Article Text

Abstract
Objectives To identify predictors of mortality within 1 year after primary surgery for ovarian cancer.
Design Prospective nationwide cohort study from 1 January 2005 to 31 December 2012.
Setting Evaluation of data from the Danish Gynaecology Cancer Database and the Danish Civil Registration System.
Participants 2654 women who underwent surgery due to a diagnosis of primary ovarian cancer.
Outcome measures Overall survival and predictors of mortality within 0–180 and 181–360 days after the primary surgery. Examined predictors were age, preoperative American Society of Anesthesiologists (ASA) score, body mass index (BMI), International Federation of Gynaecology and Obstetrics (FIGO) stage, residual tumour tissue after surgery, perioperative blood transfusion and calendar year of surgery.
Results The overall 1-year survival was 84%. Within 0–180 days after surgery, the 3 most important predictors of mortality from the multivariable model were residual tumour tissue >2 cm versus no residual tumour (HR=4.58 (95% CI 3.20 to 6.59)), residual tumour tissue ≤2 cm versus no residual tumour (HR=2.50 (95% CI 1.63 to 3.82)) and age >64 years versus age ≤64 years (HR=2.33 (95% CI 1.69 to 3.21)). Within 181–360 days after surgery, FIGO stages III–IV versus I–II (HR=2.81 (95% CI 1.75 to 4.50)), BMI<18.5 vs 18.5–25 kg/m2 (HR=2.08 (95% CI 1.18 to 3.66)) and residual tumour tissue >2 cm versus no residual tumour (HR=1.84 (95% CI 1.25 to 2.70)) were the 3 most important predictors.
Conclusions The most important predictors of mortality within 1 year after surgery were residual tumour tissue (0–180 days after surgery) and advanced FIGO stage (181–360 days after surgery). However, our results suggest that the surgeon should not just aim at radical surgery, but also pay special attention to comorbidity, nutritional state, age >64 years and the need for perioperative blood transfusion.
- Ovarian cancer
- SURGERY
- Mortality
- Predictors
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a population-based study on 2654 women with prospective registered data.
We used data sources of high quality and there was no loss to follow-up.
Adjustment for multiple factors was made: age, preoperative health score, body mass index, International Federation of Gynaecology and Obstetrics (FIGO) stage, residual tumour tissue after surgery, perioperative blood transfusion.
We were unable to perform analyses regarding neoadjuvant chemotherapy prior to surgery.
There were missing data on smoking, alcohol, laboratory data and specific cause of death.
Introduction
Five-year survival is a traditional measure of the survival of patients with cancer. The majority (70–80%) of women with ovarian cancer are diagnosed in advanced stages,1 ,2 with a median survival of approximately 2 years,3 and we may therefore overlook important factors for survival by primarily focusing on long-term survival. Ovarian cancer has a high mortality,4 and we need to focus on additional areas of prognostic importance in order to improve the outcome.
Previous studies of the survival of women with ovarian cancer have focused on mortality within the first 30–60 days after surgery or on long-term survival. These studies have identified commonplace predictors of mortality (ie, complications to surgery, FIGO stage and residual tumour tissue5). To the best of our knowledge, no former studies have focused on predictors of mortality within 1 year after primary ovarian cancer surgery. However, we hypothesised that analysing the intermediate survival of women (up to 1 year after surgery) would provide valuable information on potentially significant factors for survival. If this hypothesis proves correct, these factors should be considered in the perioperative settings and are useful in the counselling of the patient. Using data from the nationwide Danish Gynaecology Cancer Database (DGCD) obtained from 2005 to 2012, and the Danish Civil Registration System (CPR registry), the aims were to examine predictors of mortality within 0–180 and 181–360 days after primary ovarian cancer surgery. The examined predictors of mortality were age, preoperative American Society of Anaesthesiologists (ASA) score,6 smoking, body mass index (BMI), International Federation of Gynaecology and Obstetrics (FIGO) stage, residual tumour tissue after surgery, perioperative blood transfusion and calendar year of surgery.
Materials and methods
Study population
The study includes all Danish women who had undergone primary ovarian cancer surgery performed from 1 January 2005 to 31 December 2012 and who were identified in the DGCD. The DGCD is a national clinical database established on 1 January 2005,7 and since then all patients with a first-time diagnosis of ovarian cancer have been prospectively registered. This was based on mandatory reports from all Danish departments of gynaecology and histopathology. The DGCD contains details about preoperative patient characteristics (ie, age, ASA score, smoking and BMI), perioperative information (ie, FIGO stage, residual tumour tissue after surgery, blood transfusion, etc) and postoperative details (ie, histopathology, final tumour stage verification, complications and adjuvant chemotherapy).
The ovarian cancer data in the DGCD have previously been validated and the registry was concluded to be valuable for quality monitoring in gynaecological oncology.8 Each patient is identified by a unique 10-digit number given to all Danish citizens by the CPR registry at birth or when residence permits are obtained.9
The DGCD included 2831 women who had primary ovarian cancer surgery during the study period. The following were exclusion criteria: (1) a preoperative ASA score obtained >6 months before surgery (n=119), presuming 6 months to be the maximum time period to surgery if neoadjuvant chemotherapy had been administrated, and (2) a histopathology requisition completed later than 2 weeks after surgery (n=58), signifying that the specific pathology requisition most certainly originates from the current surgery. The CPR registry provided information on overall survival.
Data on predictive variables
From the DGCD, we specifically obtained data on age at the time of surgery, preoperative ASA score6 (indicating comorbidity at the time of surgery), preoperative BMI,10 preoperative smoking habits, FIGO stage,11 size of residual tumour tissue after surgery (visually evaluated by the surgeon at the end of surgery), perioperative blood transfusion and calendar year of surgery. We also received data on alcohol consumption, but due to several missing pieces of data, this parameter was omitted from further analyses. All the aforementioned parameters, apart from alcohol, were evaluated as predictors of mortality.
Age: The women were divided into two groups according to the median age: (1) age ≤64 years and (2) age >64 years at the time of surgery.
ASA score: All women were divided into two groups by the anaesthetists depending on the preoperative ASA score: (1) ASA score=1 (without comorbidity) and (2) ASA score >1 (with comorbidity).
Smoking: At the preoperative interview, women were divided into two groups according to the current smoking status: (1) non-smokers and (2) smokers.
BMI: Usually, BMI is divided into the following groups: underweight, normal, overweight and obese, but in our study population only a small group of women had BMI≥30 kg/m2. Therefore, all women were assigned into three groups according to BMI: (1) BMI<18.5 kg/m2 (underweight), (2) BMI 18.5–25 kg/m2 (normal) and (3) BMI>25 kg/m2 (overweight).
FIGO stage: The women were divided into two groups: (1) FIGO stages I and II (localised disease), and (2) FIGO stages III and IV (advanced disease).
Residual tumour: The size of the residual tumour was evaluated by the surgeon at the end of surgery, thereby forming three groups: (1) no residual tumour, (2) residual tumour ≤2 cm and (3) residual tumour >2 cm.
Blood transfusion: The women were grouped in two ways: (1) those who did not receive perioperative blood transfusion and (2) those who did.
Statistical analysis
The overall survival was illustrated by Kaplan-Meier plots of each of the following variables: age (≤64 and >64 years), ASA score (1 and >1), smoking (no, yes), BMI (underweight, normal, overweight), FIGO stage (localised, advanced), residual tumour tissue after surgery (none, ≤2 and >2 cm) and perioperative blood transfusion (no, yes). Predictive variables of interests were assessed descriptively according to death within 0–180 and 181–360 days after surgery. To estimate the time-varying effect of the predictive variables on survival within the two time periods (0–180 and 181–360 days after surgery), we used an extended Cox model.12 Included variables followed the aforementioned categorisation, and the calendar year of surgery was included as a continuous variable. Since missing data concerning smoking were observed not to be random, the estimates obtained for this variable may be biased. Accordingly, if there is any interaction between this variable and other covariates, estimates of other covariates may also be biased. Omitting smoking from the model did not substantially change the estimates of the other variables, and thus the final model was reduced on the basis of the results of the Wald tests. The final model included the following variables: age, ASA score, BMI, FIGO stage, residual tumour tissue after surgery, perioperative blood transfusion and calendar year. After applying the model, we tested whether there is a significant difference for each predictor variable between the two time periods by performing a Wald test. The results of the extended Cox model were reported by the HR and 95% CIs and the Wald test with the p values.
All analyses were conducted using Stata V.12 software (StataCorp LP, College Station, Texas, USA).
According to Danish law, ethical approval and patient consent are not required for purely registry-based studies.
Results
Our study included 2654 women who underwent surgery after a diagnosis of primary ovarian cancer from 1 January 2005 to 31 December 2012. The majority of these women were characterised by age ≤64 years (52%), preoperative ASA score >1 (61%), normal BMI (52%), advanced FIGO stage (63%), radical surgery (68%) and no perioperative blood transfusion (75%; table 1). The overall 1-year survival was 84%. A total of 412 women (16%) died within the first postoperative year. Women who died after surgery (both within 0–180 and 181–360 days) were predominantly characterised by age >64 years, ASA score >1 and advanced FIGO stage. For further descriptive details, see table 1.
Descriptive characteristics according to death up to 360 days after primary ovarian cancer surgery in Danish women performed from 2005 to 2012 (percentage distribution in brackets)
Survival
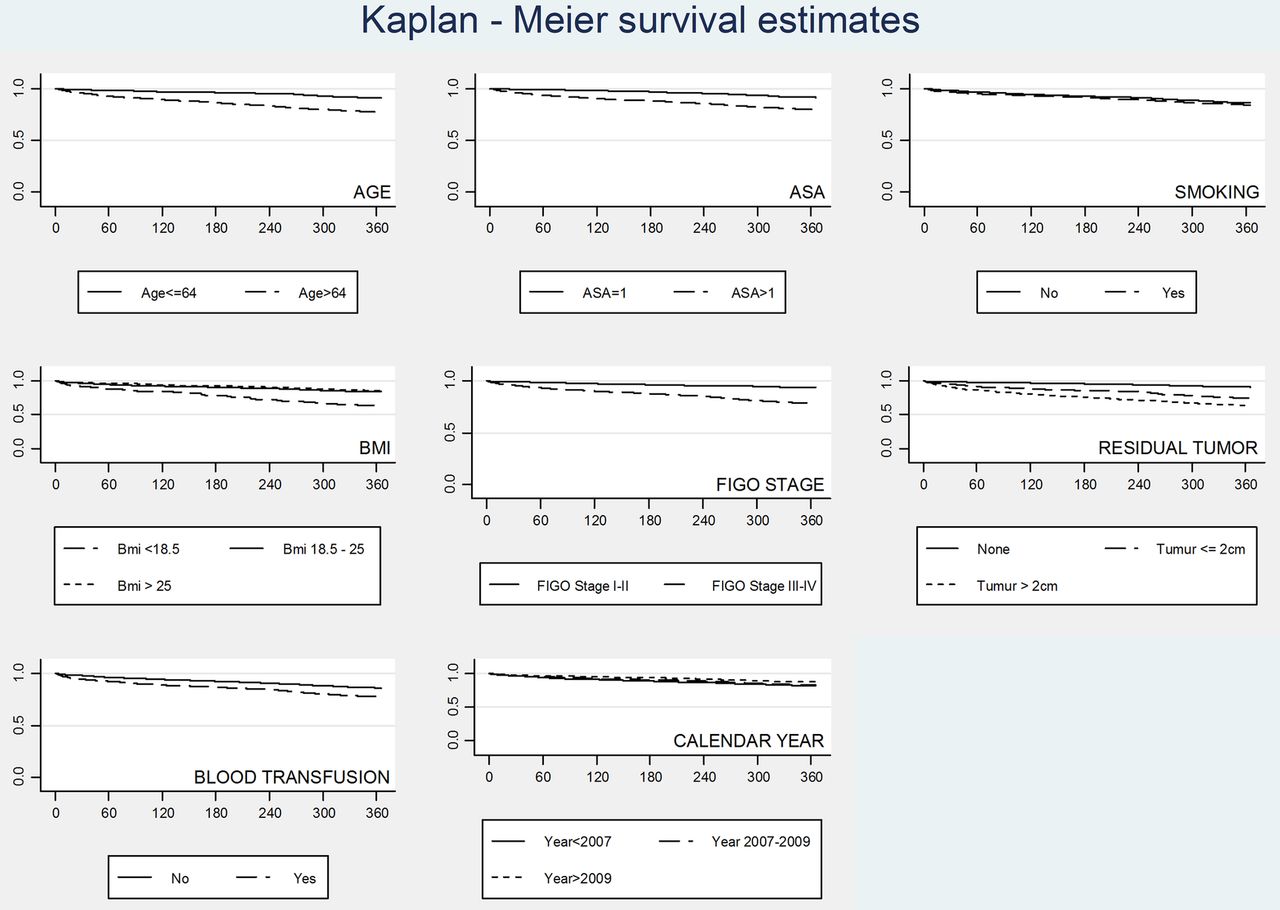
The Kaplan-Meier figures show the separate effect of the included predictive variables on survival up to 360 days after surgery (figure 1). The figures illustrate a decreased survival in women >64 years compared with women ≤64 years, in women with ASA score >1 compared with ASA=1, in underweight women compared with overweight and normal weight women, in women with advanced FIGO stage compared with localised FIGO stage, in women with >2 cm residual tumour tissue left at surgery compared with ≤2 cm and no residual tumour tissue, respectively, and in women who received perioperative blood transfusion in comparison to no transfusion.

{kind=link}
The Kaplan-Meier survival estimates on possible predictive variables in Danish women within the first year after primary ovarian cancer surgery (2005–2012), with the X-axis indicating days after surgery and the Y-axis indicating the survival proportion in percentage. ASA, American Society of Anesthesiologists; BMI, body mass index; FIGO, International Federation of Gynaecology and Obstetrics.
Predictors on mortality
Table 2 shows the results of the multivariable Cox regression analysis and the included variables were thus mutually adjusted in the model. Age >64 years had a statistically significant negative impact on mortality both within 0–180 and 181–360 days after surgery. Using age as a continuous variable did not change the effect of the other variables. ASA score ≥1 had a statistically significant negative impact on mortality only within 0–180 days after surgery. The magnitude of the effect of ASA score ≥1 decreased significantly during time with HR=2.17 (95% CI 1.46 to 3.23) within 0–180 days after surgery to HR=1.25 (95% CI 0.88 to 1.76) within 181–360 days. Being underweight increased mortality in both time periods compared with normal weighted women with HR=2.01 (95% CI 1.29 to 3.07) and HR=2.08 (95% CI 1.18 to 3.66) within 0–180 and 181–360 days after surgery, respectively. Advanced FIGO stage only had a statistically significant effect within 181–360 days after surgery (HR=2.81 (95% CI 1.75 to 4.50)). Residual tumour ≤2 and >2 cm significantly decreased survival in both time periods after surgery, with the most pronounced effect for residual tumour >2 cm within 0–180 days after surgery (HR=4.58 (95% CI 3.20 to 6.59)). The impact of residual tumour >2 cm was still present after 6 months. Perioperative blood transfusion significantly increased mortality in the period 0–180 days after surgery (HR=1.62 (95% CI 1.21 to 2.16)). In the model, calendar year of surgery did not affect mortality, but it was nearly significant within the first 6 months.
Results from the Cox multivariable regression analyses estimating the impact of possible predictive variables on mortality after primary ovarian cancer surgery in Danish women from 2005 to 2012
Some interaction exists between residual tumour and FIGO stage, but this did not change the overall conclusions.
Discussion
Predictors of the ovarian cancer mortality within the first year after surgery have not been intensively investigated. However, focusing only on the perioperative mortality and the 5-year survival may result in overlooking factors important for the survival of the patient. This study examined predictors of mortality within 0–180 and 181–360 days after primary ovarian cancer surgery. Within 0–180 days after surgery, the three most important predictors of mortality were residual tumour >2 cm, followed by residual tumour ≤2 cm and age >64 years. Within 181–360 days after surgery, advanced FIGO stage, underweight and residual tumour tissue >2 cm were the three most important predictors of mortality. Less important, but still statistically significant predictors of survival in the first 6 months after surgery, were ASA>1 and perioperative blood transfusion. Underweight women had a significantly increased mortality within the first postoperative year.
Our study has several strengths; it is based on nationwide prospective registered data, it includes several important predictive variables for mortality and no women were lost at follow-up due to complete information during the entire study period. The validity of data in the DGCD is essential for our results, and the database has previously been successfully validated on primary epithelial ovarian cancer by a comparison of the surgical and histopathological data in the registry with the corresponding medical file and the National Registry of Patients as reference.8
We observed that residual tumour tissue (both <2 and >2 cm) left at surgery has a statistically significant negative effect on survival in both periods after surgery. This finding has been outlined in many other studies,13–15 but our results indicate that a residual tumour of >2 cm is the most important predictor of death within the first 6 months after surgery. The present results and other studies unambiguously identify macroscopic tumour tissue resection as an important surgical issue in improving survival.16–18
We were unable to identify women treated with neoadjuvant chemotherapy prior to surgery due to absent data throughout the entire study period. Since preoperative neoadjuvant chemotherapy is mainly administered to women with advanced FIGO stages, in combination with the possible underestimation of residual tumour tissue at surgery following neoadjuvant chemotherapy,15 our results may be underestimated due to the possible blend of women with different characteristics. However, since neoadjuvant chemotherapy is only administered at advanced FIGO stages, it is unlikely that our strongest predictor of mortality (residual tumour tissue) within 1 year after surgery is biased, and our main conclusion of this study remains unchanged.
We also observed advanced FIGO stage to be an important predictor of mortality, but mainly within 181–360 days after surgery. The negative impact of advanced FIGO stage on mortality is well known and has been described in other investigations,16–18 but the negative effect on mortality within the first year after surgery has not been reported previously. We observed underweight to be a predictor of mortality both 0–180 and 181–360 days after surgery. In contrast, Skírnisdóttir and Sorbe19 concluded that BMI did not influence survival when evaluating women with low-stage ovarian cancer. As in our study, Skírnisdóttir and Sorbe used the BMI reported at the time of surgery, but they did not evaluate its influence on survival until 19–214 months later. Therefore, for the first time, we report the negative effect of being underweight on mortality within the first postoperative year. Malnutrition and ascites are well-known problems among patients with ovarian cancer.20 ,21 Owing to the frequent concomitant presence of ascites, the real preoperative BMI may be lower than measured and the negative influence exerted by underweight is thereby underestimated in our analyses. In a recent study, Ataseven et al22 observed low preoperative albumin to be an independent predictor for severe postoperative complications, and to be independently associated with reduced overall survival. We did not have information of serum albumin, which could have qualified the measurement of nutritional status. Body composition CT scan may even be superior to serum albumin when nutritional status prior to surgery is evaluated, as low subcutaneous fat as well as low muscular fat both have been shown to be independent predictors of mortality.23 We did not, however, have any such measures.
In our study, women >64 years demonstrated poorer survival in comparison to women ≤64 years in the first year after surgery, with the most pronounced impact of older age on mortality observed 0–180 days after surgery and thereafter exceeded by more important factors. In several countries, the relative 1-year and 5-year survival of women diagnosed with ovarian cancer have previously been reported to decrease with old age.24–26 However, to the best of our knowledge, the fact that the impact of old age occurs mainly in the first period after surgery is new information. Jørgensen et al,27 Trillsch et al28 and Sabatier et al29 noted that old women with ovarian cancer may demonstrate worse survival due to potentially inferior treatment, but our data do not include information to illuminate this aspect.
We found comorbidity (ASA>1) as a predictor of mortality, but only at 0–180 days after surgery, and with a decreasing importance over time. Grann et al30 and Sperling et al31 also observed comorbidity to be a predictor of mortality. However, in contrast to our results, they did not evaluate the effect on the immediate postoperative time period, but evaluated data after 1 year (Grann et al30 and Sperling et al31) and 5 years (Grann et al30). Consequently, our data also offer new information in this field and may indicate that reduction of any pre-existing comorbidity could be important in the increasing survival after primary ovarian cancer surgery.
Perioperative blood transfusion was observed to be a predictor of mortality 0–180 days after surgery. This is a new finding in women with ovarian cancer, but a negative effect of blood transfusion on survival has been described in other diseases.32 ,33 Among patients with gynaecological cancer, transfusion has been described to be associated with higher morbidity and increased mortality within the immediate 30 days after surgery, when controlling for parameters such as age, comorbidity, pre-existing anaemia, type of surgery, etc.34 Immune modulatory mechanisms are suggested to induce the aforementioned complications.35 Since the DGCD does not contain information on haemoglobin levels or total transfused blood units, we were unable to evaluate any possible influence of these parameters. Our findings might indicate that perioperative blood transfusion should only be prescribed to a very restricted group of patients, although this aspect needs to be studied in more detail.
Our study also has limitations. According to the incident numbers of Danish patients with ovarian cancer (2005–2012),36 a total of 86–92% had primary ovarian cancer surgery performed;7 however, only 67% of the operated patients were eligible for evaluation in our study. Missing information on smoking and alcohol prevented examination of the impact on survival. As discussed previously, analyses regarding neoadjuvant chemotherapy prior to surgery were not available due to absent information of this parameter throughout the entire study period. In addition, information regarding laboratory data would have been valuable. Other causes of death than ovarian cancer increase with age and the use of overall survival may have caused confounding. However, information on the causes of death was not available.
Residual tumour tissue, advanced FIGO stage, being underweight, comorbidity and perioperative blood transfusion were all found to be predictors of mortality within the first year after primary ovarian cancer surgery. Our results suggest that the surgeon should not just aim at radical surgery, but also pay attention to comorbidity, nutritional state and the use of perioperative blood transfusion. These findings should be confirmed in other settings, and future studies are needed to assess the impact of smoking, alcohol, units of blood transfused and neoadjuvant chemotherapy as predictors of mortality within the first postoperative year after primary ovarian cancer surgery.
Conclusions
In this study, we aimed to examine predictors of mortality within 0–180 and 181–360 days after ovarian cancer surgery. The examined predictors were age, ASA score, BMI, FIGO stage, residual tumour tissue after surgery, perioperative blood transfusion and calendar year of surgery. The overall 1-year survival was 84%. The most important predictors of mortality within 1 year after surgery were residual tumour tissue (0–180 days after surgery) and advanced FIGO stage (181–360 days after surgery). Our results suggest that the surgeon should aim at radical surgery. However, comorbidity, being underweight, age >64 years and blood transfusion were also significant predictors of mortality and need to be studied in more detail.
References
Footnotes
Contributors MØ, MI, RG, OM and BMN were involved in the conception or design of the study, data collection and interpretation of data, as well as in the drafting of the manuscript. MI (statistician) performed the analyses. All authors have read and revised the manuscript critically for important intellectual content, and approved the final version to be published.
Funding The Research Unit of Gynaecology, Odense University Hospital and the Odense University Hospital Research Foundation.
Competing interests None declared.
Ethics approval The present study was approved by the Danish Data Protection Agency (J. number 2012-41-0485).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.