Article Text

Abstract
Introduction HIV risk among female entertainment and sex workers (FESW) remains high and use of amphetamine-type stimulants (ATS) significantly increases this risk. We designed a cluster randomised stepped wedge trial (The Cambodia Integrated HIV and Drug Prevention Implementation (CIPI) study) to test sequentially delivered behavioural interventions targeting ATS use.
Methods and analysis The trial combines a 12-week Conditional Cash Transfer (CCT) intervention with 4 weeks of cognitive-behavioural group aftercare (AC) among FESW who use ATS. The primary goal is to reduce ATS use and unprotected sex among FESW. The CCT+AC intervention is being implemented in 10 provinces where order of delivery was randomised. Outcome assessments (OEs) including biomarkers and self-reported measures of recent sexual and drug use behaviours are conducted prior to implementation, and at three 6-month intervals after completion. Consultation with multiple groups and stakeholders on implementation factors facilitated acceptance and operationalisation of the trial. Statistical power and sample size calculations were based on expected changes in ATS use and unprotected sex at the population level as well as within subjects.
Ethics and dissemination Ethical approvals were granted by the Cambodia National Ethics Committee; University of New Mexico; University of California, San Francisco; and FHI360. The trial is registered with ClinicalTrials.gov. Dissemination of process indicators during the multiyear trial is carried out through annual in-country Stakeholder Meetings. Provincial ‘Close-Out’ forums are held at the conclusion of data collection in each province. When analysis is completed, dissemination meetings will be held in Cambodia with stakeholders, including community-based discussion sessions, policy briefs and results published and presented in the HIV prevention scientific journals and conferences.
Conclusions CIPI is the first trial of an intervention to reduce ATS use and HIV risk among FESW in Cambodia.
Results Will inform both CCT+AC implementation in low and middle-income countries and programmes designed to reach FESW.
Trial registration number NCT01835574; Pre-results.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is an experimental study that will assess the efficacy of combined behavioural interventions to reduce amphetamine-type stimulant use in women at high risk of HIV in Cambodia.
The study will investigate the interventions impact on drug use and sexual risk using both biomarkers and self-reported data, and the design allows for analyses that will not be confounded by secular trends in these outcomes.
The stepped-wedge design makes implementing this intervention in 10 randomised provinces feasible and acceptable in the context of extensive multisectoral coordination because a core study team provides ongoing support to multiple implementing partners.
There is a need for ongoing training and study updates to stakeholders, along with clear messages that the trial is testing an intervention that may or may not have the same results as seen elsewhere.
The study is not designed to assess the intervention impact on HIV incidence.
Background
In Cambodia, women engaged in sex work have consistently been the group with the highest prevalence and incidence of HIV. In the late 1990s, almost half (45.8%) of the women sampled were infected, and in 2006, prevalence ranged between 11.7% and 14.7% depending on work venue (non-brothel vs brothel based).1–3 Modelling and IgG BED-enzyme immunoassay studies both indicated that incidence rates also fell from over 10% annually in 1999 to 1.6% in 2006.1 ,2 Comprehensive deployment of basic HIV prevention programmes, including condom use promotion, voluntary counselling and testing, and high coverage of HIV antiretroviral treatment (ART), have contributed to these declines among women.4 Sex work remains a high-risk trade, however, and women engaged in transactional sex, working in a variety of entertainment and sex work venues, continue to show high HIV prevalence, incidence and risk.
We conducted two prospective studies of young adult female entertainment and sex workers (FESW) in Phnom Penh: the first, the Young Women's Health Study-1 (YWHS-1), initiated in 2006, and the second (YWHS-2) initiated in 2009.3 ,5 ,6 Both studies showed high HIV prevalence, 23% and 15.5%, and incidence, 3.5% and 1.2%, respectively, among these young women. Notably, our studies showed that amphetamine-type stimulant (ATS) use, principally in the form of ‘yama’ (ATS in pills) and crystal/ice, was significantly and independently associated with unprotected sex and incident sexually transmitted infections (STI).5 ,6 A large proportion (40.6%) of FESW report any lifetime use of ATS, of whom the majority (70.6%) report using before sex, and 27% report recent use (past 3 months).6 Our group also examined the social, sexual and occupational contexts associated with ATS use by young Cambodian FESWs.7 ,8 Women engaged in freelance sex work or working in brothels were more likely to use ATS than women working in entertainment establishments, who had higher hazardous levels of alcohol consumption. Elevated HIV risk among Cambodia FESW is consistent with studies of stimulant-using populations elsewhere9–11 and underscores the significant need to target ATS use as a driver of HIV infection in this population. Non-injection drug use falls outside of conventionally targeted high-risk behaviours (sexual and injection) in Cambodia and, as a result, there have been no HIV prevention programmes focused on ATS use as a key risk factor among FESW or potentially other groups.
Political, economic and social pressures have resulted in additional new challenges for HIV prevention among FESW.3 In 2008, the introduction of antitrafficking legislation aimed at suppressing human trafficking and sexual exploitation amplified risks.3 ,12 Brothels (previously acknowledged and engaged in HIV prevention programming) were closed and police crackdowns prompted an exodus of brothel-based female sex workers to entertainment venues and street-based sex work. In addition to changes in the sex work landscape, enforcement of the antitrafficking law negatively impacted on women's access to HIV and STI prevention and healthcare services.12 The number of women engaged in entertainment and sex work also increased markedly, coinciding with national and global economic shifts.3 ,13
Multiple overlapping circumstances contribute to high HIV risk among Cambodian FESW, including individual sexual and drug risk exposures, low education and high poverty levels, and the negative impacts of public policy and policing. Central to many women's employment in entertainment venues is the requirement for highly sociable interactions with male customers and, for some women, this extends to transactional sex as an opportunity for income generation. ATS are used by many women to stay awake and work longer and see more clients, which also contributes to HIV risk.6 ,8 Expanded access to ART now joins the backbone HIV prevention platform of HIV testing, condom promotion and diagnosis and treatment of STI as Cambodia aims for HIV elimination.4 However, if this goal is to be achieved, there remains a crucial need for innovative prevention methods that directly target FESW and their multiple intersecting risks.
The evidence base for effective interventions to reduce ATS use remains limited; however, the modest effectiveness of behavioural approaches to reduce stimulant use in developed countries offers an important starting point for countries like Cambodia. Moreover, there is currently no effective pharmacotherapy for treatment of ATS dependence, underscoring the need to implement and test behavioural approaches in this setting. Behavioural interventions such as conditional cash transfer (CCT) and outpatient cognitive-behavioural substance abuse treatment are evidence based for reducing stimulant use.14 ,15 However, relatively little is known about the implementation of behavioural interventions to reduce stimulant use in resource-limited settings like Cambodia where formal substance abuse treatment is often unavailable and structural factors are key determinants of ATS use.7 ,16 The primary aim of this article is to describe the study design and outcomes chosen to evaluate the effectiveness of an intervention targeting ATS use and unprotected sex developed as part of a multipart HIV prevention platform named the Cambodia Integrated HIV and Drug Prevention Implementation (CIPI) programme. We will also describe the operational challenges encountered in attempting to implement this large cluster randomised stepped-wedge trial in 10 Cambodian provinces.
Structure and rationale for the interventions
The CIPI programme includes multiple components, foremost of which is an intervention aimed at reducing ATS use and concomitant HIV risk. The cluster randomised stepped-wedge design was chosen for this intervention as: (1) it offers a significant logistic advantage due to the staggered delivery of employing a core study team, which ensures fidelity to the delivery of intervention while working with multiple NGO partners in the different provinces; (2) allows for analyses that will not be confounded by secular trends in the main outcomes of interest including consistent condom use or number of sex partners; and (3) it provides an ethical benefit of being able to deliver an intervention for which there is evidence of efficacy to everyone within a rigorous scientific framework. Since provinces serve as their own controls, and comparisons can be made across time and between groups, temporal effects, which could impact the study outcomes, can be managed. The intervention period in each cluster is a total of 16 weeks and includes: (1) a 12-week CCT intervention where women complete thrice-weekly urine-screening visits and receive small, escalating financial incentives for consistent ATS abstinence each week followed by; (2) four once-weekly sessions of cognitive-behavioural group aftercare (AC) for women who attend at least half (≥18) of the 36 urine-screening visits during the CCT phase. Adaptation of CCT and cognitive-behavioural AC was informed by the Assessment, Decision, Administration, Production, Topical experts, Integration, Training, and Testing (ADAPT-ITT) model for tailoring evidence-based HIV interventions for new target populations17 and has been described in detail elsewhere.18
Four waves of cross-sectional outcome evaluation (OE) data collection among FESW are being conducted in each cluster: one in the month prior to the CCT+AC intervention implementation and three more at 6-month postintervention intervals following the end of the 16-week intervention CCT+AC intervention (see figure 1).

Illustration of cluster randomised stepped-wedge design testing conditional cash transfer and a cognitive-behavioural aftercare programme.
CCT provides tangible incentives as positive reinforcement for behaviour change. CCT has been implemented broadly to target a range of health and social outcomes including infant mortality, child health and nutrition, tuberculosis, vaccination coverage, schooling, child labour and HIV risk in resource-limited settings.19–26 The documented effectiveness of CCT approaches is based on the theoretical premise that incentives provide positive reinforcement to enhance motivation for behaviour change and that these incentives may also mitigate the effects of structural factors, such as food insecurity and poverty, on negative health outcomes.27
In the substance use treatment field, an extensive literature has examined the efficacy of ‘contingency management’, an evidence-based form of CCT where individuals receive escalating financial reinforcement for providing biological evidence of drug abstinence. Founded on basic behavioural principles, contingency management (henceforth referred to as CCT) yields clinically meaningful, short-term reductions in stimulant use and has been used to promote HIV-related health behaviour change among substance users.14 ,28–30 CCT programmes aimed at stimulant users achieve short-term reduction in stimulant use, which promotes enhanced retention in other substance abuse treatments and potentially better overall substance abuse treatment outcomes.14 ,31–34
Since CCT is a time-limited behavioural approach, there is increasing recognition that expanded efforts may be necessary to support long-term reductions in ATS use once the financial incentive is removed. As a result, the CIPI intervention includes a cognitive-behavioural AC group following the CCT phase to provide skills for effectively managing triggers for ATS use. Drawing on prior research highlighting common change processes that predict better substance abuse treatment outcomes,35–38 the overarching goals of the cognitive-behavioural AC programme are to: build social networks that are supportive of abstinence from ATS use, improve cognitive-behavioural coping skills, and bolster self-efficacy for managing triggers for ATS use. The CIPI CCT+AC intervention aims to assist individuals with achieving clinically meaningful reductions in their ATS use that will result in lower HIV risk.
The CIPI programme also includes a microenterprise (ME) opportunity for women who do not use ATS (identified in OE assessments) or those who successfully complete CCT+AC. The rationale for including the ME opportunity into the CIPI programme was to ensure that all women had a chance to participate in a structural platform aimed at addressing gender-based poverty, an evident and critical determinant of HIV risk. By ensuring that this was available to non-ATS users (baseline) and after the CCT+AC intervention, we also aimed to safeguard against women using ATS as a means to be included in this opportunity. The ME opportunity is not part of the CCT+AC intervention; however, we recognise the considerable potential for further reductions in HIV risk among FESW by integrating multiple prevention approaches into the programme. The ME opportunity includes a 3-day financial literacy training programme and the option to apply for a small business loan. ME is a development tool that has been used to improve a diverse range of health outcomes in numerous populations, including reduction of HIV risk behaviours in FESW.39 Women often engage in sex work because they lack educational and financial opportunities to explore other income-generating options. ME may offer opportunities for women to reduce or cease involvement in transactional sex as a result of both financial and gender empowerment, potentially resulting in improved health outcomes,40–45 reductions in number of sex partners, and lower rates of unprotected sex.46 Implementation of ME-based interventions among sex workers in other settings has shown impressive potential for success.46 The ME opportunity was added to the CIPI programme in order to assess: (1) the potential engagement of Cambodian FESW with this structural intervention; and (2) ME organisations' interest in using this approach; however, it is not being evaluated as part of the ATS risk reduction intervention.
CCT+AC intervention delivery
Eligibility for the 12-week CCT intervention is determined at the preintervention baseline OE assessment(s). Using the WHO ASSIST, eligible participants were required to receive a score of four or higher (ie, >4) on the ATS specific substance involvement subscale47 and provide a urine sample that was positive for ATS (amphetamine or methamphetamine). Women who have completed the baseline OE and are eligible for CCT are provided with additional information about the intervention and an appointment to learn more and participate in a separate informed consent process. We use this tiered method of recruitment to support individual autonomy and minimise any insinuation of undue influence.
CCT programme: CCT participation includes thrice-weekly urine screening for 12 weeks (36 possible urine-screening visits). Participants are encouraged to attend urine-screening visits at the study field site, but screening can also be conducted off-site as needed to accommodate scheduling challenges that may arise in association with work or other personal issues. At each urine-screening visit, participants receive a $2 cash incentive for providing an ATS negative sample. Escalating cash bonuses are provided at the end of each week where all three of the urine samples are negative for ATS: $2 in weeks 1–4, $4 in weeks 5–8 and $6 in weeks 9–12. The goal of the cash incentive is to provide an immediate material positive reinforcement for ATS abstinence, consistent with prior research where more frequent receipt of cash incentives earned in CCT was associated with greater odds of abstinence at subsequent urine-screening visits.48 If participants provide a positive urine test for ATS, they do not receive the visit incentive or a cash bonus for that week. Urine testing results are systematically tracked on a CCT card that provides a visual representation of each visit's results. Using the CCT card, the remaining possible incentive is reviewed with participants at each urine-screening visit. Total possible reinforcement for ATS abstinence over the 12 weeks is $120. (Women report a median income of $US200 per month (IQR: $120–$300). CCT participation could represent an additional $10 per week income).
AC group sessions: Women who complete at least half of the 36 urine-screening visits (ie, ≥18) are eligible to participate in the cognitive-behavioural AC group, regardless of their urine test results. On the basis of a cognitive-behavioural model of treatment for stimulant use disorders, the principal goals of the 4-session once a week group AC programme are to: provide and encourage women to participate in a supportive social environment to assist with avoiding ATS use and/or reducing the harms that they experience related to ATS use, to provide them with skills that are designed to change thoughts, feelings and behaviours to more effectively manage triggers for ATS use, and to bolster self-efficacy for managing triggers for ATS use.18 The AC sessions include: (1) group exercises to facilitate cohesion, observational learning and skill development; (2) skills training for early recovery and relapse prevention by managing internal as well as external triggers for ATS use; (3) meditation and relaxation training and ‘practice’ techniques for managing negative emotions, triggers and cravings for ATS; and (4) a ‘lucky draw’ as a positive reinforcement for attendance wherein women draw a ticket from a prize bowl and can receive a reward in the form of a cash prize ($10, $5 or $2) or applause with positive affirmations.49 Prize bowls for each 4-session AC group include a total of 110 tickets, including one $10 ticket, 11 $5 tickets, 48 $2 tickets and 50 tickets for applause and positive affirmations from the group. Tickets are drawn without replacement. Lucky draw cash incentives are provided immediately.
ME opportunity delivery
Women who are ATS negative at preintervention baseline OE (ATS ASSIST score <4 and negative test results for ATS) and ATS using women who complete enrolled in CCT+AC and completed all weekly CCT urine-screening visits in the past 2 weeks of the 12-week programme with negative test results for ATS and attended all four AC sessions, and test negative for ATS at OE-1 are eligible for the ME opportunity.
Methods
Trial design
The goal of the CIPI intervention is to reduce ATS use and HIV risk via implementation of an evidence-based CCT+AC intervention directed at biologically confirmed ATS users. The trial uses a cluster randomised stepped-wedge design as illustrated in figure 1 to deliver the intervention with cluster randomisation at the province level.50 ,51 Ten provinces (figure 2) were randomised to 1 of 10 different initiation periods by the study statistician using a random number generator. Each province will function as its own control in a time series analysis. The intervention is conducted at the individual level. Preintervention baseline (BL-OE) was conducted in each province prior to CIPI implementation with a goal of 120 women participating at the first evaluation time point. The first BL-OE was conducted in June 2013. In the first four provinces, the BL-OE was conducted twice, at 3 months and 1-month prior to beginning CCT. In the subsequent seven provinces, the BL-OE was administered only at 1 month prior to CCT initiation. The preintervention or ‘baseline’ wave of data collection was planned to include 120 eligible women. Using estimates from our previous research showing that 25% of FESW actively use ATS,6 we estimated that 30 women would be eligible for CCT based on results in the baseline OEs. Analyses will compare OE data collected prior (BL-OE) to OE data collected and follow the conclusion of the CCT+AC intervention (OE-1, OE-2 and OE-3).
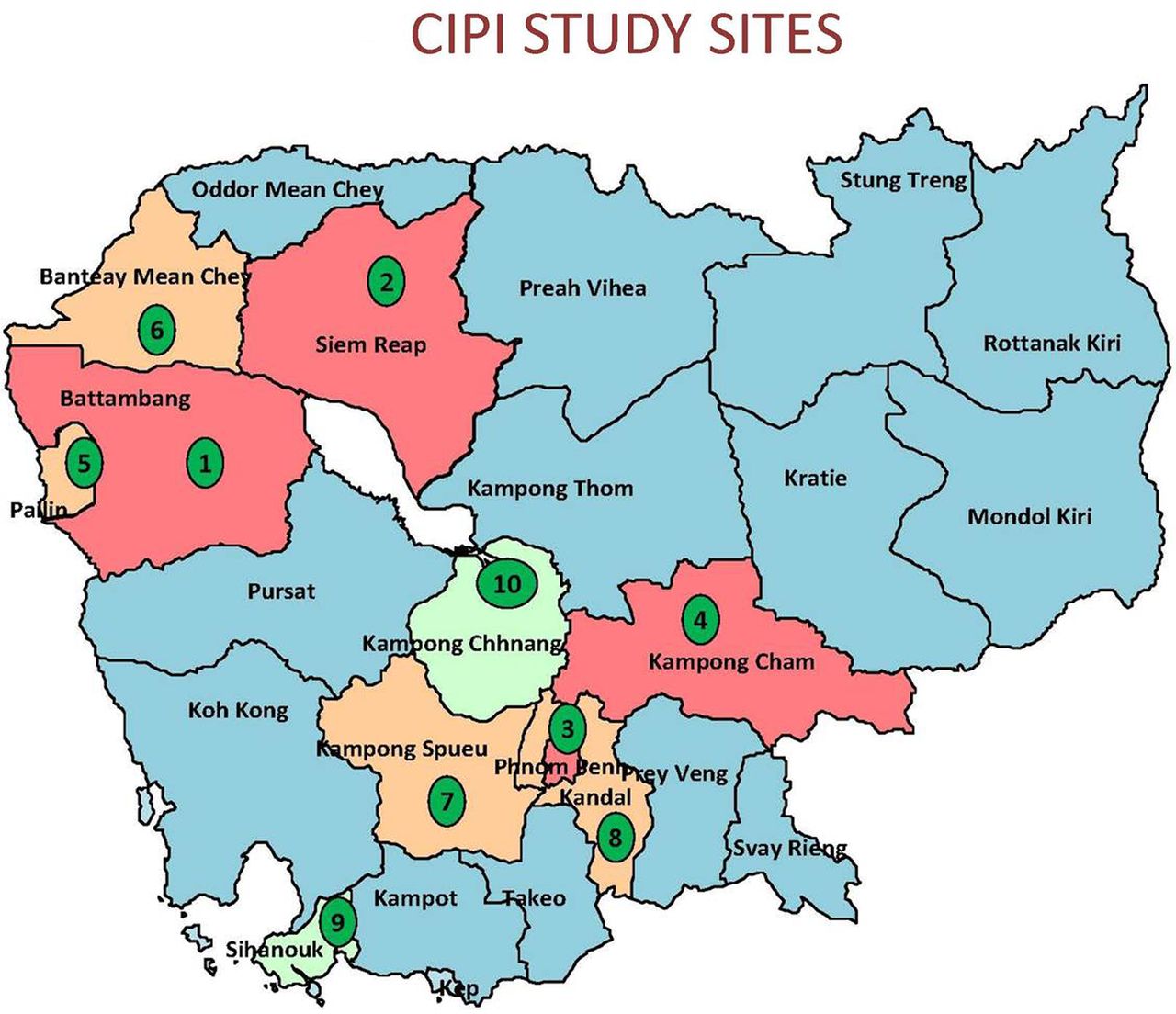
Map of Cambodia with cluster provinces and randomisation order.
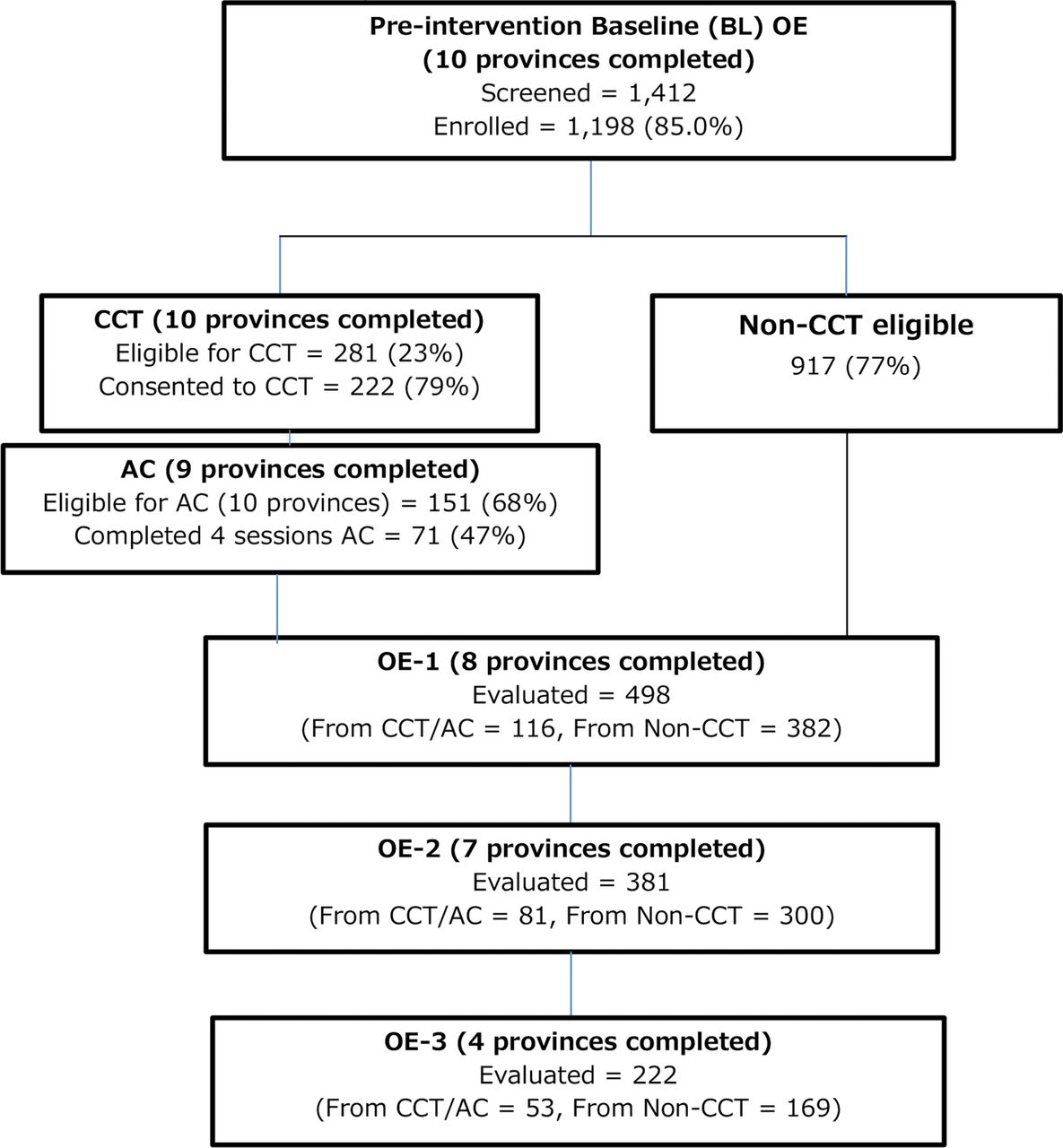
Figure 3 shows the CONSORT study flow diagram for the CCT+AC intervention through 30 September 2015. The 10-province intervention implementation involves multisectoral collaborative partnerships, and engagement in training and community information sessions, followed by intervention delivery with preintervention and postintervention outcome assessments. The intervention was extensively planned with involvement from numerous community and governmental groups. The study protocol was informed by qualitative formative research with FESW regarding the acceptability of the proposed CCT+AC intervention and barriers and facilitators to trial participation, including incentive amounts, transportation assistance, directly observed urine specimen collection, and the content of the AC programme described in detail by Dixon et al,16 in a separate report. Two governmental partners including the Cambodian Ministry of Health Department of Mental Health and the National Authority to Combat Drugs were involved early in protocol planning.

{kind=link}
{kind=link}
{kind=link}
CIPI CCT+AC Intervention: flow and process data from 10 Cluster Provinces*. AC, aftercare; CIPI, Cambodia Integrated HIV and Drug Prevention Implementation; CCT, conditional cash transfer; OE, outcome assessments.
Early in the planning process, a Stakeholder Forum attended by over 35 governmental and non-governmental stakeholders was held to review and solicit input on the proposed project. A CIPI Task Force (TF) was convened from this meeting, and Terms of Reference for members were developed to articulate the purpose and responsibilities of the TF involvement. The TF meets annually and is apprised regarding the study progress, as well as to exchange information and feedback about health and HIV risk issues relevant to FESW in Cambodia. Once implementation began, the CIPI programme was publicised and publicly endorsed by governmental partners in each province through formal orientation workshops delivered to stakeholders in each province prior to or concurrent with implementation initiation. Stakeholders included local governmental and health leaders, NGO staff (heads and outreach workers), as well as police and patient advocates.
Setting
The current widely disseminated model or ‘standard of care’ programme aimed at reducing HIV risk and HIV among FESW in Cambodia is called ‘SMARTgirl’.52 Launched nationally in 2009 as a social marketing health promotion programme aimed at women working in the high-risk entertainment sector with support from the President's Emergency Plan for AIDS Relief (PEPFAR), SMARTgirl uses targeted communication tools to promote use of health information, HIV testing, STI and reproductive health service referral. It is implemented by local NGO. Women are offered ‘membership’, which is free, and have access to a ‘club’ that serves as a drop-in centre, where they hold events as well as provide health information and referrals. Integrating CCT+AC within the activities of the existing SMARTgirl programme leverages infrastructure that is in place to reach high-risk women, and positions ATS prevention in an accepted HIV prevention context. Since sex work and drug use are illegal in Cambodia, this strategy may potentially reduce the stigma and other negative social consequences that render drug use interventions difficult to implement in this setting. The 10 target clusters (provinces) were chosen on the basis of three criteria: (1) presence of SMARTgirl HIV prevention activities; (2) high numbers of FESW enumerated as part HIV prevention programming;53 and (3) moderate to high HIV prevalence based on data from antenatal surveillance.54
Training
In each province, a designated NGO is responsible for delivering the SMARTgirl programme. Each of these partners was engaged to coordinate recruitment and retention of eligible FESW in the 10 provinces. Community partners were also engaged in delivering CCT. Training included the following components delivered by researchers and staff over 5 days: (1) Recruitment and retention of high-risk FESW and ATS using FESW; (2) Administering the study survey and collecting biological specimens (ie, urine samples and vaginal swabs) during OE assessments; (3) Conducting CCT urine-screening visits; (4) Delivering brief counselling messages based on risk profiles from study assessments; and (5) Managing participant data in the field using computer-based data collection methods.
Inclusion criteria
The target population for CIPI is Cambodian FESW who: (1) are biologically female; (2) aged ≥18 years; (3) report≥2 different sexual partners and/or transactional sex within the past month; (4) understand spoken Khmer language; and (5) are able to provide voluntary informed consent. Transactional sex includes exchanging sex for money, goods or social favours. FESW may work in the entertainment sector, such as in beer gardens, bars, massage, karaoke and other ‘entertainment’ establishments, as well as in other venues including parks and guesthouses. Targeted efforts were employed to enrol high-risk women, including those using ATS, although this was not an explicit inclusion criterion.
Exclusion criteria
The study excludes those who were born male; women aged less than 18 years (due to employment laws in Cambodia); women who cannot speak Khmer; women who are unable to provide informed consent; and those who report <2 different sexual partners or transactional sex in the past month.
Recruitment and enrolment
In all provinces, CIPI outreach workers recruited eligible participants from multiple locations including: SMARTgirl clubs, entertainment venues and other locales where FESW are known to congregate or work. Outreach workers conducted a preliminary verbal screening for eligibility, provided a basic study description, answered questions, and invited them to attend the local study site (SMARTgirl Club) for eligibility evaluation and, if interested, study participation. Transportation to the site was provided or reimbursed (up to $2). Eligible women who provided informed consent to participate were asked to provide their fingerprint at the time of initial enrolment using a commercially available digital fingerprint reader that converts and stores biometric images as an alphanumeric code (PersonID Fingerprint Identification System, Bayometric, San Jose, California, USA). The same finger will yield the same code at subsequent occasions in >99.9% of cases, and in this study was used to remove the need for identification at follow-up visits. The code is not a personal identifier as it cannot be used to recreate a fingerprint.
Data collection
The OEs are conducted prior to and following the CCT+AC intervention (figure 1). The survey includes self-reported measures of ATS and alcohol use using the WHO Alcohol, Smoking and Substance Involvement Screening Test (ASSIST).47 ,55 Participants who report any ATS use or screen positive for an alcohol use disorder receive a brief, scripted counselling message from study staff advising them to reduce or abstain from these substances as per the WHO ASSIST validation study, which identified ASSIST scores that maximise sensitivity and specificity of identifying alcohol and stimulant use disorders.47 ,55 ,56 The survey is administered privately; it takes approximately 60 min or less, and also collects information on: socioeconomic indicators, work history including sex and entertainment work, sexual and drug use behaviours, use of HIV testing and reproductive health services, economic well-being, empowerment, depressive symptoms and self-efficacy.
Biological data collection includes on-site urine testing for ATS, prostate-specific antigen (PSA) and HIV. Each participant is instructed on providing a urine specimen to be tested for ATS metabolites (ie, methamphetamine and amphetamine). Urine is tested for adulteration using Specimen Validity Testing (Innovation, Inc, San Diego, California, USA), and for ATS metabolites using the Innovacon Multi-Drug Screen Test Panel Dip Kit (Redwood Toxicology Laboratory, Inc, Santa Rosa, California, USA). Women are instructed on how to provide a self-collected vaginal swab for PSA testing, a reliable biomarker of seminal fluid exposure and bio-indicator of recent unprotected vaginal sex.57 PSA is tested for using the OneStep ABAcard p30 rapid PSA test (Abacus Diagnostics, Inc, West Hills, California, USA). A rapid HIV antibody test (Determine TM: HIV1/2; Alere Medical, Co, Ltd, Chiba, Japan) is administered twice: at baseline OE and postintervention at OE 2 (12 months after CCT+AC). HIV testing procedures are in accordance with the Cambodian National Guidelines and conducted by trained staff; results are provided within 30 min of testing. Each participant receives HIV risk reduction counselling and referrals to follow up HIV care or other services as needed. Participants are remunerated in cash in US dollars (a currency widely used in Cambodia): $4 for participation, $2 for transportation and offered refreshments and condoms at the study site. Participants are asked for basic contact information such as a mobile phone number and home address so that outreach workers can remind them of future visit appointments.
Quality assurance
The study has ongoing quality assurance procedures. At the study headquarters in Phnom Penh, the field-site supervisor and statistician/data manager perform regular data verification and protocol compliance checks. The study supervisor performs on-site monitoring of concluded surveys at each study site for data completeness, legibility and logical consistency. The supervisor and data manager also periodically observe interviews. Research staff from the lead in-country implementer, FHI360, conduct routine monitoring visits to each province to ensure fidelity to the CCT+AC intervention throughout the study. They are responsible for compiling numbers of participants recruited, completing required assessments, maintaining databases and identifying missing data and missing follow-up assessments. The research assistant prepares recruitment and missing data reports for weekly review by the study supervisor. All data are stored on a firewall-protected server in Cambodia and transferred monthly to the study statistician at UCSF using secure methods, where it is reviewed again for consistency and completeness. Inconsistencies and questions are resolved by reviewing source documents. Local provincial staff employ several strategies to achieve the highest retention possible in OEs, the CCT-AC intervention and the ME programme. These primarily consist of telephone visit reminders and calls to reschedule missed visits for those who have an active phone line, and repeated visits to participants’ home or work locations for visit reminders and in cases of missed visits. Recruitment, follow-up rates and missing data are discussed during regular team meetings, and both investigators and field staff strategise to solve problems and remedy the shortcomings.
Ethical issues and approvals
The study population is marginalised and engaged in illegal behaviours and sensitive behavioural and biological data are being collected. The study is in compliance with ethical principles for human subjects research promoted by the Declaration of Helsinki developed by the World Medical Association. Various procedures are adopted to ensure additional protection for all women screened and enrolled in the trial including: waiver of signed informed consent to minimise the risk that any information may be linked to names and be reported. The fingerprint reader cannot be linked to personal identifiers. The consent process is conducted carefully to ensure that potential participants understand research objectives, procedures, risks and benefits, reimbursement, costs and alternatives, and a short verbal assessment is conducted to ensure understanding. Very importantly, the study's process to include stakeholders is also a significant step in ensuring protections as local governmental and health leaders, NGO staff (heads and outreach workers), as well as police and patient advocates are informed and engaged in the safe and successful implementation of the project. The study team monitors for adverse events, both physical and social. The study has a Data Safety and Monitoring Plan and Board (DSMP; see below).
During the implementation, yearly stakeholder meetings have been held to report on process outcomes. Provincial ‘Close-Out’ forums are held at the conclusion of data collection in each province. Study results will be disseminated after analyses are completed through various channels, including stakeholder meetings, community-based discussions, policy briefs, written reports and publications, national (Cambodian), regional and international conference venues, and media releases where appropriate.
Data safety and monitoring
The study has a DSMP and a Data Safety Monitoring Board (DSMB). The DSMB includes investigators with experience in women's health, epidemiology, biostatistics and HIV prevention in the Southeast Asian region. The DSMB met three times during the first 18 months of the trial, and now meets yearly to review reports of study progress, enrolment and any adverse events that occur. Reports are also sent to the sponsor at the National Institute on Drug Abuse.
Analyses
The CCT+AC intervention is being implemented and evaluated using a cluster randomised stepped-wedge trial design to assess whether the intervention reduces ATS use and unprotected sex greater than the underlying secular trend at the individual and cluster levels. The primary outcomes being assessed are indicators of recent (in the past 3 months) risky sexual behaviour: (1) PSA test results (positive vs negative); (2) self-reported consistent (always) condom use with recent paying and non-paying partners during vaginal or anal sex and (3) self-reported number; and (4) type of sex partners (paying and non-paying). These were chosen on the basis of our prior research showing prospective associations between ATS use and high-risk sexual behaviour.6 Secondary outcomes include: recent ATS use (by self-report using ASSIST, and urine-based testing), patterns of ATS use including frequency, quantity and binge use; and alcohol use (using Audit C and ASSIST). We will also evaluate associations between CCT+AC and exploratory outcomes including: medical and health service use (ie, HIV testing history, HIV results, HIV treatment, STI testing and treatment); visits to reproductive health clinics, live births, pregnancy terminations in past year, birth control use; and measures of economic well-being and empowerment.
Analyses will account for account for potential within-cluster correlation due to the design using generalised estimating equations. The stepped-wedge approach can be described as a one-way crossover design with each randomisation unit spending time in intervention and control conditions. Analyses will compare outcomes from data collected preintervention to postintervention, including assessing the short-term impact (6-months post-CCT+AC) and to assess durability (12 months and 18 months post-CCT+AC). The effects of the intervention will be examined using an intent-to-treat approach. Secondary analyses of as-treated results will be conducted with data collected on the extent of the CCT+AC intervention participation.
Sample size estimates
We estimated sample size and power on the basis of two of the primary HIV risk outcomes: (1) number of sex partners and (2) unprotected sex as measured using PSA testing. We chose preintervention estimates of these outcomes based on our previous work.3 ,5 ,6 For number of sex partners, a sample size 600 (300 in CCT and 300 non-CCT) across 10 provinces (clusters) with 60 (with 30 women in CCT) individuals per cluster achieves 80% power to detect a difference in means of 0.243 between the groups (or a drop from 1.80 partners/month to 1.56 partners/month) when the SD is 1.0 and the intracluster correlation is 0.01 using a two-sided t test with a significance level of 0.05. For unprotected sex, a sample size of 600 with preintervention and postintervention measurements obtained by sampling 10 clusters with 60 patients each in a group achieves 80% power to detect a minimum reduction in the proportion testing positive for PSA of 8% with a baseline (preintervention) proportion of 22% testing PSA positive. The CCT arm of the intervention will enrol 300 women or 30 women per province. Sample size estimates were performed by first using the formula from a balanced, parallel group design and then adjusting the values upward by a factor of 1.44 to account for the decreased efficiency of the stepped-wedge design due to the unequal allocation of preintervention and postintervention outcome assessments.
Trial status
The CIPI intervention was initiated in June 2013 with the first preimplementation OE evaluation survey and data collection among 120 women recruited in the first randomised province: Battambang. Four of the 10 provinces had 2 preimplementation OE assessments; the remaining 6 provinces had 1 preimplementation OE (figure 1). As of 30 September 2015, all 10 provinces have completed preimplementation OE assessments with a total of 1198 women enrolled (figure 3). The CCT-AC intervention has initiated in all 10 provinces with 281 women eligible, and 222 enrolling. The CCT+AC intervention has been completed in 8 of the 10 provinces. The first postintervention OE assessment (OE-1) has been completed in 8 provinces (N=498), the second (OE-2) in 7 provinces (N=381), and the third and final evaluation (post-OE) has been completed in 4 provinces (N=222). Of 288 women eligible for the ME opportunity, 195 (68%) consented to participate (the majority (90%) non-CCT+AC participants); 178 (91%) completed the 3-day financial literacy training, 38 (21%) applied for microloans, of whom 27 (67%) were approved and funded. We anticipate completing data collection in all provinces by November 2016.
Discussion
Although there is evidence that CCT+AC interventions can reduce stimulant use, most studies to date have been conducted in developed countries, and principally among men who have sex with men.14 ,34 ,58–61 To the best of our knowledge, this is the first study to examine the effectiveness of this evidence to an intervention delivered to high-risk women in a resource limited setting. Given the absence of safe and effective medication assisted treatments for stimulant use, there is a strong need for evidence-based behavioural approaches that have demonstrated effectiveness for ATS users in other settings and especially in resource-limited ones such as Cambodia. The CIPI programme is being implemented in close collaboration with multiple stakeholders including governmental and NGO partners and, if shown to be effective, has potential for widespread implementation in the Cambodian context. The cluster randomised stepped-wedge design has met the logistic expectation for ease of implementation across the 10 provinces and with multiple partners since the core study team has been able to travel to each site and ensure fidelity to the protocol across sites. Community stakeholders have expressed appreciation that their province is receiving the intervention, suggesting that there are no feelings of inequity. Data collection has not ended and analyses have not begun on any of the study outcomes, which has frustrated community partners and the stakeholders at the yearly meeting, and been challenging for researchers to address.
Although not a primary outcome of this trial, the ultimate goal of our intervention is to reduce HIV infection by decreasing ATS use a key risk factor for Cambodian FESW. In addition to collecting data on HIV testing and results over the study period, HIV infection is being measured at two time points; however, the trial is not powered to detect differences in HIV incidence outcomes. By joining the CIPI intervention to the SMARTgirl programme, which provides support to women to engage in reducing sexual risk and improving reproductive health engagement, our programme has the potential to add value and impact to an existing programme which in 2012 was estimated to reach over 15 000 Cambodian FESW.62 In addition to the outcome measures described above, we are also tracking programmatic factors including the number and proportion of CIPI participants using contraceptive methods, uptake of family practice screening and subsequent contraceptive uptake, and uptake of referrals for HIV, STI testing and, among women who are HIV-positive, those who link to clinical services for HIV treatment.
The study implementation includes significant process and outcome indicators, and a detailed recording of practice, implementation notes and recruitment assessments. Refusal assessment for the CCT+AC intervention enrolment, however, is not undertaken systematically. In brief informal conversations conducted about reasons for refusal to participate in CCT+AC, the most commonly offered reasons included being ‘too busy’, migration and ‘changing schedule’.
We also encountered challenges in the scheduled roll-out of the study. Pragmatic considerations including the Cambodian holiday calendar and local funding changes to NGOs, which impacted the availability of personnel, necessitated minor modifications to the trial timeline. CIPI was initiated 1–3months later than was initially scheduled in some provinces. Scheduling for the 6-month postintervention OE assessments was not impacted. The trial design also underwent adaptation in June 2014, due to cost factors, principally operational and personnel-related, resulting in eliminating one of two preimplementation OEs in each province to one preimplementation OE prior to CCT-AC intervention delivery. Four provinces had two preimplementation OEs, and the remaining six had one. This adaptation did not impact quality control or protocol fidelity as the intervention was rolled out on the basis of an ongoing review of process indicators by study researchers.
While there are other evidenced-based interventions that could be implemented to address ATS use,31 and unprotected sex63 among FESW, many involve intensive behavioural treatments that require significant resources to support implementation and extensive fidelity monitoring. The approach used in the CIPI intervention aims to build on the current key HIV prevention programming for FESW in Cambodia such that implementation is coupled with existing resources currently in place.52 Use of formative qualitative research and extensive consultation, and collaboration and coordination across multiple sectors and stakeholders, meant that we were able to identify and address key concerns and preferences and to take these into account in developing or modifying the trial protocol in order to optimise the acceptability of the intervention and the implementation of the trial. The stepped-wedge design makes implementing this large-scale intervention feasible and acceptable in the context of extensive multisectoral coordination because a core study team provides ongoing support to multiple implementing partners in different provinces, and especially as all randomised provinces receive the intervention, which obviates the need for designated control provinces and potential community concerns about equity and ethical issues. Even without a control group, the study team has to be very clear that the project is testing an intervention that may or may not have the same results seen elsewhere. The workshops and stakeholder meetings have been essential to providing this information in an ongoing manner.
Importantly, CIPI is the first trial assessing the impact of a CCT+AC intervention in reducing drug use and HIV risk to be conducted in Asia. In resource-limited settings like Cambodia, CCT and time-limited, cognitive-behavioural interventions represent potentially scalable approaches to reducing ATS use and optimising HIV/AIDS prevention efforts. Results from the CIPI CCT+AC intervention have the potential to inform the science of HIV and drug prevention implementation in low and middle-income countries to achieve an AIDS-free generation.
Acknowledgments
The authors would like to express our gratitude to Amy Weissman for supporting the implementation of this project, Chim Srean for coordinating data management in the field in its early phases and Phou Maly for her ongoing and invaluable work in the field as a supervisor and facilitator for the aftercare groups. The authors would also like to thank Drs Rick Rawson and Steve Shoptaw for their consultation with our team in adapting Matrix Model early recovery and relapse prevention skills for this population. The authors are indebted and grateful for the ongoing support of numerous non-governmental organisations who have made the implementation of this project possible: Cambodian Women for Peace and Development (CWPD), Phnom Srey Organization for Development (PSOD), Poor Family Development (PFD) and KHEMERA. This research would not be possible without the support from the Cambodia National Ministry of Health Department Mental Health and Substance Abuse and the National Authority for Combating Drugs. Finally, the authors would like to acknowledge the gracious and considerate involvement of the following organisations working to make microenterprise opportunities available to women in the CIPI study: Chamroeun, Phnom Srey Organization for Development-Asian Community Trust (PSOD-ACT) and Vision Fund.
References
Footnotes
Contributors The CIPI trial is part of a five-year research programme led by KP and ESS. AWC, JLE, LM, EN and CM conceived the research questions and designed the CIPI intervention with contributions from MS and SN. All authors were part of a trial design group led by KP. KP wrote the manuscript with contributions from ESS, AWC, JLE, MS, CS, CM and LM. All authors commented on and approved the final version of the manuscript.
Funding The study is funded by the US National Institutes of Health (NIH) National Institute on Drug Abuse (1R01 DA033672; Page & Stein, PIs). The funder is not involved in the study design; collection, management, analysis and interpretation of data; writing of the report; and the decision to submit the report for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Ethics approval Cambodia National Ethics Committee; University of California San Francisco IRB, University of New Mexico Health Sciences Center IRB and FHI-360 IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data presented in this paper are available from the corresponding author on request.