Article Text

Abstract
Objectives To assess cost-effectiveness and cost utility of telerehabilitation (TR) versus standard rehabilitation (SR) after total knee replacement (TKR).
Design Markov decision modelling of cost-effectiveness and cost-utility analysis based on patient-level and secondary data sources employing Italian National Health Service (NHS; Ita-NHS) and Society perspectives.
Setting Primary care units (PCUs) in Italy.
Participants Patients discharged after TKR.
Interventions Mixed SR-TR service (10 face-to-face sessions and 10 telesessions) versus SR (20 face-to-face sessions)
Primary and secondary outcome measures The incremental cost per additional knee flexion range of motion (ROM) and per QALY gained by SR-TR compared with SR. Second, we considered the probability of being cost-effective and the probability of being more effective and less expensive.
Results TR appears to be the cost-effective in the base case and in all of the considered scenarios, but is no longer more effective and less expensive if transportation costs are excluded. Comparing SR-TR with SR, the incremental cost-effectiveness ratio (ICER) adopting the Ita-NHS perspective for the base case was −€117/ROM gained. The cost-effectiveness probability for SR-TR was 0.98 (ceiling ratio: €50/ROM), while the joint probability of being more effective and less expensive was 0.87. Assuming that TR would increase health-related quality of life (HRQOL) utilities by 2.5%, the ICER adopting Ita-NHS perspective is −€960/QALY (cost-effectiveness probability: 1; ceiling ratio: €30 000/QALY). All the performed sensitivity analyses did not change the conclusions, but if transportation costs were excluded, the probability for SR-TR of being more clinically effective and less expensive reduced to 0.56.
Conclusions The analysis suggested SR-TR to be cost-effective, even less expensive and more effective if the PCUs provide ambulance transportations. However, the uncertainty related to TR costs, HRQOL and long-term clinical outcomes raises important topics for future research, which should be addressed to confirm our estimates.
Trial registration number ISRCTN45837371.
- HEALTH ECONOMICS
- REHABILITATION MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study assesses cost-effectiveness and cost-utility for telerehabilitation (TR) after total knee replacement (TKR) and provides the implications of the number of transportation for the primary care units.
The model uses patient-level data for prostheses survival and health-related quality of life (HRQOL) utilities from the largest ever conducted pragmatic randomised controlled trial for TKR.
Effectiveness parameters, HRQOL utilities for TR and the assumptions in costing standard rehabilitation-TR are uncertain and need further investigations.
Introduction
Total knee replacement (TKR) is considered an effective and cost-effective solution to overcome the most common problems in osteoarthritis and rheumatic arthritis.1 ,2 In 11 years, the number of TKRs performed in Italy has more than doubled (27 959 TKR performed in 2001; 63 048 TKR in 2012), and was the 21st most performed procedure in 2012.3 ,4 The overall number of procedures is forecasted to increase further in the next years due to the reduction in average age of the population undergoing TKR and the extension of lifespan.5 Patients are often treated using standard rehabilitation (SR) after the surgery.6 ,7 Owing to the number of procedures undergone each year, TKR and the consequent rehabilitation have a high impact in terms of socioeconomic burden, affecting both costs to the Italian National Healthcare Service (Ita-NHS) and patients.8According to Piscitelli and colleagues, productivity losses for patients who underwent TKR were on average 9 days in 2005. If the time spent in hospital is included, this increases to 20 days.8 In total, TKR patients aged younger than 65 years lost 386 586 days of employment in 2005 or ∼€30 million.9 ,10 In addition, rehabilitation cost for the NHS is around €158 million in 2005 (€47 million for hospital rehabilitation and €111 million for home rehabilitation). However, the current value is expected to be even higher in the next years due to the continuing increase in the number of TKRs performed in Italy.5 Budget allocation for TKR and its related rehabilitation should be considered as a societal issue rather than just as an NHS concern. In the past years, telerehabilitation (TR) has been shown to be non-inferior to usual care.11–14 Although this evidence was reinforced in 2015 with a meta-analysis showing a significant positive effect of TR after TKR,15 and the presence of promising results in terms of costs reduction,16 the actual cost-effectiveness for TR in TKR patients remains unknown. The aim of the present analysis is to assess the cost-effectiveness and cost utility of TR versus standard care after TKR.
Methods
A Markov model was developed to represent the natural progression of the TKR and estimate the cost-effectiveness of a mixed SR-TR programme compared with SR. The treatments assessed in our economic evaluation were as follows:
SR: 20 face-to-face rehabilitation sessions in the following 3 months after TKR.
SR-TR: 10 face-to-face rehabilitation sessions and 10 telesessions delivered in the following 3 months after TKR.
The cost-effectiveness was measured both as incremental cost per knee flexion range of motion (ROM) and as incremental cost per quality-adjusted life year (QALY) and reported as the average of 5000 probabilistic sensitivity analysis (PSA) simulations. The net monetary benefit was calculated and employed to estimate the probability that each programme would be the most cost-effective at different willingness to pay (WTP) for one unit increase in the outcome (ROM or QALY). Additionally, the probability of each strategy was plotted against the WTP threshold to obtain the cost-effectiveness acceptability curve. The costs were estimated using a ‘bottom-up’ approach employing Italian tariffs17 and under the guidance of a panel of experts. The effectiveness parameters used the results of a recent clinical trial13 and patient's level data from a large multicentre UK-based clinical trial.18 Since the average duration of the rehabilitation after TKR is 3 months, we assumed that each set of devices (ie, two sensors and a tablet)19 was shared by three patients during the same year.
Model structure
We employed a previously developed and widely used Markov model.20 Four different states following the first TKR were considered:
Successful TKR,
Revision,
Successful revision,
Death.
Each cycle lasted 1 year; we assumed that each surgery (ie, both TKRs and revisions) required rehabilitation, and that TR influenced neither the probability of having a second surgery nor the health-related quality of life (HRQOL) utilities. The perspectives considered in the model were Ita-NHS and Society. Productivity losses were estimated assuming that face-to-face rehabilitation lasts 1 h,13 excluding transportation time. The human capital approach and the average net income in Italy in 20149 ,10 were used to value the indirect costs. A lifetime time horizon was employed, correcting the estimates with the half cycle method and an annual discount rate of 3% for both costs and outcomes. The surgery, medication and other procedural costs were not included as these would not be expected to differ between postsurgical treatment options.
Transition probabilities
Annual probabilities of death not related to surgery were estimated from the WHO lifetables,21 while mortality due to the surgery was based on the UK National Joint Arthroplasty Registry,22 and was applied to primary TKR and to revisions. The probability of a first revision is time-dependent and was derived from a parametric regression-based survival model using data from a large multicentre UK-based clinical trial.18 According to the Akaike Information Criterion (AIC) statistics, a γ distribution performed better than the other models tested and the predictions were estimated on the basis of: patient's age, gender and any complications (please see online supplementary table S1 for further details). Follow-up in this study was stopped after 9 years and the probability of a first revision beyond this point was based on extrapolations. Since the survival model could underestimate the revision probability after 9 years, different scenarios were explored. We assumed that the probability after 9 years would constantly increase if compared with the previous cycle employing yearly increment coefficients ranging from 2.5% up to 10%. The re-revision rate was obtained from the published literature and was translated into a constant probability.23
Effectiveness of rehabilitation programmes
A recent meta-analysis assessed the clinical effectiveness of TR in recovering the motor function in different populations.15 Agostini et al found that TR after TKR is clinically more effective than usual care. Among the studies cited in Agostini et al's review for TR after TKR,11–13 two out of three used videoconferencing. The only study employing sensors for the TR after TKR was a non-inferiority study,13 using an interactive TR kit. The set of devices comprised two wireless sensors able to capture the knee movement and a touch screen all-in-one computer. The patients undertook half of the sessions under a physiotherapist's supervision and the other half at home. However, the patients enrolled in the trial did not experience any complications. Therefore, to avoid unrealistic matches between patients and clinical outcomes, the following considerations in assigning the outcome rewards were required. The SR arm was supposed to receive exclusive face-to-face rehabilitation, so the clinical outcome of the control group was applied to the patients in the SR arm. The SR-TR arm was further divided into two groups: patients with or without complications. Patients who experienced any complications received only face-to-face rehabilitation sessions; therefore, the control group outcome was assigned to them. On the other hand, the remaining patients in the SR-TR programme did not have any complication and received half of the sessions remotely; consequently, the outcome of the experimental group (ie, TR) was associated with the patients without complications. After clinical expert consultation,24 the selected clinical effectiveness outcome employed in our model was the knee flexion ROM after 3 months of follow-up.
Health-related quality of life
No studies were identified which reported exhaustive results for the HRQOL utilities of patients following a TR programme after TKR. Therefore, we employed the data from a large multicentre UK-based clinical trial (KAT trial)18 to estimate the HRQOL for SR and to predict SR-TR utilities. This was based on the EuroQol five dimensions (EQ-5D) questionnaire, a five dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and three levels (no problems, some problems or severe problems) instrument.25 The responses were translated into a numeric scale using UK weights26 ranging from 1 (full health) to −0.6 (health states worse than death), and 0 is equivalent to death. The HRQOL utilities were calculated before and 1 year after any surgery. Since the available studies for TR after TKR suggested SR-TR to be at least not inferior to usual care,14 ,15 we assumed SR-TR to not influence HRQOL. However, to further explore the impact of our assumption, we performed a two-way sensitivity analysis to consider different scenarios—please see the ‘Sensitivity analyses’ section for further details. Ordinary least squares and Tobit models were used to estimate the utilities using the following explanatory variables: patient's age, gender, any complication and type of surgery (ie, first TKR or revision; please see online supplementary table S2 for further details). The HRQOL decrement was not assessed as we assumed utilities would not be influenced by TR, and it would have the same impact on both arms of the model.
Supplementary tables
Costs
On the basis of the model assumptions and the perspectives adopted, direct and indirect cost units are summarised in table 1. Direct costs were limited to the Italian tariffs for the ambulatory rehabilitation (year 2013)17 and the ambulance transportation (year 2008)27 for the SR programme. The SR-TR programme relied on the Italian tariffs for rehabilitation and transportation for the 10 face-to-face sessions, while the cost related to the 10 telesessions was based on opinions from a panel of experts in the clinical and Telco areas. Finally, the costs were inflated to 2008 and 2013 euros.28 The cost of TR was broken down into: hardware, server, internet and telesessions cost. Since there is no comprehensive information on cost of TR after TKR, data were obtained from expert opinions. Hardware cost was elicited from the engineers of the REal-TIme System laboratory (ReTIS—Sant'Anna School of Advanced Studies) and the lifetime of the devices was estimated to be 3 years. Likewise, the expert advisory group from an Italian Telco provided costs for the server and for the internet connection. According to directors of the rehabilitation units across ‘Area Vasta Nord-Ovest’ in Tuscany, telesessions cost was estimated assuming the medical personnel cost to be halved.24 Productivity lost was measured considering the average duration of a face-to-face rehabilitation session.13 Monetisation of indirect cost was performed using the human capital approach and was limited to patients younger than 70 years (maximum pensionable age in Italy).
Parameter values employed in the Markov model
Sensitivity analysis
To reflect the uncertainty in parameters, each PSA simulation uses randomly selected values for the transition probabilities, the costs, the clinical outcome, the utilities and the number of rehabilitation sessions. For those parameters without any information available on the variation of the mean, the PSA assumed an SE equal to 40% of the mean.30 The probabilistic values for costs and transition probabilities were obtained using γ and β probability distributions, respectively, while both the clinical outcome and the number of rehabilitation sessions used normal distributions. The Cholesky decomposition method was used to represent uncertainty in the regression models for HRQOL and prostheses survival analysis.
One-way sensitivity analysis was employed to estimate the variation of the cost-effectiveness results according to the changes in assumptions and single parameters. Furthermore, a two-way sensitivity analysis was performed to calculate the incremental cost-effectiveness ratio (ICER), the cost-effectiveness probability and the probability of being more effective and less costly varying HRQOL assumptions and the number of ambulance transportation.
This economic evaluation was developed following the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guidelines.31
All the analyses were performed with Excel V.2013 (Microsoft Corporation, USA) and with STATA V.12 (StataCorp LP, USA).
Results
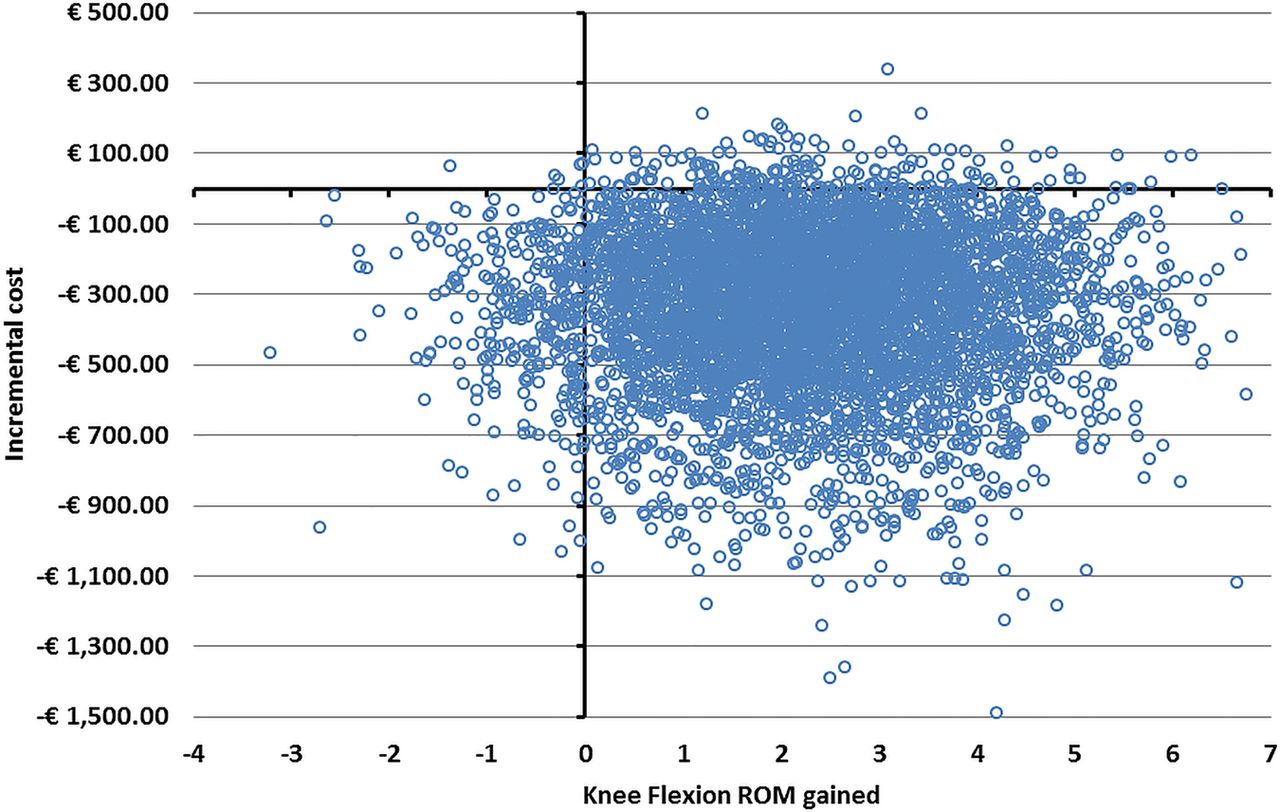
To assess the lifetime costs and effectiveness of SR-TR and SR, we employed a cohort of 1000 patients with the KAT trial sample features (44% males, 19% experienced complications during or after the surgery). However, an average age of 60 years rather than 70 years was used to consider the reduction in the average age of the TKR patients in the next years.5 Additionally, the number of ambulance transportations was assumed to be 25% of the number of face-to-face rehabilitation sessions (eg, five round trips over 20 sessions for SR and three round trips over 10 face-to-face sessions for SR-TR). Table 2 reports the lifetime HRQOL, clinical outcome and cost results according to the payer perspectives and the percentage of the ambulance transportations reimbursed out of the number of face-to-face sessions. When compared with SR, the incremental cost per ROM gained for SR-TR ranges from −€117 (Ita-NHS perspective) to −€152 (Society perspective; table 3). Figures 1 and 2 present the PSA results for both perspectives plotted along the cost-effectiveness plane. Employing the base-case cohort, most of the simulations were located below a €50/ROM threshold, leading to a 98% probability for SR-TR of being cost-effective. Likewise, the joint probability for TR being less expensive and more clinically effective against SR was 86% for the base case. Since the number of reimbursed ambulance round trips varies across the different primary care units (PCU), figures 3 and 4 show the cost-effectiveness acceptability curves reducing the provided number of ambulance transportations from all to none of the face-to-face rehabilitation sessions. Results were not affected by the number of ambulance round trips: the probability of being cost-effectiveness ranged from 83% (no ambulance transportation) to 100% (all rehabilitation sessions) at a threshold of €50/ROM. The QALYs gained for the base-case cohort in the SR arm were 13.02; assuming the HRQOL experienced by the patients involved in the SR-TR programme to be equivalent to those involved in SR, the average lifetime saving was €338 per patient. Table 4 reports in full detail the cost-utility analysis results.
Base-case discounted lifetime: costs, clinical outcome and QALYs according to transportation scenarios and payer perspectives
Base-case and one-way sensitivity analyses
Two-way sensitivity analysis according to the SR-TR effect on HRQOL, number of transportations reimbursed and payer perspective

Results of probabilistic sensitivity analysis for the base case, adopting the Italian NHS perspective. NHS, National Health Service; ROM, range of motion.

Results of probabilistic sensitivity analysis for the base case, adopting the Society perspective. ROM, range of motion.

Cost-effectiveness acceptability curves for the base-case economic analysis according to the number of reimbursed transportations and adopting the Italian NHS perspective. NHS, National Health Service; SR, standard rehabilitation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves for base-case economic analysis according to the number of reimbursed transportations and employing the Society perspective. NHS, National Health Service; SR, standard rehabilitation.
Sensitivity analyses
Table 3 reports one-way sensitivity analyses results. Employing the reference cohort and increasing the number of patients experiencing complications, the ICERs decrease up to a saving of €122 per ROM. Running the model increasing the value for the sensors cost, for the average age at operation or applying any Telco fee per patient for the service, reduced the probability for SR-TR of being cost-effective. Nevertheless, table 3 showed that the lowest probability of being cost-effective is 83% (no transportation), while the lowest value for the joint probability for SR-TR of being less expensive and more effective is 56% (no transportation). Table 4 shows the results for the two-way sensitivity analysis, matching the changes in HRQOL utilities to the percentage of the ambulance transportations reimbursed out of the number of face-to-face sessions. Although TR is clearly cost-effective if SR-TR is not inferior to SR and the maximum WTP is €30 000/QALY, the lowest ceiling ratio necessary to ensure 100% of cost-effectiveness probability is largely lower. In this sense, if the utilities of the patients treated with TR were increased by 2.5%, the ceiling ratio ranges from €600/QALY (10 transportation) to €3000/QALY (no transportation).
Discussion
This study explored the cost-effectiveness and cost-utility of TR compared with standard care following TKR. We used a decision model to assess and forecast the lifetime costs, clinical and HRQOL effects of a mixed SR and TR programme against usual care. The results of the base-case analysis suggested SR-TR is highly cost-effective independently from the perspective adopted. Since the number of the reimbursed ambulance transports changes across the PCUs, both results for cost-effectiveness and cost-utility analysis were reported considering all the possible scenarios (ie, ambulance transportation between none and all face-to-face rehabilitation sessions). Reducing the number of transportations decreased the cost-effectiveness probability; however, even if transportation costs were excluded, SR-TR was still a cost-effective alternative to usual care. One-way sensitivity analyses showed that the results of the model were robust to variations in each parameter. The cost of sensors was the parameter with the greatest impact on cost-effectiveness after the number of ambulance transportations provided. Increasing the cost of the sensors increased the ICER from −€117/ROM for the base case (ie, sensors cost: €100) to −€64/ROM (ie, sensors cost: €500), leading to a reduction in the cost-effectiveness probability from 98% to 90%. Cost-utility analysis was performed using the utilities belonging to patients accessing the SR protocol18 and the base-case scenario assumed no changes in HRQOL for SR-TR patients. If TR is at least non-inferior to SR, the current analysis suggests that SR-TR would be highly cost-effective. Nonetheless, the recently released Italian guidelines for telemedicine declared that the assessed programmes would be implemented if the effectiveness is equal or superior to usual care and the cost is equal or lower.32 Out of the parameters involved in the sensitivity analyses, we considered paying a fee ranging from €30 to €100 to the potential service provider. Even in the worst-case scenario, the probability of SR-TR being less costly and more effective is high (probability: 74%). The current analysis showed that TR is clinically more effective and less expensive for all the considered scenarios, but if the transportation is not reimbursed by the PCU, choosing between SR-TR and SR would be almost indifferent (ie, probability of being more effective and less costly: 56%). The authors of the clinical trials assessing TR after TKR justified remote rehabilitation being more effective than usual care due to the increased intensity of the treatment.11–15 Our results showed that TR could curb spending on healthcare mainly because of reduced transportation costs. This could restrict the adoption of SR-TR to those PCUs providing transportation for rehabilitation after TKR and requiring further investigation on the WTP for those PCUs not providing ambulance service.
Whereas a cost-analysis for TR after TKR was published recently,16 no exhaustive cost-effectiveness or cost-utility analyses have been undertaken at the time of our evaluation. Tousignant and colleagues documented the costs for in-home TR after total knee arthroplasty based on a previous clinical trial. The main finding of the analysis was that the cost for the TR arm was significantly less than for the control group.16 TR on average led to save $C263, 95% CI −$C382 to −$C143 (ie, €186, 95% CI −€270 to −€101), reducing the expenditure by 18%. Not surprisingly, the most important item of cost was the travelling expenditure, which accounted for 49% of the total cost. However, the transportation cost reduction for the TR arm was significant if the distance between the healthcare centre and the patient's house was >30 km. Our results—a saving of €230 per patient—agree with Tousignant and collegues’ estimates; however, some elements should be taken into account. Beyond the differences due to cross-country comparison, Tousignant and colleagues’ estimates employed a different treatment scheme, technical equipment and time horizon. Our cost-effectiveness analysis considered outpatient physiotherapy—the patients’ travel to the PCUs by ambulance—while Tousignant and colleagues considered home visits—the physiotherapists’ travel from the healthcare units to patients' homes. Second, the equipment used in Tousignant and colleagues’ paper was a videoconferencing system (equipment cost: €12 960), while the current work relies on a kit composed of two sensors and one tablet (equipment cost: €260). Finally, our study adopted a lifetime horizon, while Tousignant and collegues focused on the first 4 months after discharge only.
There are a number of limitations associated with this study. Decision modelling involves assumptions and simplifications, and cannot perfectly reflect actual clinical practice. The dispersion parameters for some items involved in our analysis (eg, rehabilitation tariffs, transportation costs) were not available, reducing the accuracy of our analysis. However, if any information was not available on variance of the employed parameters, we applied a coefficient of variation of 40%,30 which in some cases could be an overestimate of the uncertainty. Another limitation that should be taken into account is the potential selection bias for the trial providing the clinical outcome.13 Piqueras and colleagues excluded the patients who experienced any complication. Therefore, the validity of our results was preserved, assigning the TR outcome exclusively to the patients with a positive prognosis. This led to assigning the SR outcome reward to patients with complications, perhaps leading to an overestimate of their ROM. Furthermore, the study focused on a specific provision and operation of the outpatient physiotherapy service that might limit the generalisability of our results. First, the only mode of transport considered was the ambulance, while in a real setting private cars and minibuses could also be used. Moreover, the transportation tariff was assumed to be the lowest possible one and the travelling time was not considered in the productivity loss, thereby underestimating these costs. Second, the study assessed only physiotherapy delivered in hospitals because of the lack of clinical data for other rehabilitation pathways for TR. In addition, physiotherapists in a hospital gym setting usually monitor and instruct many patients simultaneously; this could also be possible employing TR, but perhaps it would be more time consuming, thereby leading to higher medical personnel costs. Even though assumptions are necessary for decision modelling, some of them could not reflect reality; this raises questions that should be addressed in future research developing ad hoc studies.
Given the innovativeness of the treatment, Italian telemedicine guidelines32 stated that tariffs for telemedicine should be comparable to those for the available usual care services. However, TR could lead to an increase in the efficiency of delivering treatment by reducing the effort of the physiotherapist. These performance issues should be taken into account in the tariffs definition. Likewise, Agostini et al15 found a significant positive effect for TR against SR; however, further clinical long-term effectiveness evidences are required to confirm the results. In this sense, HRQOL and prosthesis survival studies for TR after TKR ought to be developed to improve the robustness of our estimates.
Our paper has important implications for the healthcare services since the number of TKR performed across Europe has increased dramatically in the past decade. The growth rate varies across the European countries; for instance, if France faced an increment in the TKR performed between 2000 and 2012 by 80%, in Denmark the number of knee prostheses implanted has more than tripled in the same period.33 The metrics for Italy and the UK appear comparable to this picture, with the number of TKR increasing from 27 959 to 63 048 (2001–2012)3 and from 13 517 to 82 267 (2003–2013), respectively.22
These statistics probably reflect the number of knee rehabilitations performed across Europe, suggesting that physiotherapy after TKR has an impact on the healthcare budgets. Evidence showed telerehabilitation could be a cost-effective programme, and less costly and more effective if transportation is provided by PCUs. Likewise, considering productivity lost would reinforce our results, justifying TR adoption. Another interesting point is that the increased efficiency could reduce the time necessary to treat patients accessing the TR programme. If this reduction will be demonstrated, TR could allow the reallocation of resources to other disease areas or to patients with a worse prognosis. Despite the difficulties in telemedicine diffusion in Italy, in the past 5 years there was an increasing interest from the Italian Ministry of Health for telecare.34 This led to define the telemedicine guidelines, practically setting the basis for redesigning the Ita-NHS and integrate e-health programmes within it.32 Even though further research is needed to validate our results, TR after TKR has been shown to be able to curb spending in healthcare and to improve clinical outcomes in the short term.
Acknowledgments
The authors would like to thank: Dr Helen Campbell for the enlightening conversation during the model development, the KAT trial study group for permitting access to the data, and Dr Helen Dakin and Professor Alastair Gray in particular for the data preparation and the valuable support. They would also like to thank Mr Seamus Kent for the comments and the help to improve the manuscript, the Telecom Italia engineers from the Wellbeing Health Innovative Technologies (WHITE) Joint Open Laboratory (Telecom Italia) and the decision-makers from the Tuscany ‘Area-Vasta Nord-Ovest’ for their opinions for the model assumptions. The authors also thank Telecom Italia, which funded his PhD scholarship.
References
Footnotes
Contributors FF developed the Markov model, performed the statistical analysis and drafted the paper. GT was responsible for conception and design. All authors contributed to the final draft/paper.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.