protocols will be publicly available via the Australian and New Zealand Clinical Trials Registry (Trial number: ACTRN12615000360516). Data management procedures will be conducted by DRL and JS. All entered data will be de-identified using participant codes and will be stored electronically in a password protected drive at the University of Newcastle. Quality checks of entered data will be completed by JS (ie, range checks). Access to the final trial dataset will comply with the conditions of the ethics committee approval and will be at the discretion of the lead CI, DRL. The findings of the RCT and dissemination studies will be published in peer-reviewed journals and all participating schools in the RCT will receive a report outlining the study findings at the conclusion of the trial.
References
Footnotes
Contributors All authors contributed intellectually to the study design and research methodology, or will be directly involved in the collection and management of data. DRL and JJS were responsible for drafting the manuscript. All authors provided critical review and endorsed the final version of the manuscript.
Funding This work was supported by the Australian Research Council (Grant number: FT140100399) and the NSW Department of Education and Communities School Sport Unit.
Competing interests None declared.
Ethics approval University of Newcastle and NSW Department of Education and Communities human research ethics committees.
Provenance and peer review Not commissioned; externally peer reviewed.