Article Text

Abstract
Objective To develop and validate an instrument to assess adherence to each individual drug taken by patients undergoing long-term treatment.
Design Multicentre prospective observational validation study.
Setting Six general practitioners' clinics and 6 university hospitals in Paris, France.
Participants Patients 18 years and older receiving at least one long-term treatment.
Methods The instrument was developed from a literature search and interviews with experts. Clarity and wording were assessed during pilot testing with 51 patients. The tool was validated in a sample of consecutive patients. We assessed agreement between adherence measured with our tool and drug diaries and compared measurements from our instrument with (1) the Lu instrument; (2) the Adherence Estimator (AE); (3) patient's adherence assessed by physicians; (4) the Morisky Medication Adherence Scale-4 items (MMAS-4); and (5) the Treatment Burden Questionnaire (TBQ). Reliability was assessed by a test–retest method.
Results A total of 243 patients taking 961 drugs were recruited in 2014. We found good agreement between adherence measured by our tool and drug diaries (intraclass correlation coefficient (ICC) 0.69, 95% CI 0.34 to 0.91) and a linear relationship between measurement with our tool and (1) the Lu instrument (p<0.01); (2) 2 items of the AE (perceived need for medication (p<0.01) and concerns about medication (p<0.01)); (3) patients' adherence assessed by their physicians (p<0.01); (4) the MMAS-4 (p<0.01) and (5) the TBQ (p<0.01). Reliability of the retest was good (ICC 0.67, 95% CI 0.42 to 0.85).
Conclusions We developed an instrument with acceptable validity and reliability to assess adherence for each drug taken by patients, usable in hospital and primary care settings.
- questionnaire
- medication adherence
- validity
- GENERAL MEDICINE (see Internal Medicine)
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Our instrument describes the different medication-taking behaviours for each drug taken by a patient. It may allow clinicians to identify how patients routinely manage their multiple drugs.
Our instrument was validated in a sample of inpatients and outpatients.
Measurements of adherence using our instrument illustrate the variability in adherence among the different drugs taken by a patient and the importance of rethinking adherence drug by drug.
We did not compare measurements from our instrument against electronic monitoring devices.
External validity of our instrument in other countries with different healthcare systems may be limited.
Introduction
The WHO suggested that ‘solving the problem of medication non-adherence, defined as the extent to which a person's behavior fails to coincide with medical advice, would be a greater improvement than any biomedical discovery’.1 Control of many illnesses depends on patient adherence to drug regimens. However, studies have shown that approximately 50% of patients stop taking their medications 6 months after drug initiation.2 ,3 This situation may lead to increased hospitalisation rates and long-term mortality.4 ,5 Clinicians and researchers need tools to detect medication non-adherence. Many strategies have been developed: pill counting, prescription refill rates, drug diaries, biological markers, electronic monitoring devices, etc.1 ,6 ,7 Each method captures different aspects of medication adherence.6 For example, electronic monitoring devices provide accurate information on time of container opening8 but may be intrusive and of limited use in routine practice for patients receiving multiple medications. In contrast, prescription refill rates can provide data on medication adherence in ‘real life’, but information on medication-taking behaviours (eg, schedule errors, omissions of doses, treatment discontinuation, etc) may be limited.
Measurement of adherence is a complex task because patients could adhere differently to their multiple drugs9 ,10 and exhibit various medication-taking behaviours.2 ,11 Thus, it is important to understand how patients routinely manage their treatment because different intake behaviours could be associated with different consequences.11 In routine care, self-reported questionnaires are the simplest and cheapest way to assess adherence,12 ,13 although patients tend to overestimate their adherence.3 ,14 There are many questionnaires in the literature to assess adherence, but most have been developed for specific conditions or treatments,15–17 and their measurement often focuses on predictors or factors of adherence18 or on quantitative rates of medication intake.19
In this study, we aimed to develop and validate a self-reported questionnaire to assess medication adherence for each individual drug taken by patients with long-term drug treatment, suitable across any treatment context.
Methods
This project involved: (1) theoretical conceptualisation of the tool, (2) development of the tool and (3) assessment of its measurement properties.
Theoretical conceptualisation of the tool
The theoretical conceptualisation of the tool was based on the taxonomy published by Vrijens et al,20 which describes adherence as a process divided into three quantifiable phases: initiation (first dose taken), implementation (defined as the extent to which a patient's actual dosing corresponds to the prescribed dosing regimen) and discontinuation (the end of the therapy). Persistence is defined as the length of time between initiation and the last dose taken. According to this conceptual framework, we aimed to develop a tool describing several medication-taking behaviours (ie, discontinuation, drug holidays, missing doses and schedule errors) to capture implementation and persistence. Indeed, it could help clinicians better understand how patients manage their treatments and find appropriate patient-centred solutions.
To elaborate the items of the tool, we used the results from three systematic reviews6 ,12 ,21 completed by a search in MEDLINE via PubMed for recent studies describing medication adherence and questionnaires to assess it. Published self-reported questionnaires are often specific to disease areas or treatments,15–17 ,22 ,23 focused on patient beliefs,18 ,24 or not adapted to assess differential adherence for each drug taken by the patient.25 In addition, most of them provide a single value for measurement of adherence (eg, considering a patient who takes <80% of the doses as ‘non-adherent’).3 This approach remains satisfactory for comparing patients' adherence in trials focused on one drug. However, it may be limited in routine practice as it does not inform on differences in adherence to multiple drugs.9 ,10 To the best of our knowledge, only a few published questionnaires26 ,27 take into account the fact that patients may adhere differently to multiple medications. We aimed to provide complementary information to these tools by describing medication-taking behaviours. We also wanted to design a tool suitable for any treatment context, and able to assess adherence for each medication taken by patients.
Development of the tool
We followed a recommended multistep approach to develop the tool.28
Elaboration of the tool
After a review of the literature, a working group composed of a medical resident (CC), two general practitioners (SS and V-TT) and a professor of epidemiology (PR) drafted five questions related to (1) early discontinuation of the drug; (2) systematic omission of a daily dose (eg, at noon); (3) drug holidays; (4) skipping doses and (5) schedule errors. For each question, we devised possible answers with practical examples and pictographs. Our approach was pragmatic: we asked patients to select the answer that best applied to them, even if their drug intakes did not exactly fit the suggested answers. We hypothesised that this approach would be easier for patients than asking them for an accurate number of doses missed.14 For example, we considered that a patient usually missing a single dose every month would have had difficulties choosing between ‘once a month’ and ‘less than once a month’.
Interviews of experts
One investigator (SS) interviewed four experts—two physicians, one pharmacist and one methodologist—with research experience in the field of medication adherence. During semistructured interviews, she asked them about (1) the relevance of the tool; (2) the clarity of questions, possible answers, pictographs and (3) the global feasibility of the questionnaire. The working group considered their comments and modified the preliminary tool. This step ensured the tool's content validity.
Pilot testing
We performed a two-step pilot testing in April 2014. Consecutive patients were recruited in one university hospital and four general practices in Paris, France. First, we asked 34 consecutive patients to complete the questionnaire. Then investigators performed a double interview method: they asked participants to explain what each item meant to them and why they chose a particular response. Discrepancies between what was intended and what was understood were noted.29 Our working group adapted the tool according to patients’ answers. In a second step, we tested the revised instrument with 17 different patients whose responses suggested good acceptability of the tool. The resulting tool (online supplementary figure S1) contained five questions with two or three possible answers to each question. Each question was illustrated with practical examples and pictographs to help patients recognise their behaviours.30 ,31 We used non-threatening sentences adapted from the literature3 to reduce social desirability bias.6
Supplemental material
Characteristics of the 51 patients in the pilot test are detailed in online supplementary table S1.
Definition of adherence at drug level
On the basis of our clinical experience and the literature,3 ,32 we defined six drug adherence levels for a given drug (table 1). Level 1 corresponded to high drug adherence (no drug holidays, no missing doses and no schedule errors) and level 6 corresponded to drug discontinuation.
Six levels of drug adherence
Definition of adherence at the patient level
To allow comparisons between our tool and other measures of adherence, we defined patient adherence level as the adherence level for the drug for which the patient was the most non-adherent (see online supplementary table S2). We performed a sensitivity analysis to explore whether other definitions (patient adherence level defined as the mean or median drug adherence level) would change our results.
Evaluation of the tool's measurement properties
We evaluated the instrument's properties by studying validity and reliability. We validated the instrument at the drug and patient levels.
Participants and drugs
We recruited consecutive patients in six general practices and six care units of university hospitals in the Ile-de-France region, France. Patients were eligible if they were ≥18 years old; were receiving at least one drug requiring long-term use initiated for at least 30 days; gave written consent to participate; and were able to write answers in French. We excluded patients with cognitive impairment or a language barrier and those who received medication from a nurse or a home care provider. We did not include drugs prescribed if needed or for an acute condition.
The list of drugs taken by the patient was obtained by a review of medical records by the investigators (SS or CC) and by asking the patient if he or she was using additional over-the-counter medications. Drugs were categorised independently into drug classes by two investigators (CC and SS) using a classification adapted from pharmacy claims.33
Assessment of the tool's measurement properties at the drug level
Validity
Criterion validity was assessed by evaluating the agreement between the level of adherence to the drug assessed with our tool and drug diaries. Each patient was asked to complete a 14-day diary for only one drug chosen randomly among his or her medications to improve acceptability and feasibility. One investigator (SS) assessed the drug adherence level in drug diaries. Each reported drug intake was considered a taken dose and each missing intake a missing dose; schedule errors were assessed by counting time intervals between reported doses.
Construct validity was assessed by comparing measurements from our instrument and the following measures. Among possible scales, we chose those usable across any treatment context and requiring a short response time in order to minimise the burden for respondents:
Lu et al's14 instrument was completed by patients for all medications. This self-reported adherence instrument has been validated in HIV-positive patients and measures patients' average ability to take their medication as prescribed. The instrument uses a six-step scale ranging from ‘very poor’ to ‘excellent’. We generated a French-language version of this instrument usable for each prescribed drug during a translation procedure34 ,35 detailed in online supplementary table S3. Cognitive testing performed during the first pilot testing led to adaptation of the instrument in an 11-step rating scale ranging from 0 (very poor) to 10 (excellent). We hypothesised a linear relationship between measurement by our tool and the Lu instrument.
The Adherence Estimator (AE)18 was completed by patients for all medications. This self-reported adherence instrument is a validated three-item tool that predicts intentional non-adherence associated with beliefs about medicines. Scores for each item (perceived need for medication, perceived concerns about medication and perceived medication affordability) range from 1 (agree completely) to 6 (disagree completely). We generated a French-language version of this instrument (see online supplementary table S3). We hypothesised a linear relationship between measurement by our tool and the AE instrument.
Drug adherence for each medication was assessed by the physicians taking care of the patients. They were asked to best estimate the patient's adherence for each drug using an 11-step rating scale ranging from 0 (very poor) to 10 (excellent). We hypothesised a linear relationship between measurement by our tool and physicians' evaluation.
Reliability
Reliability of the measurement of adherence at drug level was determined by a test–retest method. Patients completed our instrument at baseline and after 1-month.36 Retest questionnaires were sent by postal mail to patients.
Assessment of the tool's measurement properties at the patient level
Validity
Construct validity was assessed by comparing measurements from our instrument and the following measures: the Morisky Medication Adherence Scale-4 items (MMAS-4)25 and the Treatment Burden Questionnaire (TBQ).37
The MMAS-425 was initially developed among patients diagnosed with hypertension. It has been validated in inpatients and outpatients, various conditions and treatments. It contains four questions with yes (0) or no (1) answers. The item scores are summed to define three levels of adherence: 0 (high adherence), 1–2 (medium adherence), and 3–4 (low adherence). The questionnaire was designed to obtain a global score per patient. We hypothesised a positive correlation between overall patient adherence by our tool (online supplementary table S2) and the MMAS-4 score.
The TBQ37 aims to assess the workload of healthcare for patients and its impact on quality of life. This scale contains 13 items with an 11-step rating scale ranging from 0 (not a problem) to 10 (big problem) and was designed to obtain a global score per patient. We hypothesised a positive correlation between overall patient adherence by our tool and the TBQ score.37 ,38
Reliability
Reliability of the measurement of adherence at patient level was determined by a test–retest method. Patients completed our instrument at baseline and after 1-month.36 Retest questionnaires were sent by postal mail to patients.
Statistical analysis
Data are described with numbers (percentages) for categorical variables and means (SD) or medians (IQR) for quantitative variables. Agreement between measurement from our tool and drug diaries was assessed by the intraclass correlation coefficient (ICC)28 and considered acceptable at ICC>0.60.28 ,39 The 95% CIs were determined by a bootstrap method. Similarly, the test–retest agreement was assessed using ICC.
To assess construct validity, we used mixed linear models with the identity of the patient taking the drug as a random effect to account for the clustered structure of our data (different drugs taken by the same patient). We considered five models to compare drug adherence level measured with our tool and the Lu questionnaire, the three items from the AE and physicians' evaluations.
Correlations between patient level of adherence obtained with our tool and the MMAS-4 global score or TBQ score were assessed by Spearman correlation coefficient (rs) and considered high at rs>0.5 and moderate at rs=0.35–0.50.40 All statistical tests were two-sided with p<0.05 being considered statistically significant.
To better understand the relationship between drug adherence assessed by our tool and the global score obtained by the MMAS-4, we used a graphical representation. We classified all patients by MMAS-4 score level (low, medium and high) and represented, for each patient, all prescribed drugs coloured according to the six drug adherence levels of our tool.
We used complete case analysis to manage missing data. All statistical analyses involved use of R V.2.13.1 (http://www.r-project.org).
Results
Participants and drugs
From May to August 2014, 243 patients were recruited (median age 59.1 years (IQR 42.5–70.6 years)); 163 (67.1%) were women and 155 (63.8%) were outpatients (table 2). Patients took a total of 961 medications (median 3 (IQR 2–5) per patient), corresponding to 292 distinct drugs. Among the 243 patients who responded to the study questionnaire, all completed our instrument for at least one medication, which allowed us to define drug adherence levels for 913/961 (95.0%) medications. A total of 210 (86.4%) patients completed the instrument for all their medications. Most of the prescribed drugs were cardiac agents, representing 222 (23.1%) drugs. Figure 1 shows the results by different drug classes (see classification detailed in online supplementary table S4).
Demographic and clinical characteristics of patients (n=243)

Drug adherence by different medication classes. Each bar corresponds to a medication class. The width of a bar is proportional to the number of drugs of the class in the study. Colours correspond to drug adherence levels.
Assessment of the measurement properties of the developed tool at the drug level
Validity
A total of 37 patients (39.7% of patients who agreed to complete diaries) returned their 14-day drug diaries. Agreement between adherence measured by our tool and drug diaries was good, with ICC 0.69 (95% CI 0.34 to 0.91) (see online supplementary table S5).
We found a linear relationship between adherence measured by our tool and with the Lu questionnaire (p<0.01). Mean ratings increased from 2.1 (SD 3.8) for discontinued drugs (adherence level 6) to 9.9 (SD 0.8) for drugs for which patients were highly adherent (adherence level 1) (table 3).
Comparison between drug adherence levels obtained by our tool and other measures at the drug level (n=913 drugs)
Drug adherence measured by our tool and measures obtained by the AE were linearly related. The mean AE score about perceived need for medication decreased from 2.5 (SD 2.0) for discontinued drugs to 1.3 (SD 0.8) for drugs for which patients were perfectly adherent (p<0.01) and the mean AE about the score for perceived concerns about medication increased from 4.5 (SD 1.7) for discontinued drugs to 5.1 (SD 1.5) for drugs for which patients were highly adherent (p<0.01). However, we found no significant association with perceived affordability of drugs (p=0.28).
A total of 57 physicians (45% of sent questionnaires) evaluated 501 drugs taken by their patients. Drug adherence measured by our tool and physicians' perception of patient adherence was linearly related (p<0.001). However, physicians rated adherence highly for discontinued drugs (mean score 6.3 (SD 3.2)).
Reliability
Test–retest results were obtained for 53 patients taking a total of 203 drugs. Agreement was good for drug adherence level, with ICC 0.67 (95% CI 0.42 to 0.85) (see online supplementary table S6).
Assessment of the measurement properties of the developed tool at the patient level
Validity
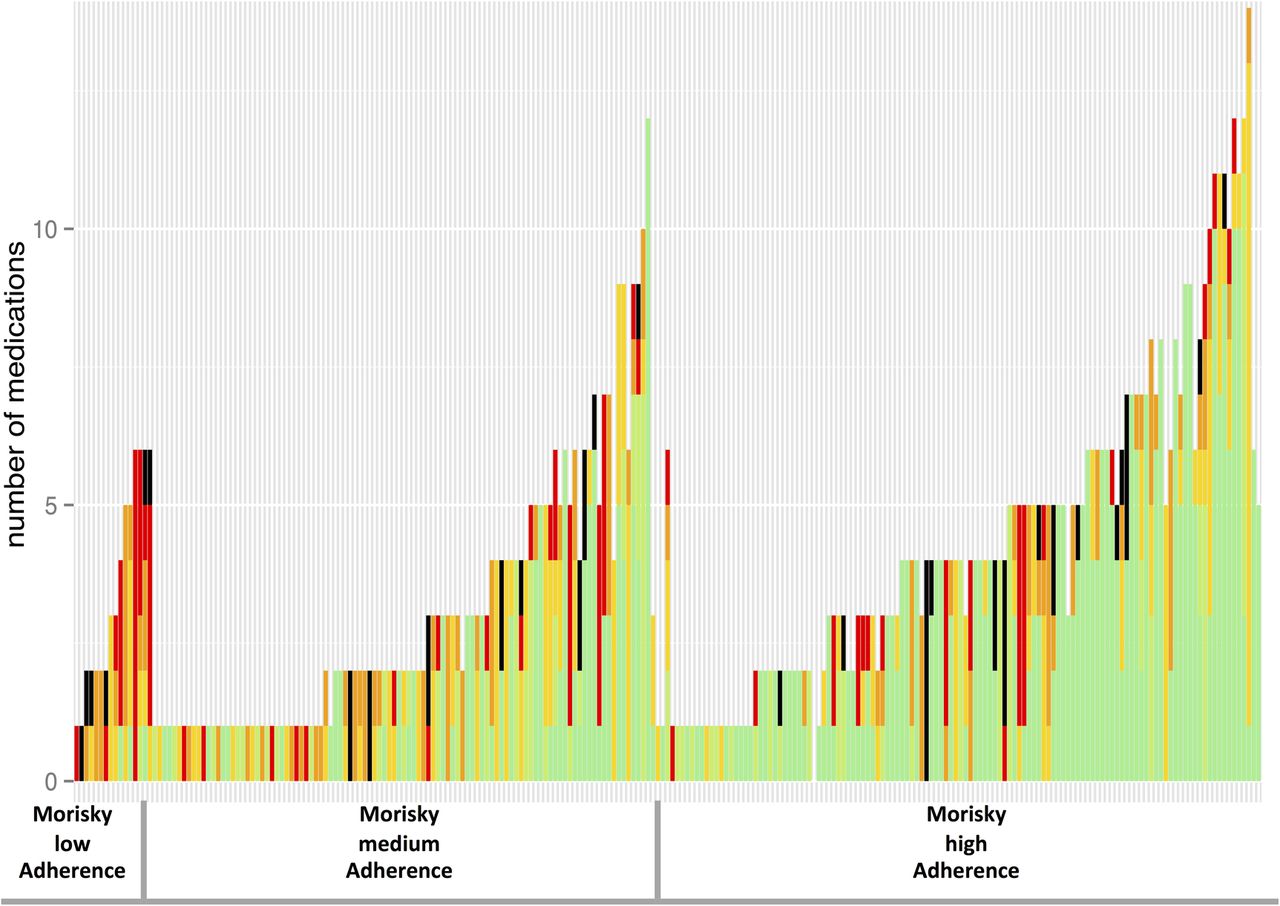
We found a weak correlation between patient adherence levels obtained with our tool and the MMAS-4 score (rs=0.28, p<0.01). We found variability in adherence among the different drugs taken by patients (figure 2): patients could perfectly adhere to one drug and could have discontinued another one. We found a weak correlation between global patient adherence obtained by our tool and TBQ scores (rs=0.32, p<0.01).

{kind=link}
{kind=link}
Drug adherence for each drug taken by the patient according to the Morisky Medication Adherence Scale-4 items (MMAS-4) level. Each bar corresponds to a patient: patients were ordered by the MMAS-4 score and number of prescribed drugs. The height of a bar is proportional to the number of drugs taken by the patient. Colours correspond to drug adherence levels: green, high adherence; light green, good adherence; deep yellow, moderate adherence; orange, poor adherence; red, very poor adherence; black, discontinuation.
Sensitivity analysis exploring different definitions of patient adherence level did not change results as detailed in online supplementary table S7.
Reliability
Test–retest results were obtained for 53 patients taking a total of 203 drugs. Agreement was good for patient adherence levels, with ICC 0.80 (95% CI 0.65 to 0.91).
Discussion
In this study, we developed a new tool providing an accurate assessment of adherence by describing several medicine-taking behaviours (ie, discontinuation, drug holidays, missing doses and schedule errors) for each drug taken by a patient. To the best of our knowledge, this tool is the first to assess adherence for each drug taken by patients and taking into account medicine-taking behaviours. Its response rate suggests good acceptability.
All hypotheses for construct validity were verified, except for the expected relationship between measurement of adherence using our tool and the AE question about affordability of the drug. This result may be explained by the poor suitability of this question for French patients: in France, the national public health insurance programme guarantees healthcare free of charge for patients with chronic conditions.
Measurements of adherence at patient level using our tool were weakly correlated with measures of the MMAS-4. These findings could be related to poor psychometric properties of our tool or variability in adherence among the different drugs taken by patients, as illustrated in figure 2. This is an example of the difficulties encountered when defining adherence at the patient level (eg, considering a patient as ‘adherent’ or ‘non-adherent’ without exploring the differences among different drugs). Measurements of adherence at the patient level using our tool were weakly correlated with measures of the TBQ. This result was expected in part because the TBQ measures burden of treatment globally, including components other than problems with medications.
In the present study, we developed a self-reported instrument to assess adherence. We acknowledge that patient-reported outcomes are more at risk of respondent bias than are other measures of adherence, such as electronic devices. However, they represent the easiest way to assess adherence in routine practice. These different methods are complementary and all have advantages and limits. Use of a given method should be guided by the specific purposes of adherence studies.6 In this study, we did not compare measurements of adherence using our tool with electronic monitoring devices, prescription refill rates or pill counts. Moreover, we did not assess the responsiveness of our instrument which could be explored in future studies.41
The main strength of this study is the large diversified recruitment (inpatients and outpatients with different conditions and various treatment regimens), thus ensuring the suitability of our tool for assessing adherence across any disease or treatment context.
Moreover, our estimates of adherence assessed by our tool at the drug level may be more accurate than those obtained with other tools: indeed, we did not ‘judge’ whether a patient was adherent or not, but we assessed specific behaviours for specific medications with a ‘no-blame’ approach, suggesting to the patient that non-adherence may be the norm or usual. This finding was illustrated by the lower ceiling effect with our tool than with other measures of adherence (Lu's questionnaire, AE, MMAS-4). As a result, asking about different medicine-taking behaviours for each individual prescribed drugs could avoid a rating value judgement and reduce overestimation of self-reported adherence. However, these findings need to be confirmed in other studies.
This study has limitations. First, our tool is not suitable for drugs taken several times a day or irregularly (eg, once a month). Moreover, it does not provide information about occasional change in dosage by the patient or accurate frequency of behaviours. This was a conceptual choice: we preferred to develop a simple and easy-to-use tool usable for studies or daily practice, in which patients could select the answer that best applied to them while minimising the respondent's burden. Second, we collected only names of the prescribed drugs. As a result, our tool does not provide information about pill colour, galenic form or generic drug use, which could have an impact on drug non-adherence.42 ,43 Third, our sample was a convenience sample and was not representative of the population of patients taking long-term treatments, especially in other countries with different healthcare systems. Fourth, only a small sample of patients completed and returned drug diaries, generating wide CIs. This finding suggests poor acceptability of assessment of adherence with drug diaries, which may be too intrusive for routine use. In addition, diaries may be considered as interventions, but this would not have impacted estimates of patient adherence using our tool, as our tool was filled before the diaries were completed. Finally, global patient adherence level was arbitrarily defined. However, we assessed whether different definitions of patient level of adherence affected our results and did not find any change in our findings (online supplementary table S7). It is important to note that our definition of adherence at patient level was mainly for allowing comparisons between our tool and other measurements at patient level. For practice, we recommend using our tool to assess adherence at drug level.
This study may have several clinical implications. First, physicians rated adherence highly for discontinued drugs, which highlights that they were often unaware of how patients managed their different medications. They should be aware of the importance of assessing drug adherence during consultations or prescription refill requests. Second, we found variability in adherence to the different drugs taken by a given patient. Adherence may depend on multiple factors, including the nature/indication of the drug, as suggested by figure 1. These findings support the literature, which has shown that patient adherence is affected by different beliefs and experiences about their medications, conditions and the healthcare system.3 ,44 Physicians caring for patients under long-term treatment should take into account these factors to understand the complexity of medication intake. Asking about different medicine-taking behaviours rather than simply categorising patients as ‘adherent’ or ‘non-adherent’ could avoid value judgements and facilitate patient–physician discussions about medications. More work is needed to implement our instrument in the clinic and to assess its impact on treatment decisions in routine practice.
Conclusion
We developed a new instrument with acceptable validity and reliability to assess drug adherence, providing information about medicine-taking behaviours for patients with long-term therapies and with a new ‘drug-by-drug’ perspective. Our self-reported adherence tool could complement other measurements of treatment adherence in routine practice. We found variability in the different drugs taken by a patient and poor awareness of patient non-adherence by physicians. These findings should encourage physicians to ask about medication-taking during consultations and to assess adherence not globally per patient but rather for each individual drug.
Acknowledgments
The authors thank Caroline Barnes and Cathia Zak for help with questionnaire translation and Laura Smales for reviewing the manuscript before submission. They are particularly indebted to Gerard Reach, Jean-François Bergmann, Virginie Savoldelli and Fabienne Marcellin for sharing their time and expertise during meetings.
References
Footnotes
Contributors SS was involved in the study conception, writing of the manuscript, meeting experts, elaborating the tool, recruiting patients, interpreting results and drafting the manuscript. V-TT and PR were involved in the study conception, elaborating the tool, interpreting results and drafting of the manuscript. CC was involved in elaborating the tool and recruiting patients. EP was involved in statistical analysis. PR is the guarantor.
Funding The study was supported by an academic grant from the programme ‘Equipe espoir de la Recherche’, Fondation pour la Recherche Médicale, Paris, France (number DEQ20101221475).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol was approved by the Institutional Review Board of University Paris Descartes (IRB 0001072).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.