Article Text

Abstract
Objective To compare the efficacy and safety of a concentrated formulation of insulin glargine (Gla-300) with other basal insulin therapies in patients with type 2 diabetes mellitus (T2DM).
Design This was a network meta-analysis (NMA) of randomised clinical trials of basal insulin therapy in T2DM identified via a systematic literature review of Cochrane library databases, MEDLINE and MEDLINE In-Process, EMBASE and PsycINFO.
Outcome measures Changes in HbA1c (%) and body weight, and rates of nocturnal and documented symptomatic hypoglycaemia were assessed.
Results 41 studies were included; 25 studies comprised the main analysis population: patients on basal insulin-supported oral therapy (BOT). Change in glycated haemoglobin (HbA1c) was comparable between Gla-300 and detemir (difference: −0.08; 95% credible interval (CrI): −0.40 to 0.24), neutral protamine Hagedorn (NPH; 0.01; −0.28 to 0.32), degludec (−0.12; −0.42 to 0.20) and premixed insulin (0.26; −0.04 to 0.58). Change in body weight was comparable between Gla-300 and detemir (0.69; −0.31 to 1.71), NPH (−0.76; −1.75 to 0.21) and degludec (−0.63; −1.63 to 0.35), but significantly lower compared with premixed insulin (−1.83; −2.85 to −0.75). Gla-300 was associated with a significantly lower nocturnal hypoglycaemia rate versus NPH (risk ratio: 0.18; 95% CrI: 0.05 to 0.55) and premixed insulin (0.36; 0.14 to 0.94); no significant differences were noted in Gla-300 versus detemir (0.52; 0.19 to 1.36) and degludec (0.66; 0.28 to 1.50). Differences in documented symptomatic hypoglycaemia rates of Gla-300 versus detemir (0.63; 0.19to 2.00), NPH (0.66; 0.27 to 1.49) and degludec (0.55; 0.23 to 1.34) were not significant. Extensive sensitivity analyses supported the robustness of these findings.
Conclusions NMA comparisons are useful in the absence of direct randomised controlled data. This NMA suggests that Gla-300 is also associated with a significantly lower risk of nocturnal hypoglycaemia compared with NPH and premixed insulin, with glycaemic control comparable to available basal insulin comparators.
- DIABETES & ENDOCRINOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first comprehensive literature review and network meta-analysis (NMA) summarising the available clinical trial literature on the clinical benefits of the newly approved basal insulin, Gla-300, and potential basal insulin comparators, and enabling comparisons between these therapies.
The systematic literature review was limited to only English language literature; while this is likely to include all major randomised clinical trials conducted for basal insulin therapy in type 2 diabetes mellitus (T2DM), it may exclude smaller studies with no publication in English.
The NMA was conducted in accordance with National Institute for Health and Care Excellence guidance and extensive sensitivity analyses were utilised to assess the robustness of the findings.
While NMA enables the synthesis of available clinical information, it is not a substitute for head-to-head clinical trials to compare therapies, and such trials should be encouraged and conducted.
Introduction
Worldwide, approximately 348.3 million people are living with type 2 diabetes mellitus (T2DM).1 ,2 As T2DM progresses, insulin therapy may be required to achieve glycaemic control. The 2015 ADA/EASD Position Statement on Managing Hyperglycemia in T2DM recommends initiating basal insulin in combination with oral therapy among the appropriate options for patients who are unable to achieve their glycated haemoglobin (HbA1c) target after 3 months of metformin monotherapy.3
Insulin glargine 300 u/mL (Gla-300) is a new basal insulin that has recently (2015) been approved by the European Commission and the US Food and Drug Administration. Gla-300 is a concentrated formulation of insulin glargine 100 u/mL (Gla-100), developed to produce a more flat and more prolonged pharmacokinetic and pharmacodynamic profile.4–6 Several randomised controlled clinical safety and efficacy trials comparing Gla-300 to Gla-100 have shown that Gla-300 achieves reduction in HbA1c comparable to that of Gla-100, while lowering the risk of hypoglycaemia.6–8 Comparable HbA1c reduction is expected given that each treatment group utilised the same dose titration to achieve fasting plasma glucose of 4.4–5.6 mmol/L (ie, treat-to-target approach). The lower hypoglycaemia rates observed with Gla-300 may be due to properties inherent to the glargine molecule that lead to pharmacokinetic and pharmacodynamic differences at varying concentrations (ie, between Gla-300 and Gla-100).4 ,5
At the present time, head-to-head studies of Gla-300 with other available basal insulin options have not been conducted; however, such comparisons would help determine the place in therapy for this product. Meta-analysis enables the findings from multiple primary studies with comparable outcome measures to be combined.9 In absence of direct head-to-head clinical trials, mixed treatment meta-analysis (also known as network meta-analysis (NMA)) may be used to estimate comparative effects of multiple interventions using indirect evidence.9 The current report is an NMA conducted to indirectly compare the efficacy and safety of U300 versus available intermediate-acting to ultra-long-acting basal insulin formulations in the treatment of T2DM.
Methods
Systematic literature review
A systematic literature review was conducted to identify evidence for the clinical efficacy and safety of insulin regimens in T2DM according to National Institute for Health and Care Excellence (NICE) standards.9 The following electronic databases were searched: the Cochrane Library (eg, the Cochrane Central Register of Controlled Trials (CENTRAL) and the Database of Abstracts of Reviews of Effectiveness (DARE)), MEDLINE and MEDLINE In-Process (using Ovid platform), EMBASE (using Ovid Platform) and PsycINFO. Congresses searched were the European Association for the Study of Diabetes (EASD; 2011–2013), the American Diabetes Association (ADA; 2011–2013) and the International Diabetes Federation (IDF; 2011 and 2013). Key search terms included: ‘diabetes mellitus, type 2/’, ‘glargine’, ‘detemir’, ‘degludec’, ‘NPH’, ‘neutral protamine hagedorn’, ‘biphasic’, ‘aspart protamine’, ‘novomix’ and ‘premix’. Searches were limited to human, English-language only articles published from 1980 onwards. The NMA focused on studies published recently (ie, based on availability of basal insulin analogues). At the time of analysis, the Gla-300 vs Gla-100 studies were only available in clinical study reports; however, these studies have subsequently been published.6–8
Several quality control procedures were in place to ensure appropriate study selection and data extraction. Screening of abstracts and full-text was conducted by two independent researchers (a third independent researcher made a final determination for articles for which there was uncertainty). Data extraction was also conducted by two independent researchers (with reconciliation of discrepancies). Where available, full-text versions of the article were used for data extraction (an abstract or poster was not used unless it was the terminal source document). All processes were documented by the researchers and the data extraction file was also quality checked. The source materials (abstracts, full-text articles) and data extraction files were sorted, and saved on a secure server.
Inclusion criteria
In order to be considered for the NMA, clinical studies identified by the systematic literature review had to meet the following criteria: randomised active comparator-controlled clinical studies, patient population of adults with T2DM treated with basal insulin (with or without bolus), patients could be newly initiating insulin (naïve) or already exposed to insulin, and a minimum follow-up of 20 weeks. In addition, studies were required to have patients from at least one of the following countries: the USA, France, Germany, the UK, Spain and/or Italy.
Outcome measures
Outcome measures analysed by NMA included change in HbA1c (%) from baseline, change in body weight (kg) from baseline and rates of hypoglycaemic events (documented symptomatic and/or nocturnal) per patient year. A documented symptomatic event was defined as an event during which typical symptoms of hypoglycaemia were accompanied by measured plasma glucose under a threshold value. In the EDITION trials, the results were reported using both a concentration of ≤3.0 mmol/L and of ≤3.9 mmol/L. No restriction on the threshold levels was imposed. A 3.9 mmol/L threshold for the EDITION trials was selected to be consistent with the majority of other trials in the network. Nocturnal hypoglycaemic events were defined as any event (confirmed and/or symptomatic) occurring during a period at night.
Statistical methods
All analyses were implemented using the statistical software R and OpenBUGS, specifically the packages using Markov Chain Monte Carlo (MCMC). Examples of coding used are provided in an online supplemental appendix. Randomised clinical trials that were identified from a systematic literature review and that met the study selection inclusion criteria were analysed using a random-effect Bayesian NMA, following the UK NICE guidance.9 Each outcome was analysed within the evidence network where it was reported. MCMC was used to estimate the posterior distribution for treatment comparison. Continuous outcomes (eg, change in HbA1c or body weight) were modelled assuming a normal likelihood and an identity link. Event rate data (eg, number of hypoglycaemic episodes per patient-year follow-up) were modelled using a Poisson mixed likelihood and log link. Non-informative priors were assumed.
Sensitivity analyses
Sensitivity analyses including meta-regression were conducted to evaluate the robustness of the findings. The base scenario included studies of patients on basal insulin-supported oral therapy (BOT; patients received basal insulin in combination with oral antihyperglycaemic drugs but with no bolus insulin; patients could be either—insulin naïve or insulin experienced). Additional scenarios were all studies (ie, patients receiving basal insulin with or without bolus), studies of patients on BOT excluding premixed studies, studies of insulin-naïve patients only, only studies with Week 24–28 results, and excluding degludec three times weekly (3TW) dosing. Meta-regression was conducted for key outcomes to account for study-level population characteristics, adjusting for the following: study-level baseline HbA1c, diabetes disease duration and basal-bolus population. In addition, broader definitions for hypoglycaemia were analysed. A comparison of NMA to classical meta-analysis in the base scenario (BOT) using an inverse variance-weighted method was also conducted.
Results
Systematic literature review
Over 4000 studies were identified for screening, of which 86 were identified for data extraction; from these, 41 studies were included in the NMA (figure 1A). A brief overview of these studies is provided in table 1.
Randomised comparative studies included in NMA of patients with T2DM on basal insulin treatment

(A) PRISMA flow diagram for studies comparing basal insulin therapies in type 2 diabetes mellitus (T2DM; N=41). aCochrane Library (eg, the Cochrane Central Register of Controlled Trials (CENTRAL) and the Database of Abstracts of Reviews of Effectiveness (DARE)), MEDLINE and MEDLINE In-Process (using Ovid platform), Embase (using Ovid Platform) and PsycINFO; If applicable, relevant results from clinical trial registry were included. Zinman et al34 report 2 distinct studies within 1 publication. bFor title/abstract and full-text review, articles were excluded based on inclusion/exclusion criteria as specified in the systematic literature review. cTwo articles analysed the same trial. dConferences searched included EASD and ADA 2011–2013, and IDF 2011. IDF 2013 was assessed when the CD-ROM became available—the end of February. Multiple abstracts examined the same trial and 14 trials were extracted. eStudies must include at least two treatment arms in the network, including: U300, insulin glargine, insulin detemir, insulin NPH, insulin degludec and premix insulin. (B) Evidence network diagram for BOT studies (n=25) reporting HbA1c (%) change from baseline. Each insulin treatment is a node in the network. The links between the nodes represent direct comparisons. The numbers along the lines indicate the number of trials or pairs of trial arms for that link in the network. Reference numbers indicate the trials contributing to each link. BOT, basal insulin-supported oral therapy; HbA1c, glycated haemoglobin; NPH, neutral protamine Hagedorn.
Included trials
All studies were randomised based on entry criteria, with interactive voice (or web) response system or telephone system as the main method of randomisation (n=22), followed by use of sequential numbers/codes (n=6) and electronic case record system (n=1); the method of randomisation was either not reported or not clear in the remaining studies (n=12). The majority (40/41) of studies specified an open-label in design (1 study did not specify). Loss to follow-up (ie, rates of discontinuation among randomised patients) among the studies ranged from 1.6% to 28.5%, with 10 studies reporting discontinuation rates <10%, 22 reporting 10–20% and 5 reporting >20% in at least one treatment arm (loss to follow-up was not reported in 4 studies). The baseline patient characteristics of patients in each of the 41 studies are provided in table 2.
Patient baseline characteristics for trials included in the NMA (N=41)
Twenty-five of the 41 studies (61%) were of patients on BOT (main population for this analysis; n=15 746 patients). The evidence network for the BOT studies is depicted in figure 1B. Patients in the BOT studies had a mean age ranging from 52.4 to 61.7 years, duration of diabetes 8.2–13.8 years, baseline body weight 81.3–99.5 kg and HbA1c 7.8–9.8%.
Glycaemic control
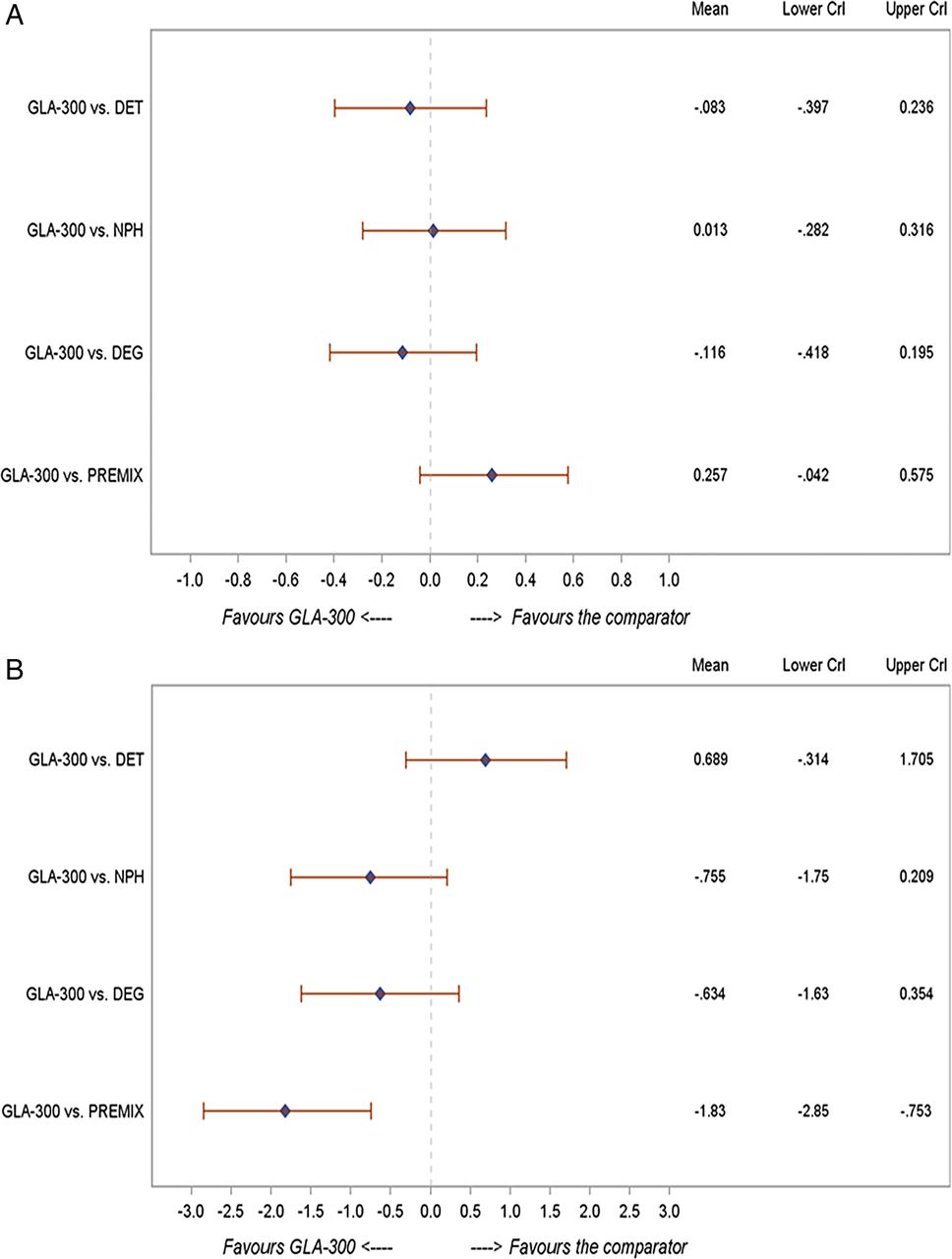
In patients with T2DM on BOT (n=25 studies), the change in HbA1c was comparable between Gla-300 and insulin detemir (−0.08; −0.40 to 0.24), neutral protamine Hagedorn (NPH; 0.01; −0.28 to 0.32), degludec (−0.12; −0.42 to 0.20) and premixed insulin (0.26; −0.04 to 0.58) (figure 2A). These changes were similar to those in the overall NMA (n=41 studies) and across the various sensitivity analyses shown in table 3A.
Additional analyses

NMA findings for Gla-300 versus other basal insulins in the BOT population: (A) change in HbA1c (%); (B) change in body weight (kg); (C) risk of nocturnal hypoglycaemia; (D) risk of documented symptomatic hypoglycaemia. BOT, basal insulin-supported oral therapy; CrI, credible interval; DET, =insulin detemir; DEG, insulin degludec; HbA1c, glycated haemoglobin; NMA, network meta-analysis; NPH, neutral protamine Hagedorn; PREMIX, premixed insulin; RR, risk ratio.

{kind=link}
{kind=link}
{kind=link}
Continued
Body weight
Change in body weight from baseline was reported in 36 trials in the NMA. Among patients with T2DM on BOT, no statistically significant difference in body weight change was observed between Gla-300 and detemir (difference: 0.69; 95% CrI −0.31 to 1.71), NPH (−0.76; −1.75 to 0.21) or degludec (−0.63; −1.63 to 0.35), whereas weight gain was significantly lower with Gla-300 compared with premixed insulin (−1.83; −2.85 to −0.75) (figure 2B). These changes were similar to those in the overall NMA (n=41 studies) and across the various sensitivity analyses (table 3A).
Hypoglycaemia events
Among the studies identified, 20 trials reported nocturnal hypoglycaemia event rate data and 16 reported documented symptomatic hypoglycaemia event rate data that met criteria for inclusion in the NMA. The hypoglycaemia event data from each of these clinical trials are summarised in table 4.
Hypoglycaemia outcomes for trials included in the NMA
Nocturnal hypoglycaemia
In patients with T2DM on BOT, Gla-300 was associated with a significantly lower nocturnal hypoglycaemia rate compared with NPH (0.18; 0.05 to 0.55) and premixed insulin (0.36; 0.14 to 0.94) and a numerically lower rate when compared with detemir (0.52; 0.19 to 1.36) and degludec (0.66; 0.28 to 1.50) (figure 2C). These changes were similar to those in the overall NMA (n=41 studies) and across the various sensitivity analyses (table 3A).
Documented symptomatic hypoglycaemia
In patients with T2DM on BOT, Gla-300 was associated with a numerically lower rate of documented symptomatic hypoglycaemic events compared with detemir (0.63; 0.19 to 2.00), NPH (0.66; 0.27 to 1.49) and degludec (0.55; 0.23 to 1.34) (figure 2D). These changes were similar to those in the overall NMA (n=41 studies) and across the various sensitivity analyses (table 3A). In the BOT population, comparative data for premixed insulin were not available for this particular outcome.
Comparison of NMA to classic meta-analysis findings
The comparison of NMA results that integrate all available evidence versus those from classical meta-analysis solely based on direct evidence in the base scenario (BOT) found generally consistent effect size across all four outcomes and tighter 95% CIs with the classical meta-analysis (table 3B).
Discussion
In this NMA of randomised clinical studies comparing various basal insulin therapies in patients with T2DM, the new concentrated formulation, Gla-300, demonstrated change in HbA1c that was comparable to the change reported in studies of insulin detemir, degludec, NPH and premixed insulin. Change in body weight with Gla-300 was significantly less than that with premixed insulin and comparable to the other basal insulin. Hypoglycaemia rates appeared lower with Gla-300 and the comparator basal insulin. The rate of documented symptomatic hypoglycaemia associated with Gla-300 was numerically but not significantly different from that of other basal insulin therapies. A notable difference was that Gla-300 was associated with a significantly lower risk of nocturnal hypoglycaemia (ranging from approximately 64% to 82% lower) compared with premixed insulin and NPH.
These NMA data extend our current knowledge regarding Gla-300. Based on direct comparisons in the EDITION studies, Gla-300 was associated with comparable glycaemic control, but had a significantly lower rate of nocturnal hypoglycaemia compared with Gla-100.6–8 The more flat and more prolonged pharmacokinetic profile associated with Gla-300 compared with Gla-100 may contribute to the reduced rate of nocturnal hypoglycaemia that is observed clinically. Reasons for the difference in pharmacokinetic profile between Gla-100 and Gla-300 are not known, but may be due to factors inherent to the retarding principle of the insulin glargine molecule and a phenomenon of surface-dependent release.4 ,5 Gla-300 has a pH of approximately 4, at which it is completely soluble; however, once injected subcutaneously, the solution is neutralised and forms a precipitate allowing for the slow release of small amounts of insulin glargine. It has been suggested that the size (ie, surface area) of the subcutaneous deposit may determine the redissolution rate.51
The finding of a significantly lower rate of nocturnal hypoglycaemia associated with a basal insulin analogue compared with NPH is consistent with previous meta-analyses. For example, a meta-analysis of randomised clinical trials comparing long-acting basal insulin analogues (Gla-100 or detemir) with NPH showed that, among 10 studies reporting data for nocturnal hypoglycaemia, both analogues were associated with a reduced risk of nocturnal events, with an OR of 0.46 (95% CI 0.38 to 0.55) compared with NPH.52 Similarly, in the pivotal Treat-to-Target study comparing Gla-100 to NPH, the risk reduction with Gla-100 ranged from 42% to 48% for different categories of nocturnal hypoglycaemic events.26 A subsequent meta-analysis of individual patient data from 5 randomised clinical trials comparing Gla-100 to NPH, reported reductions of approximately 50% in nocturnal hypoglycaemia with Gla-100.53 Given these data, along with patient-level data from the EDITION trials,6–8 which when pooled54 demonstrated a 31% lower relative difference in the annualised rate of nocturnal events over the 6-month study period for Gla-300 compared with Gla-100, the even more pronounced difference in the rate of nocturnal events between Gla-300 and NPH in this NMA is expected.
The finding of fewer nocturnal hypoglycaemic events with Gla-300 compared with premixed insulin in this NMA is in line with ‘real-world’ data from the Cardiovascular Risk Evaluation in people with type 2 Diabetes on Insulin Therapy (CREDIT) study, an international observational study that provided insights on outcomes following insulin initiation in clinical practice.55 In CREDIT study, propensity-matched groups were evaluated 1 year after initiating insulin treatment and showed that basal insulin was associated with significantly lower rates of nocturnal hypoglycaemia compared with premixed insulin. This also held true for propensity-matched analysis of basal plus mealtime insulin versus premixed insulin groups.
The substantially lower risk of nocturnal hypoglycaemia associated with Gla-300 is an important finding given the clinical burden associated with such events.56 In a multination survey of 2108 patients with diabetes (types 1 and 2) who had recently experienced nocturnal hypoglycaemia, patients reported a negative impact on their sleep quality as well as their functioning, the day after a nocturnal hypoglycaemic event.57 Nocturnal events were associated with increased self-monitoring of blood glucose, and approximately 15% of patients reported temporary reductions in insulin dose. An economic evaluation of these data found that nocturnal hypoglycaemic events were associated with lost work productivity and increased healthcare utilisation.58 Utilisation costs were estimated to be higher among patients who injured themselves due to a trip or fall associated with their nocturnal hypoglycaemia episode (approximately $2000 per person annually).
While the findings of this NMA are promising for Gla-300, several limitations are evident. The studies included in this NMA were of open-label design, which is inherently subject to bias; however, this type of methodology is typically used in trials comparing insulin therapies due to visible differences between insulin products and/or differences in injection devices. A potential issue is that there was no multiplicity adjustment, and given that there were multiple comparisons, it is possible that positive findings were due to chance. In addition, trial-level summary data may not have been adequately powered to detect differences between products—for example, while randomised controlled studies of Gla-100 versus Gla-300 and pooled patient level data from these studies have shown that Gla-300 is associated with a significantly lower rate of nocturnal hypoglycaemia, the trial-level data comparisons in this NMA did not achieve significance for this end point. Finally, a well-recognised limitation of any NMA is that, by design, these are not randomised comparisons; however, these data can aid the decision-making process until prospective randomised comparative clinical trial data become available.
Strengths of the current NMA include that it was conducted in accordance with established NICE guidelines and that the estimates reported are in line with those in previous meta-analyses of comparative basal insulin studies.52 ,53 ,59 ,60 NMA provides the capability of considering different pathways simultaneously rather than simple indirect pairwise comparison through multiple pathways. Another strength is the quality of studies included in the NMA (ie, the majority had discontinuation rates <20%). The studies included were similar in design and, from a clinical standpoint, heterogeneity of the patient population was not considered an issue. Results of the NMA were internally consistent with what was reported in individual RCTs. Finally, extensive sensitivity analyses considering subsets of studies, different hypoglycaemia definitions and adjusting for trial-level characteristics, supported the robustness of the findings.
In conclusion, clinical trial findings and the results from this NMA suggest that Gla-300 in the treatment of T2DM is associated with a lower rate of nocturnal hypoglycaemia than treatment with premixed insulin and NPH, while demonstrating comparable glycaemic control versus all comparators. Change in body weight was significantly lower for Gla-300 versus premixed insulin, and comparable with other basal insulin. These NMA data, along with randomised clinical trial findings of reduced nocturnal hypoglycaemia and comparable clinical benefits for Gla-300 versus Gla-100, suggest that this new basal insulin represents an important advance in insulin treatment for patients with T2DM.
Acknowledgments
The authors would like to acknowledge Keith Betts, Ed Tuttle, Simeng Han, Jinlin Song, Alice Zhang and Joseph Damron, from the Analysis Group, for study analysis support, and Kulvinder K Singh, PharmD, for medical writing support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors NF, EC, CF and AV conceived and designed the study. NF, EC, CF, DZ, WL, AV, HW, H-wC, QZ, EW and CG contributed to the draft of the manuscript. All the authors have read and approved the final version of the manuscript.
Funding Sanofi sponsored the NMA.
Competing interests NF reports personal fees from Sanofi Aventis, during the conduct of the study and personal fees from Novo Nordisk, outside the submitted work. EC and HW are employees of Sanofi. CF, DZ and EW report grants from Sanofi, during the conduct of the study; and the Employer (Analysis Group) has received other grants from Sanofi to fund other research (eg, in different therapeutic areas); the Employer has similar arrangements with other drug and medical device manufacturers. WL received honoraria and compensation for travel and accommodation costs for attending advisory boards from Sanofi Aventis. AV is an employee of Sanofi and owner of Sanofi shares. QZ is a former employee of Sanofi, and owner of Sanofi shares. CG is a former employee of Sanofi.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.