Article Text

Abstract
Introduction Diabetes mellitus affects 9% of the European population and accounts for 15% of healthcare expenditure, in particular, due to excess costs related to complications. Clinical trials aiming for earlier prevention of diabetic nephropathy by renin angiotensin system blocking treatment in normoalbumuric patients have given mixed results. This might reflect that the large fraction of normoalbuminuric patients are not at risk of progression, thereby reducing power in previous studies. A specific risk classifier based on urinary proteomics (chronic kidney disease (CKD)273) has been shown to identify normoalbuminuric diabetic patients who later progressed to overt kidney disease, and may hold the potential for selection of high-risk patients for early intervention. Combining the ability of CKD273 to identify patients at highest risk of progression with prescription of preventive aldosterone blockade only to this high-risk population will increase power. We aim to confirm performance of CKD273 in a prospective multicentre clinical trial and test the ability of spironolactone to delay progression of early diabetic nephropathy.
Methods and analysis Investigator-initiated, prospective multicentre clinical trial, with randomised double-masked placebo-controlled intervention and a prospective observational study. We aim to include 3280 type 2 diabetic participants with normoalbuminuria. The CKD273 classifier will be assessed in all participants. Participants with high-risk pattern are randomised to treatment with spironolactone 25 mg once daily, or placebo, whereas, those with low-risk pattern will be observed without intervention other than standard of care. Treatment or observational period is 3 years.
The primary endpoint is development of confirmed microalbuminuria in 2 of 3 first morning voids urine samples.
Ethics and dissemination The study will be conducted under International Conference on Harmonisation – Good clinical practice (ICH-GCP) requirements, ethical principles of Declaration of Helsinki and national laws. This first new biomarker-directed intervention trial aiming at primary prevention of diabetic nephropathy may pave the way for personalised medicine approaches in treatment of diabetes complications.
Trial registration number NCT02040441; Pre-results.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Multinational, multicentre investigator-initiated clinical trial.
Aim to include more than 3000 participants with 3 years follow-up.
Randomised, double masked intervention with spironolactone 25 mg, or placebo, in selected participants.
Biomarker-directed therapy trial aiming at primary prevention of diabetic nephropathy.
Validation of pre-existing urinary proteomics-based chronic kidney disease (CKD) risk classifier (CKD273).
Introduction
Diabetic nephropathy (DN), characterised by declining renal function and increasing albuminuria (>300 mg/day), is the leading cause of end-stage renal disease (ESRD) in the Western world, and is associated with significant cardiovascular morbidity and mortality.1 Microalbuminuria (>30 mg/g) is the earliest and most commonly used clinical hallmark of increased risk for DN and has evolved into a key marker for risk prediction and treatment monitoring in diabetes. Despite this, numerous alternative biomarkers have been proposed for early identification of individuals at risk of progression to DN, as the sensitivity and specificity of microalbuminuria for early detection of disease are limited by a number of factors: high day-to-day variability of urine albumin excretion; the phenomenon of non-albuminuric DN;2 ,3 and presence of advanced renal pathological changes by the time microalbuminuria is clinically detectable,4 but to date, none have outperformed microalbuminuria in large-scale, prospective studies. For optimal and early diagnosis of individuals at risk of DN, and thereby a need for aggressive intervention, there is a requirement for new markers that can be used in addition to urinary albumin excretion and renal function (glomerular filtration rate; GFR). The pathogenesis of DN is complex and incompletely understood, meaning that it may be simplistic to expect that a single biomarker could perform adequately for early disease detection, risk assessment and therapeutic monitoring. Chronic kidney disease (CKD)273 is a proteomic panel of 273 urinary peptides which has been validated for diagnosis of DN in a multicentre setting, and shows promise as a tool for detection of DN years before development of microalbuminuria.5–7
The renin-angiotensin-aldosterone system (RAAS) plays a key role in the development and progression of DN, and its blockade with ACE-inhibitors (ACEI) or angiotensin II receptor blockers (ARB) is considered first-line therapy for renoprotection in diabetes.8–10 Studies of early initiation of RAAS blockade have shown delay in onset of microalbuminuria, at the cost of increased side-effect burden and cardiovascular events.11 To date, these studies have been performed in largely unselected populations, and their limited success may reflect the fact that fewer patients progress to DN than previously thought, reducing the power.12 ,13
Recent years have seen a resurgence of interest in the role of aldosterone as a mediator of atherosclerotic disease, endothelial dysfunction and oxidative stress. Furthermore, ‘aldosterone breakthrough’ has been associated with a more rapid decline in renal function in patients with DN.14 Numerous small studies suggest that addition of aldosterone antagonist to ACEI or ARB may reduce albuminuria in patients with CKD although large, long-term studies of this therapeutic strategy are lacking.15 It seems feasible that targeting appropriately intensified early preventative therapy towards those at highest risk could limit disease progression as well as side effects resulting from unnecessary prescribing.
To make the transition from bench to bedside, biomarkers must be shown to outperform the current state-of-the-art in large-scale studies, and to inform therapeutic decision-making. The PRIORITY study (proteomic prediction and renin angiotensin aldosterone system inhibition prevention of early DN in type 2 diabetic patients with normoalbuminuria),16 therefore, aims to address two clinical questions: first to confirm that CKD273 can predict development of microalbuminuria in a large cohort of normoalbuminuric patients with type 2 diabetes; and second to determine whether early initiation of aldosterone antagonism can reduce risk of transition to microalbuminuria in individuals identified as ‘high risk’ participants.
Methods and analysis
Study population
The study includes type 2 diabetic patients with preserved kidney function (estimated GFR (eGFR)>45 mL/min/1.73 m2) and normoalbuminuria (urine albumin to creatinine ratio (UACR)<30 mg/g in two of three consecutive morning urine samples). Participants who are eligible, according to the inclusion and exclusion criteria at the screening visit, can be included in the trial (table 1).
Inclusion and exclusion criteria
Study design
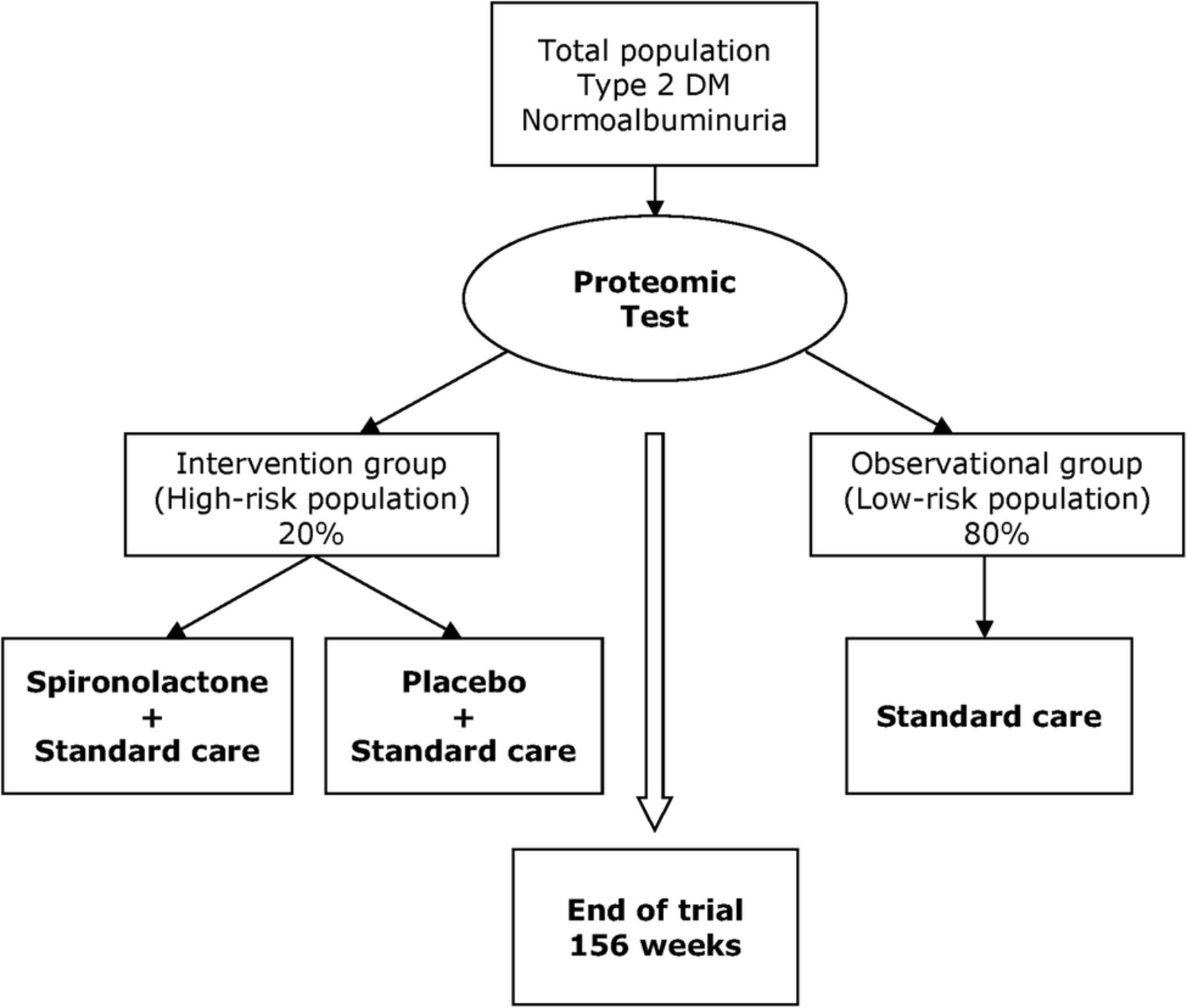
Prospective observational study of participants were stratified as high or low risk based on CKD273, and a prospective, multicentre, randomised, double-masked, placebo-controlled trial of spironolactone in the high-risk patients. All participants fulfilling the inclusion criteria will be screened with CKD273 classifier in order to determine the risk of future DN (figure 1).

{kind=link}
Study design. DM, diabetes mellitus.
Participants with a high-risk pattern will be included in the randomised intervention study with active drug or placebo in addition to standard care, whereas participants with a low-risk pattern will be followed-up on standard-of-care without specific intervention as part of the trial. All participants will be followed for 3 years after the baseline visit.
Intervention
In addition to standard diabetes care, participants with a high-risk proteomics pattern will be randomised to receive the study drug: spironolactone 25 mg tablets for oral use once daily or matching placebo. The randomisation process is computer generated, and randomisation lists will be prepared by an independent statistician at the Robertson Institute, University of Glasgow. The study drug will be labelled with a unique pack identifier number. Assignment to study medication is provided by email to the investigators though a web-based system. Participants will be stratified based on whether or not they are treated with RAAS blocking agents at baseline. Randomisation will be performed 1:1 for placebo and active drug.
Both the study personnel and the patient will be masked to the type of intervention. Placebo and active study drug will not be distinguishable from each other in terms of appearance, odour, labelling or instructions for use. The masking of treatment allocation will be maintained until data lock. The study drug will be produced, stored and distributed in accordance with good manufacturing practice and good distribution practice.
Study visits
At the screening visit, local laboratory blood samples will be taken for creatinine, sodium, potassium and glycated haemoglobin (HbA1c). Compliance with inclusion and exclusion criteria will be evaluated. Weigh, height, blood pressure and heart rate will be measured. Urine sample for proteomic risk assessment with CKD273 will be obtained. Urine samples from the ‘run-in-phase’ will be collected 3 days following the screening visit and brought or sent to the study site. The baseline visit will be performed 6 weeks after the screening visit.
Participants with a high-risk proteomics pattern will be provided with study medication after randomisation, and seen for a safety visit at the study centre after 2 weeks, with local measurement of creatinine and potassium. Every 13th week, participants will be seen in the clinic and provided with the study drug. At each visit, participants will be tested for UACR in three consecutive urine samples, and locally measured biochemistry.
Participants with a low-risk CKD273 pattern will be seen once yearly after the baseline visit and tested for UACR in three consecutive urine samples as well as locally measured biochemistry.
Morning void urine samples are collected by the participants at home on three consecutive days, and brought or sent to the study centre. Participants are provided with a written instruction on how to collect urine samples. Samples are tested for urinary tract infection and in case of urinary tract infection samples are re-done after relevant medical treatment.
Concomitant medical treatment
Treatment of any medical condition aside from hypertension, albuminuria and hyperkalaemia must be in accordance with local guidelines. If local guidelines do not recommend a specific first-line antihypertensive agent it is suggested to start with a calcium channel blocker, or thiazide diuretic, to reduce interference with UACR. Antihypertensive treatment prior to inclusion, especially ACEI or ARB treatment, should be continued unchanged during the ‘run-in phase’ and throughout the study if possible. Participants not on treatment with ACEI or ARB at the time of screening should not start such treatment before the primary endpoint is reached, however, it is not prohibited if indicated due to high blood pressure, although a calcium channel blocker or thiazide diuretics is recommended as first-line intervention unless local guidelines necessitate other intervention. In the duration of the trial, confirmed blood pressure >140 mm Hg systolic and or diastolic >90 mm Hg is considered hypertension where treatment must be considered.
Plasma or serum level of potassium >0.4 mmol/L above local upper reference range is considered hyperkalaemia. The study protocol contains specific treatment guidelines to be followed in case of hyperkalaemia (see online supplementary material). In brief: (1) confirm potassium concentration in a non-haemolysed sample, (2) advise lower dietary intake, (3) review medical treatment for agents known to cause hyperkalaemia, (4) consider treatment with non-potassium sparing diuretics. Temporarily pausing or discontinuation of study medication is mandatory in cases of potassium >0.9 mmol/L above local upper reference range.
Supplemental material
For low-risk patients, routine diabetes treatment can be performed by healthcare providers who are not part of the study team.
Primary endpoint
Development of confirmed microalbuminuria (UACR>30 mg/g) in at least two of three first morning voids with a 30% increase (geometric mean) in UACR from ‘run-in-phase’ samples, or >40 mg/g (geometric mean).
The primary end point is measured at the central laboratory at Steno Diabetes Center on a continuous basis as the trial is running. After arrival and defrosting, the samples are spun for 10 min at 1680 g before subsequent analysis of urine creatinine and urine albumin (Vitros 5600, Ortho C. Diagnostics, France).
In addition to the primary end point, the study protocol prespecifies other renal and cardiovascular secondary end points including change in eGFR (see online supplementary material). To address future scientific questions, blood, urine and DNA samples will be collected at time of randomisation and at end of study.
Sample preparation for urinary proteomics
A total of 0.7 mL of urine will be diluted with 0.7 mL, 2 mol/L urea and 10 mmol/L NH4OH containing 0.02% SDS. For removal of high-molecular weight polypeptides, samples will be filtered using Centrisart ultracentrifugation filter devices (20 kDa molecular weight cut-off; Sartorius, Göttingen, Germany) Subsequently, the filtrate will be desalted using a PD-10 column (GE Healthcare, Stockholm, Sweden) equilibrated in 0.01% NH4OH in high-performance liquid chromatography-grade water. Finally, samples will be lyophilised and stored at 4°C. Shortly before capillary electrophoresis mass spectrometric (CE-MS) analysis, lyophilisates will be resuspended in high-performance liquid chromatography-grade water to a final protein concentration of 0.8 mg/mL checked by BCA assay (Interchim, Montlucon, France). CE-MS analysis will be performed with a P/ACE MDQ capillary electrophoresis system (Beckman Coulter, USA) coupled to a micro-TOF-MS (Bruker Daltonic, Germany). Technical details and characteristics of the CE-MS platform were extensively described recently.17
Urinary proteomic analysis and data processing
CE-MS analysis results in individual data sets contain information on generally 1200–2000 peptides per sample. Mass spectral ion peaks representing identical molecules at different charge states (m/z with z=1, 2, 3…) will be deconvoluted into single masses using MosaiquesVisu software, which employs a probabilistic clustering algorithm and uses isotopic distribution (for z≤6), as well as conjugated masses for charge-state determination of peptides/proteins.18 For noise filtering, signals with z>1 observed in a minimum of three consecutive spectra, with a signal-to-noise ratio of at least four will be considered. For clustering, peptides in different samples will be considered identical, if the mass deviation is lower than ±50 ppm for 800 Da peptides, gradually increasing to ±75 ppm for 15 kDa peptides. Data sets will be accepted only if the following quality control criteria are met: A minimum of 800 peptides (500 peptides on the Q-TOF) must be detected with a minimal MS resolution of 8.000 (required resolution to resolve ion signals with z=6) in a minimal migration time interval (the time window in which separated signals can be detected) of 10 min. All detected polypeptides will be deposited, matched and annotated in a Microsoft Structured Query Language database.19 The final result is a peak list, characterising each protein and peptide by its molecular mass (Da), and normalised CE migration time (min). Migration time and ion signal intensity (amplitude) will be normalised using internal polypeptide standards that include 29 collagen fragments that are generally found in urine, and that do not appear to be highly significantly associated with disease.20
Proteomics classification
The CKD273 classifier is a Support Vector Machine (SVM)-based classification model21 ,22 that was developed for discrimination between patients with CKD and controls.23 Classification is performed by determining the Euclidian distance (defined as the SVM classification score) of the 273-dimensional vector to a 272-dimensional maximal margin hyperplane.23 In previous studies, CKD273 threshold of 0.343 was found to discriminate between patients with and without DN.24 To accommodate the early detection of CKD, the cut-off for use in PRIORITY trial was lowered from 0.343 to 0.154. This decision was based on a post hoc analysis of 737 type 2 diabetic patients from the DIRECT-2 study, where this cut-off was associated with increased risk of progression to microalbuminuria independent of eGFR and UACR, and was present in 20% of the participants.25 Scoring above this threshold indicates high risk of development of DN.
Statistical analysis
A statistical analysis plan (SAP) will be written and signed before database lock. Analyses not described here or in the SAP will be considered exploratory/post hoc analyses.
The predictive value of a positive and negative test, specificity and sensitivity of the test in relation to prediction of development of the primary end point will be calculated. To assess whether CKD273 improves risk prediction of the primary outcome we will determine the concordance statistic (c-statistic). Both parameters measure the discriminative ability of a marker in a model to distinguish between people who will or will not develop the outcome (in case of predictive methods).
The primary end point will be analysed in the total population with comparisons of high-risk versus low-risk pattern and active versus placebo treatment using a Cox proportional-hazards regression model with treatment as a fixed effect. The model will be adjusted for independent predictive covariates and at least for the baseline UACR. A two-tailed Wald χ2 test with an α level of less than 0.05, and HRs with two-sided 95% CIs will be calculated.
The study statistician will be partly unmasked while conducting statistical analysis with information regarding an ad hoc allocation to either group 1 or 2, but without information about which group received active or placebo treatment. Final unmasking will be done after all analysis in the SAP has been conducted.
Sample size
The expected relative proportions of type 2 diabetic patients developing microalbuminuria (within 3 years) in our study population are: 25% in participants at high risk for DN in the treatment group, 35% in participants at high risk for DN in the placebo group, and 4% in therapy-naive participants at low risk for DN. Using the samples size formula for two proportions test (α=0.05 β=0.80), randomised (1:1), n=328 in each arm of the intervention group is required. It is expected that approximately 20% of the population will be at high risk based on CKD273, therefore, at least 3280 participants have to be included overall.
Estimated sample size can be revisited in an amendment to the study protocol if new data emerge while conducting the trial.
Ethics and dissemination
The study will be performed under International Conference on Harmonisation – Good clinical practice (ICH-GCP) requirements, ethical principles of the Declaration of Helsinki, and national laws and regulations depending on each country. Written favourable opinion from independent ethical committees must be obtained before starting the study in the respective country. The study is a prospective study, and written approval of the respective national competent authorities and/or other regulatory authorities, if applicable, must be available before study-specific procedures are performed for the first participant.
It is the responsibility of the investigator to obtain written informed consent from each individual participating in this study after adequate explanation of the aims, methods, objectives and potential hazards of the study. It should be made clear that refusal to participate or withdrawal from the trial at any stage will have no consequences regarding the patient's subsequent care. No patient should feel obliged to participate in the trial. If there is any doubt as to whether the patient has understood the written and verbal information, the patient should not enter the trial.
Data from the study will be published in international, peer-reviewed journals.
Project management
The chief investigator is professor Peter Rossing. The consortium consists of 15 partners from 10 countries, with 13 study centres including participants. The trial is registered at the EU Clinical Trials Register (EudraCT: 2012-000452-34), as well as at http://www.clinicaltrial.gov (NCT02040441). An external advisory board contributed in the creation of the study protocol. Prior to inclusion of participants, an independent data monitoring committee will be established.
Discussion
The PRIORITY study is innovative in several ways and will provide important data, regardless of its outcome. First, the prospective validation of a new biomarker in a chronic disease such as diabetes, is unique, and will provide solid answers instead of speculations so frequently put forward from retrospective biomarker studies. Second, this investigator-initiated multicentre study will investigate the effect of spironolactone, an off-patent drug with the potential to provide early prevention of DN, by contrast with new and more expensive drugs with a less robust clinical safety record. Combining the ability to select high-risk individuals based on a new biomarker, and a clinical trial with intervention, thus provides information both on the utility of the biomarker, as well as the effect of the intervention, for the targeted high-risk population. Third, the PRIORITY study represents a remarkable clinical collaboration across Europe, with the support of the EU, and as such, experiences from the study may provide a blueprint for future non-industry-led clinical trials in indications and diseases currently not covered by available evidence.
Several markers have been suggested as predictors of DN, in particular, elevated the urinary albumin excretion rate.26 Urinary albumin has, however, turned out to be less specific than originally thought, and thus, markers that can improve precision in prediction as well as provide even earlier indications on increased risk for DN are warranted.
The present study will validate a new test based on urinary proteomics in a prospective way. Whereas microalbuminuria is thought to reflect the presence of glomerular filtration barrier damage with increased leak of albumin into the urine, we propose that the urinary proteomic-based classifier (CKD273) reflects altered composition of mesangial extracellular matrix components, which occur before any structural damage to the filtration barrier has developed. In fact, we have demonstrated that changes in the urinary peptidome can predict the development of overt DN in patients with normoalbuminuria.7 ,23 ,24 The urinary proteomic marker not only differentiates between normoalbuminuria and DN, but also identifies participants at risk of progression from normoalbuminuria to macroalbuminuria, about 4 years before development of DN.7 This proteomic test has been evaluated in cross-sectional and retrospective longitudinal studies but, not unlike other biomarkers, it has not yet been investigated in specifically designed prospective studies.
Blockade of the renin angiotensin system with ACEI or ARB has been the cornerstone of renoprotective treatment in diabetes. RAAS blockade is best established in patients with microalbuminuria or macroalbuminuria,8 ,27 whereas, early treatment/prevention in normoalbuminuric patients has yielded more variable results.11 ,28 ,29 In recent years, it has become clear that aldosterone should be considered a hormone with widespread unfavourable effects on the vasculature, the heart and the kidneys.30–32 We have demonstrated that elevated plasma aldosterone despite long-term treatment with losartan, what has been termed ‘aldosterone breakthrough’, is associated with a faster decline of GFR in type 1 diabetic patients with DN.14 Short-term studies in proteinuric type 1 and type 2 diabetic patients have demonstrated that spironolactone safely adds to the renal and cardiovascular protective benefits of treatment with maximally recommended doses of ACEI or ARB by reducing albuminuria and blood pressure.33 ,34 The selective aldosterone receptor antagonist, eplerenone, also reduced proteinuria by 48% when added to an ACEI in type 2 diabetes patients with albuminuria >50 mg/g.35 In less advanced DN (microalbuminuria), we observed an even larger effect on urinary albumin excretion when adding spironolactone to standard treatment including an ACEI, with reductions of 60% in albuminuria, suggesting that early prevention is better than treatment.36 Although treatment with aldosterone blockade has been avoided for many years in nephrology, participants eligible for this trial will not suffer from renal impairment, and the dose of spironolactone is low, thus, the risk of adverse events due to hyperkalaemia or gynaecomastia is reduced.
The PRIORITY study population consists of patients with type 2 diabetes, which is highly relevant, as prevalence and incidence of this chronic condition are increasing in Europe and worldwide.37 Currently, type 2 diabetes accounts for 15% of the healthcare budget in European nations, and prevention or delaying of complications such as DN is vital in order to prevent health costs from increasing. A patient with complications costs approximately six times more than a patient with uncomplicated type 2 diabetes.38 In addition, patients with DN are at risk of substantial comorbidity, as well as cardiovascular complications and advanced kidney disease. Diabetes represents the leading cause of ESRD in most of the world. Any early intervention that can prevent or delay DN will, therefore, have substantial impact. A health economic cost-benefit analysis should be performed after publication of results from the PRIORITY trial to compare costs related to screening with new markers and early treatment versus potentially saved costs on prevented ESRD treatment and ESRD complications.
Limitations of this study
The major limitation of this study is that our primary end point is only a surrogate end point (development of microalbuminuria) rather than a hard end point, such as doubling of serum creatinine, development of ESRD or renal death, but so far, development of microalbuminuria is the only available end point for early intervention. This surrogate end point was chosen instead of using hard end points, as the trial is conducted in a normoalbuminuric population. Development of hard renal end points can take up to 20 years12 in such populations, hence, persistent microalbuminuria, which is considered a valid surrogate end point will be a feasible and acceptable outcome for our study.39 The aim to replace albuminuria as a biomarker, by designing a study based on albuminuria as outcome, may appear suboptimal at first glance. However, despite all criticisms, microalbuminuria has consistently found its way into clinical guidelines and is the key event in a diabetes patient's clinical course that triggers the initiation of renoprotective therapy. As such, the prediction and prevention of microalbuminuria, despite its limitations, is a clinically important surrogate end point that has changed clinical practice.40
With assignment of treatment to the participants with a high-risk pattern only, the trial cannot address the effect of treatment in participants with a low-risk pattern or answer the question of whether the combination of screening and treatment is superior to a non-screening.
There is no wash-out period included at the end of the study. Thus, we cannot exclude that UACR would increase to microalbuminuric levels in the intervention group if treatment was withdrawn. On the other hand, several studies have demonstrated that reduction in UACR with treatment predicts decreased development of renal and cardiovascular end points.41 ,42
Future translation of the results of this trial into widespread clinical practice will be challenging due to the cost and complexity of the proteome analysis and associated intellectual property rights. Currently, only a limited number of laboratories worldwide are able to perform the CE-MS analysis to the required standard, and to analyse the MS data to produce the CKD273 classifier. The limited number of diagnostic laboratories is in contrast with the potential need in the event that the CKD273 classifier delivers its promises. However, CE-MS technology itself is widely available, and specific analysis pipelines can be applied based on the patent holder's protocols and, thereby, widely implemented across laboratories worldwide. Alternatively, multiplex markers may be developed, but the sensitivity and specificity will be reduced if the number of peptides included in the classifier is reduced.
Potential impact of the PRIORITY trial
Previous and current trials usually aim to include participants with a specific phenotype based on biochemical values such as eGFR and/or level of albuminuria. By contrast, our novel approach uses targeted intervention based on a proteomics-based risk classifier. This will be the first ‘omics’-based biomarker-directed therapy trial targeting type 2 diabetes patients, aiming at primary prevention of DN. Furthermore, as the urinary proteomic test is based on a large number of polypeptides related to different processes associated with progression of renal disease, improved understanding of these processes could further improve the possibilities for personalised medicine as well as new targeted interventions.
If the proteomic classifier is validated in this prospective study, we will establish an earlier marker for DN than microalbuminuria, and potentially, a much more specific one. This will enable us in future studies to include only high-risk patients in interventional trials, increasing the event rate and reducing the number of patients needed to be included in the trial. Furthermore, identification of low-risk patients who do not need additional renoprotective treatment will protect them from unnecessary intervention, risk of side effects and save medical costs.
Even if we are not successful with both our aims, we may still prove the value of the biomarker, or the benefit of early intervention with spironolactone. However, if the study successfully achieves both aims, we will have a new diagnostic strategy for early identification of individuals at risk for the most devastating and expensive complication of diabetes, as well as a cheap intervention to offer.
References
Footnotes
Contributors ML, FP, GC, JB, CD, HvdL, HM, GN, MN, AO, PLR, IR, GS and PR conceived the study. ML, FP, GC, CP, CD, HM and PR wrote the initial draft. FP, GC, CD, MN, AO, IR, GS and PR provided feedback and comments. All authors approved the final version of the manuscript prior submission. ML and FP took responsibility for the submission process.
Funding The PRIORITY project is an investigator-initiated study funded under Framework Programme 7 of the European Commission Directorate General for Research and Innovation. Project ID: Health-F2-2011-279277.
Competing interests HM is co-founder and a shareholder of Mosaiques Diagnostics GmbH (Hannover, Germany). CP is employed at Mosaiques Diagnostics.
Ethics approval Voluntary Harmonisation Procedure for the assessment of multinational clinical trial applications. Followed by approval in each participating country with a approval from national competent authority and IEC.
Provenance and peer review Not commissioned; externally peer reviewed.