Article Text

Abstract
Objective The transition from hospital to home represents a key step in the management of patients and several problems related to this transition may arise, with potential adverse effects on patient health after discharge. The purpose of our study was to explore the association between components of the hospital discharge process including subsequent continuity of care and patient outcomes in the post-discharge period.
Design Systematic review of observational and interventional studies.
Setting We conducted a combined search in the Medline and Web of Science databases. Additional studies were identified by screening the bibliographies of the included studies. The data collection process was conducted using a standardised predefined grid that included quality criteria.
Participants A standard patient population returning home after hospitalisation.
Primary and secondary outcomes Adverse health outcomes occurring after hospital discharge.
Results In the 20 studies fulfilling our eligibility criteria, the main discharge-process components explored were: discharge summary (n=2), discharge instructions (n=2), drug-related problems at discharge (n=4), transition from hospital to home (n=5) and continuity of care after hospital discharge (n=7). The major subsequent patient health outcomes measured were: rehospitalisations (n=18), emergency department visits (n=8) and mortality (n=5). Eight of the 18 studies exploring rehospitalisations and two of the eight studies examining emergency department visits reported at least one significant association between the discharge process and these outcomes. None of the studies investigating patient mortality reported any significant such associations between the discharge process and these outcomes.
Conclusions Irrespective of the component of the discharge process explored, the outcome considered (composite or not), the sample size and the study design, no consistent statistical association between hospital discharge and patient health outcome was identified. This systematic review highlights a wide heterogeneity between studies, especially in terms of the component(s) of the hospital discharge process investigated, study designs, outcomes and follow-up durations.
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This review is the first to date focusing on the relationship between components of hospital discharge organisation and subsequent patient health in a standard population returning home after hospitalisation.
Quality assessment of the included studies was based on two combined tools to take account of the heterogeneity of the underlying study designs.
The numerous discharge process elements investigated in the studies were categorised into several component types, and the impact of each component was assessed with regard to the corresponding health outcome(s) that was reported.
A single author was involved in critical steps of the review (article selection, data abstraction, quality assessment of the included studies), and this constitutes a limitation of the study.
The heterogeneity between studies on key issues such as hospital discharge components, study designs and outcomes (including follow-up durations), prevents quantitative synthesis and hampers consistent assessment of the impact of discharge organisation on patient health.
Introduction
Rationale
Since the pioneering studies of Forster et al1 ,2 in which around 20% of patients were reported to have experienced an adverse event within 2 weeks of hospital discharge, several studies have documented the rates of adverse health outcomes, such as emergency department visits and hospital readmissions, occurring during the post-discharge period.3–5 Therefore, return to home after a hospital stay should not viewed by hospital staff as the completion of patient management. Ideally, scheduling outpatient follow-up visits, promoting direct communication with primary care providers and ensuring transmission of the discharge summary, notifying pending test results at discharge, and, if necessary, arranging or suggesting outpatient post-discharge investigations, are various elements of the continuity of care after discharge that should be integrated within the hospital discharge process. Consequently, hospital discharge and subsequent continuity of care are complex interrelated processes involved in a patient's transition from hospital to home. One can hypothesise that some components of discharge organisation affect, at least partially, patients' subsequent healthcare, for example, the rate of rehospitalisation.
Several observational studies have highlighted deficiencies in the transition of care from the inpatient to the outpatient setting. Such studies focused on various aspects related to direct communication between inpatient and outpatient healthcare providers,6 ,7 discharge summaries (content, timeliness, transmission to an outpatient physician),8 ,9 traceability and follow-up providers' information on pending test results at hospital discharge,10 ,11 non-completion of recommended outpatient work-ups (diagnostic procedures, subspecialty referrals and laboratory tests) after hospital discharge,12 medication errors (omission or unjustified prescription) in discharge summaries,13 ,14 drug-related problems after discharge15 ,16 and post-discharge follow-up outpatient visits.17 ,18 Only a few observational studies have investigated the potential association between elements of the hospital discharge process (and subsequent continuity of care) and patient health outcomes,19–21 and their reports are conflicting as regards the effect of such processes on patient health after discharge. Moreover, these studies considered patients with various admissions sources and/or discharge locations, not only their home, before and after hospital discharge. Other studies aimed at exploring the perspectives of hospital staff and/or primary care providers,22–24 or patient opinions,25–27 or both,28 ,29 on hospital discharge and subsequent continuity of care. In particular, few studies have explored the association of such opinions on patient health outcomes such as rehospitalisations30 ,31 or rehospitalisations and emergency department visits.32
Finally, several reviews33–45 examined the effect of various interventions related to hospital discharge. One review was not a systematic review but highlighted several challenges, not necessarily directly focused on patient health outcomes.33 Three reviews concerned interventions on medication reconciliation at discharge,34–36 and in two of them,34 ,35 studies involving medication reconciliation at admission or during hospitalisation were also included. One review only concerned older patients with congestive heart failure and considered only interventions combining comprehensive discharge planning with post-discharge support.37 Two reviews focused on a single outcome, the rehospitalisation rate at 30 days after discharge.38 ,39 Conversely, one review focused on a single discharge component, telephone follow-up.40 There were four reviews in which some41–43 or all44 outcomes considered were not patient health measures, for example, discharge destination,41 ,42 length of stay,41–43 patient or health provider satisfaction41–43 and organisational outcomes (timeliness, accuracy, completeness and overall quality of the information transfer).44 One review categorised interventions according to the timing of these pre-discharge, post-discharge and bridging interventions, and included studies in which the destination of patients after discharge could be a nursing home or skilled nursing facility.45
As regards results obtained, the review on telephone follow-up interventions40 as well as the three reviews examining interventions related to medication reconciliation34–36 indicated that it was not possible to link these interventions to clinically significant improvements. Similarly, the review focusing on the 30-day readmission outcome was negative.38 Three reviews41 ,42 ,45 paint a rather mixed picture: the effectiveness of interventions on patients' health was not clearly demonstrated, and was at best modest. Three reviews37 ,39 ,43 were more positive. First, based on the selection of randomised trials in which the intervention under study explicitly described one or more components that aimed to improve the handover of care between hospital and primary care providers during hospital discharge, the review of Hesselink et al43 indicates that a significant effect was found in favour of the intervention for one or several outcome measures in 25 of the 36 studies. Second, the systematic review of Phillips et al37 reports that comprehensive discharge planning plus post-discharge support for older patients with congestive heart failure resulted in a 25% reduction in the relative risk of readmission, considering studies with a follow-up ranging from 3 to 12 months. Third, based on the inclusion of 42 randomised trials, with most studies relating to populations of patients at high risk, the meta-analysis of Leppin et al39 indicates that peri-discharge interventions are associated with a reduction in the rehospitalisation rate at 30 days after discharge.
The perspectives varied widely from one review to another as regards the elements of the discharge process explored, the targeted population, the outcome(s) considered (including follow-up duration) and patient location after discharge. Considering the common case of a standard hospitalised patient from the general population returning home after discharge, the simple question ‘Are there some discharge components specifically associated with health outcomes?’, is not answered in the available reviews. De facto, we failed to identify a work providing a synthesis of the available knowledge on this question.
Objective
We conducted a systematic review to explore the potential association between elements of the hospital discharge process (including post-discharge continuity of care) and adverse outcomes (including healthcare resource consumption) in the post-discharge period, in a standard population of patients returning home.
Methods
The reporting of the systematic review is based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines46 (see online supplementary file 1).
supplementary file
Eligibility criteria
The predefined study inclusion and exclusion criteria are detailed in online supplementary file 2.
supplementary file
Information sources
Initial searches in the databases were conducted between 1 March 2013 and 30 June 2013, with no limit considered for the start date, and all searches were updated on 13 July 2016. A combined search in the Medline database via PubMed and in the Web of Science was performed, using different search terms to cover exploration of the organisational process for hospital discharge and subsequent continuity of care. Four independent searches were conducted, which focused on discharge summary, medication reconciliation procedures (preferably at hospital discharge), global organisation of the discharge process and subsequent continuity of care, and care transition. We screened the bibliographies of review articles detected during the database searches (which were not eligible for inclusion) to identify any additional studies that had been missed during the database searches.
Search strategies
The queries made in the Medline and Web of Science databases are detailed in online supplementary file 3.
supplementary file
Study selection
The eligibility of each retrieved article was assessed by one author (BC) in terms of its title, abstract and, if necessary, the full text. We decided a priori that in the case of doubt, a second reviewer (GH) would decide whether to include the study. The bibliography of each included study was screened to potentially identify any studies missed in the database searches. Whenever this resulted in the identification of an additional study, this screening process was repeated until no additional study was found.
Data collection process
The data collection process was conducted (by BC) using a standardised predefined data collection sheet and extracted data were checked.
Data items
The following information was extracted from each of the studies included: name of first author, journal, year of publication, component(s) of the discharge process investigated, study design, objective(s), setting, participants, sample size, method(s), description of the intervention and comparator (if applicable), main outcome measures, results, synthesis of the major results (ie, significant association or not between the component(s) of the discharge process investigated and patient health outcomes) and study limitations.
Risk of bias in individual studies/quality assessment
The methodological quality of the selected studies was evaluated (by BC) using two tools that have been proposed for assessing studies when the considered study set includes major differences in terms of experimental design (nb, we formalised a priori that in the case of doubt when rating the methodological quality of a study, a second author (GH) would be solicited for this rating). First, the Quality Assessment Tool for Quantitative Studies47 ,48 rates study global quality as strong, moderate or weak. Second, the Mixed Methods Appraisal Tool–V.201149 grades the studies according to five categories, ranging from 0% (research questions not clearly stated), low (score=25%), moderate (score=50%) and high (score=75%) to very high (score=100%) methodological quality. Both tools have strengths and weaknesses. For example, the Quality Assessment Tool for Quantitative Studies automatically assigns a strong score to randomised controlled trials, irrespective of the quality of randomisation method and allocation concealment, while the Mixed Methods Appraisal Tool is limited to the evaluation of four items. Studies were finally ranked into three categories (weak, moderate or strong) according to a combination of the ranks determined by each of the two tools: in a first step, low and very low, moderate, and high and very high rankings with the Mixed Methods Appraisal Tool were recategorised as weak, moderate and strong, respectively, and then, the final ranking of a given study was chosen as the lowest rank of the two tools.
Summary measures and synthesis of results
A standard quantitative synthesis, that is, a meta-analysis, was deemed not to be appropriate because of wide variability in study designs, types of intervention (if applicable) and outcomes. Nevertheless, a synthesis of the results from the observational and interventional studies has been conducted and presented in the form of a summary table and figures with the aim of identifying emerging patterns relating components of the discharge process to patient health outcomes.
Risk of bias across studies
The possibility of publication bias resulting in more positive than negative studies being published may have affected the results of our review but could not be assessed.
Additional analyses
No prespecified additional analysis was performed.
Results
Study selection
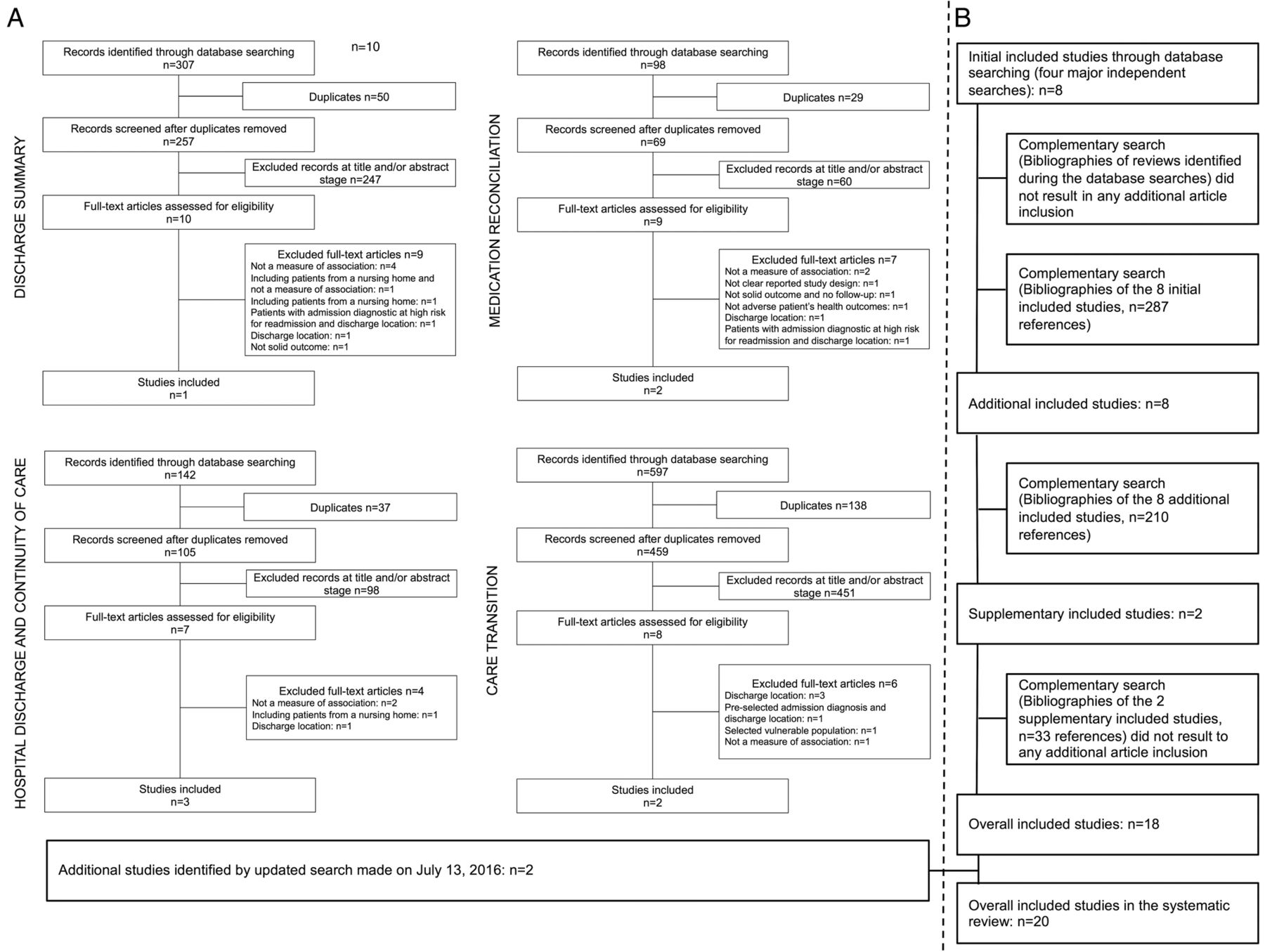
The results of the eight initial independent searches (four major queries in each of the databases) identified 1144 publications, 890 after excluding 254 duplicates, of which eight studies were initially included (see online supplementary file 4 that indicates the references of full-text articles excluded and details the corresponding reason) (figure 1). Screening the bibliographies of the initial included studies resulted in the inclusion of 10 additional studies. No additional studies were identified from the bibliographies of reviews identified during the database searches. Thus, the initial set consisted of 18 studies.31 ,50–66 Update of the searches made on 13 July 2016 resulted in the inclusion of two additional studies.67 ,68
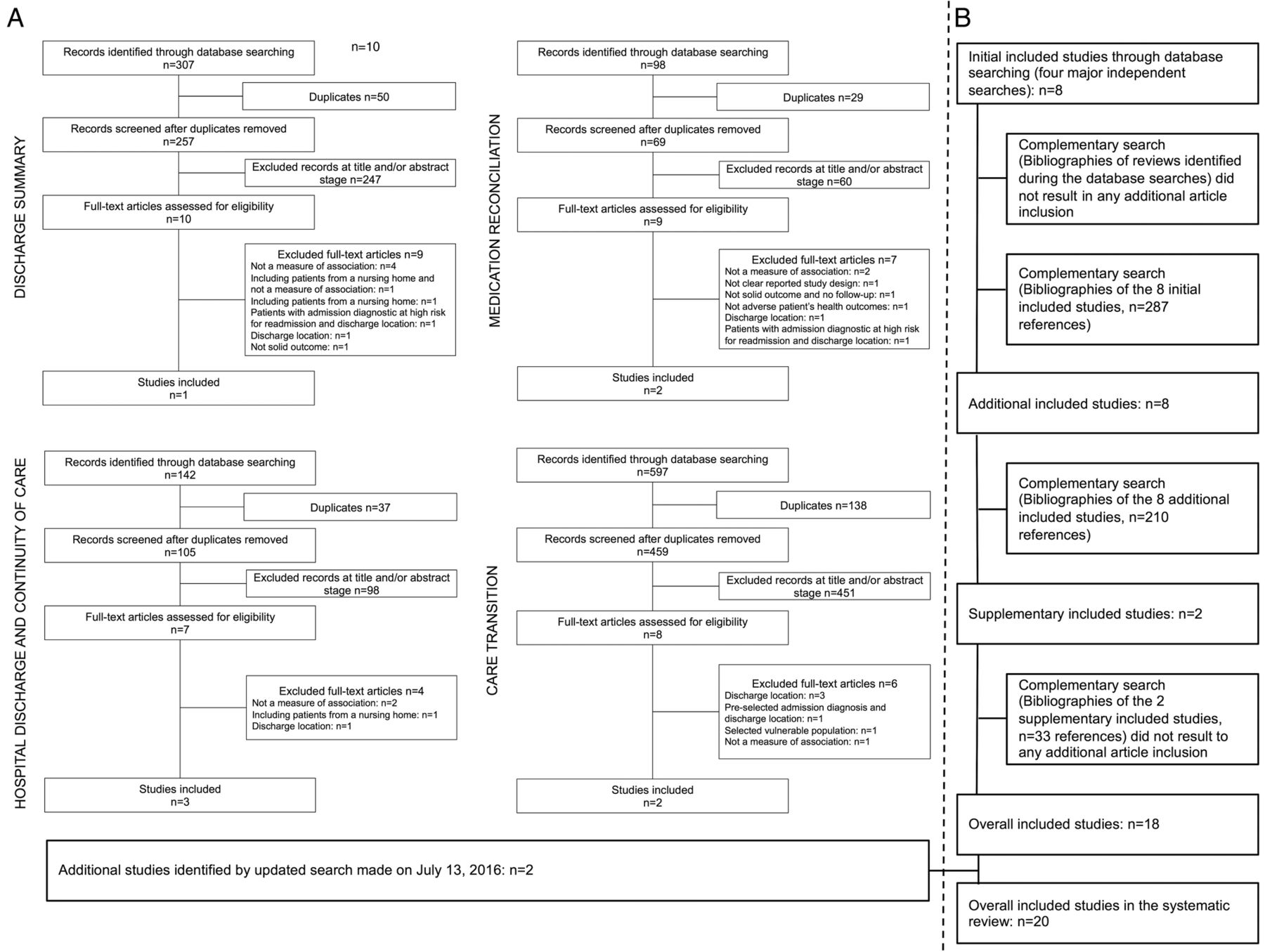
Flow diagram of the systematic review process. (A) Flow diagram of the four independent searches in the Medline and Web of Science databases. (B) Flow diagram of the process for screening the bibliographies of the reviews and initial included studies.
supplementary file
Study characteristics
The study characteristics are summarised in online supplementary file 5. The 20 selected studies were published between 2001 and 2015 and were performed in the USA (n=14), Canada (n=4), Australia (n=1) and the UK (n=1). Eleven studies were observational31 ,50–58 ,67 and nine were interventional59–66 ,68 (including five randomised controlled studies).59–62 ,68 The interventions were mostly multifaceted interventions: four were pharmacist interventions59 ,60 ,63 ,64 and four focused on the transition from hospital to home,61 ,62 ,65 ,66 while only one was an intervention with a single component (a post-discharge phone call).68
supplementary file
In 15 studies, patients were discharged from general medical and/or surgical units. Five studies targeted patients with heart failure,31 ,50 ,51 ,65 ,67 with one study targeting a somewhat larger population.31
Sample sizes ranged from 8363 to 73862 patients for interventional studies and from 8652 to 938 93353 patients for observational studies.
Risk of bias within studies/quality assessment
According to the Quality Assessment Tool for Quantitative Studies, 12 studies were rated as having a strong,31 ,50 ,51 ,53–57 ,60–62 ,67 six a moderate52 ,58 ,59 ,63 ,66 ,68 and two a weak64 ,65 methodological quality (figure 2).

Methodological quality of the studies included. Dotted lines indicate the quality determined from the combination of both quality tools (abscissa and ordinate, respectively).
According to the Mixed Methods Appraisal Tool, seven studies were rated as having a very high,31 ,50 ,53–56 ,62 three a high,51 ,52 ,67 six a moderate,57 ,58 ,60 ,61 ,63 ,66 three a low64 ,65 ,68 and one a very low59 methodological quality (figure 2).
When the two quality tools were combined, nine studies were rated as having a strong,31 ,50 ,51 ,53–56 ,62 ,67 seven a moderate52 ,57 ,58 ,60 ,61 ,63 ,66 and four a weak59 ,64 ,65 ,68 combined methodological quality (figure 2).
Results of individual studies
Components of the discharge process investigated
Five discharge process components were explored primarily: discharge summary (n=2),58 ,67 discharge instructions as mentioned in the medical records (n=2),31 ,51 drug-related problems at discharge (n=4),59 ,60 ,63 ,64 transition from hospital to home (n=5)54 ,61 ,62 ,65 ,66 and continuity of care after hospital discharge (n=7) (table 1).50 ,52 ,53 ,55–57 ,68
Hospital discharge process and subsequent continuity of care, and associated patient health outcomes
Two observational studies58 ,67 investigated the discharge summary component. One study58 examined the timeliness of discharge summary finalisation and the other67 investigated the timeliness, documented transmission to the follow-up physician and content of the discharge summary. This component was also explored in two other studies54 ,57 in combination with other components of the hospital discharge process. In particular, the availability of the discharge summary to the physician during post-discharge visits was investigated.
The component relating to documentation of discharge instructions provided to patients was explored in two observational studies,31 ,51 and both concerned patients with congestive heart failure.
Drug-related problems were addressed via the assessment of a pharmacist intervention in four studies.59 ,60 ,63 ,64 The type and number of intervention elements (eg, pharmaceutical counselling, education, medication review, medication reconciliation, follow-up with a pharmacist after discharge) varied between studies. Similarly, the component ‘transition from hospital to home’ was explored mainly in four interventional studies,61 ,62 ,65 ,66 with the number and type of intervention elements (eg, patient therapeutic education, medication reconciliation, post-hospitalisation follow-up) varying between studies. Only one observational study54 explored the transition from hospital to home, focusing on different aspects of the communication between hospital staff and primary care physicians (primary care physician's awareness of his or her patient's hospitalisation, receipt of a discharge summary, direct exchanges with the multidisciplinary hospital team).
In contrast, except for a single interventional study that explored the impact of a post-discharge phone call,68 the component ‘continuity of care after discharge’ was investigated exclusively in observational studies. The elements targeted in these studies were documented follow-up appointment arrangements scheduled before discharge,55 timing of outpatient follow-up after discharge,50 ,56 post-discharge follow-up by hospital physicians or general practitioners,53 a score for continuity of care,57 and medical errors related to discontinuity of care from the inpatient to the outpatient setting.52
Patient health outcomes after discharge
The major outcomes measured in the included studies were, in order of frequency, rehospitalisations (n=18),31 ,50–52 ,54–59 ,61–68 emergency department visits (n=8)54 ,55 ,59 ,61 ,62 ,64 ,66 ,68 and mortality (n=5) (table 1).50 ,51 ,54 ,55 ,57 Two studies investigated only composite outcomes: emergency department visits or rehospitalisations,60 and rehospitalisations or mortality.53 In addition, six studies investigated outcomes separately and in combination: emergency department visits and/or rehospitalisations,55 ,62 ,64 ,66 rehospitalisations or mortality,50 and emergency department visits or rehospitalisations or mortality.54
The rate of post-discharge visits to a general practitioner was another, less frequently, measured outcome.61–63 This outcome was considered from a different perspective in each of three studies: unplanned visits to a general practitioner,63 no outpatient follow-up within 21 days61 and follow-up visits with the primary care provider.62
Follow-up duration after discharge varied from 7 days58 to 12 months51 for rehospitalisations, from 72 hours64 to 31 days61 for emergency department visits, from 30 days50 ,54 ,55 to 12 months51 for death, and from 15 days63 to 3 months63 for visits to the general practitioner.
Synthesis of results
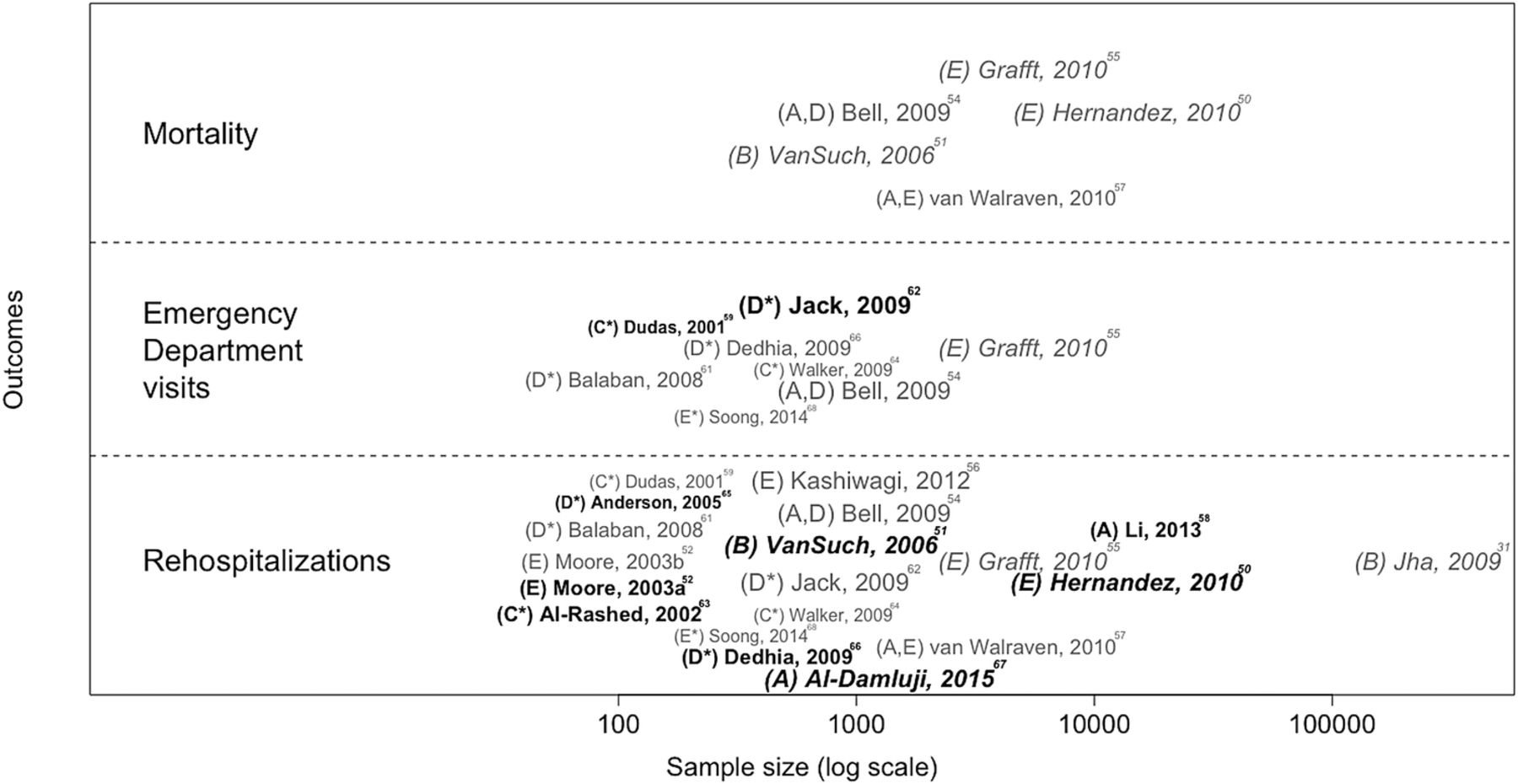
The included studies were published within the past 15 years, suggesting a relatively recent area of investigation. Whereas the studies' underlying healthcare organisations were relatively homogeneous (with most studies originating from the USA), the components of the discharge process investigated were not (see online supplementary file 5). Even when considering a given component category, the variable of interest and the associated investigation method varied widely across studies, including follow-up duration for assessing patient outcome (see table 1), which precluded us from performing a meta-analysis that would generate meaningful results. Nevertheless, the effect of components of the discharge process on the main patient health outcomes is described in figure 3.

Effect of hospital discharge process and subsequent continuity of care components on patients' health outcomes. The letters in parenthesis correspond to the type of component investigated: A, discharge summary; B, discharge instructions; C, drug-related problems; D, transition from hospital to home; and E, continuity of care. In addition, interventional studies are identified by an asterisk. Studies in bold and normal characters indicate significant and non-significant associations reported, respectively. Studies in italic characters indicate studies involving patients with heart failure. Small, medium and large sized characters indicate a weak, moderate and strong methodological quality. Moore, 2003a refers to the measured outcome of rehospitalizations related to work-up errors. Moore, 2003b refers to the measured outcomes of rehospitalisations related to medication continuity errors and to test follow-up errors.
In 13 studies,50–53 ,55 ,58 ,59 ,61–63 ,65–67 at least one significant association was reported between component(s) of the hospital discharge process and any patient health outcome explored, irrespective of the type of outcomes and the follow-up duration.
Of the 18 studies31 ,50–52 ,54–59 ,61–68 that explored the potential association between hospital discharge process and rehospitalisations, 7 reported a significant association,50 ,51 ,58 ,63 ,65–67 while 10 reported a non-significant association.31 ,54–57 ,59 ,61 ,62 ,64 ,68 The remaining study52 evaluated three types of medical errors (work-up errors, medication continuity errors and test follow-up errors) related to the discontinuity of care from the inpatient to the outpatient setting and found a significant association only between work-up errors and rehospitalisations. When the analysis was restricted to the 14 studies31 ,50 ,54–56 ,58 ,59 ,61–64 ,66–68 that investigated rehospitalisations within approximately 30 days of discharge (including 15–22 days,63 28 days58 and 31 days61), five studies50 ,58 ,63 ,66 ,67 reported a significant association between this outcome and the hospital discharge process, while nine31 ,54–56 ,59 ,61 ,62 ,64 ,68 reported a non-significant association.
Of the eight studies54 ,55 ,59 ,61 ,62 ,64 ,66 ,68 (six of which were interventional studies)59 ,61 ,62 ,64 ,66 ,68 that investigated post-discharge visits to the emergency department as an outcome, two interventional studies59 ,62 reported a significant association between this outcome and the investigated intervention.
The five studies that investigated patient mortality50 ,51 ,54 ,55 ,57 were all observational, and all reported no significant association between discharge process and death.
Eight studies50 ,53–55 ,60 ,62 ,64 ,66 explored a composite outcome (mostly based on 30-day follow-up duration, n=7), the nature of the combination varying from one study to another (table 1 and figure 4). The association between component(s) of the discharge process and subsequent continuity of care and the composite outcome was reported as significant in four studies50 ,53 ,62 ,66 and as non-significant in three studies.54 ,60 ,64 In the remaining study,55 there was no significant association between documented follow-up appointment arrangements and rehospitalisations or emergency department visits within 30 days. However, documented follow-up appointment arrangements were significantly associated with a higher likelihood of having either an emergency department visit or a hospital readmission within 180 days of the initial hospital discharge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of hospital discharge process and subsequent continuity of care components on patients' composite health outcomes. The letters in parenthesis correspond to the type of component investigated: A, discharge summary; B, discharge instructions; C, drug-related problems; D, transition from hospital to home; and E, continuity of care. In addition, interventional studies are identified by an asterisk. Studies in bold and normal characters indicate significant and non-significant associations reported, respectively. Studies in italic characters indicate studies involving patients with heart failure. Small, medium and large sized characters indicate a weak, moderate and strong methodological quality. The follow-up duration in each study is indicated, for example ‘30d’ indicates that the follow-up reported is the post-discharge period of 30 days. ED, emergency department.
Finally, figures 3 and 4 indicate that irrespective of the component explored, one cannot identify any consistent statistical association between any hospital discharge component and any patient health outcome.
Risk of bias across studies
Risk of bias across studies was especially difficult to evaluate because of the wide heterogeneity between studies (eg, design, sample size, hospital discharge components, outcomes, follow-up duration). Any correction of a potential publication bias against studies with negative or non-significant associations would have reduced the variability found in this review, with a corresponding mechanic effect favouring consistent absence of an association between discharge organisation and subsequent patient health.
Additional analyses
No additional analysis was performed.
Discussion
Summary of evidence
The major outcomes used to estimate the effect of the discharge process and subsequent continuity of care on patient health after discharge were rehospitalisations and emergency department visits, most commonly measured at approximately 30 days after discharge. Eight of the 18 studies that explored rehospitalisations reported at least one significant association between discharge process and this outcome, while two of the eight studies that investigated emergency department visits reported a significant association. No study reported a significant association between a discharge component and mortality. This systematic review highlights a wide heterogeneity across the studies, especially in terms of the component(s) of the hospital discharge process investigated, study designs and outcomes measured (including follow-up durations). Such a heterogeneity in critical elements prevents a meaningful meta-analysis from being performed. Nevertheless, figures 3 and 4 indicate globally that irrespective of the component of the discharge process explored, outcome considered, sample size or study design, one cannot identify any consistent statistical association between the presence of a component or an intervention likely improving the quality of the hospital discharge process and an improvement in a patient health outcome. The global picture from our review indicates that the effect of discharge process and subsequent continuity of care components on patient health after discharge remains unclear. Therefore, it is not possible to draw any conclusions about the most critical organisational discharge process components on which to base potential recommendations. This contrasts with the review of Leppin et al39 which indicates that peri-discharge interventions targeting specific populations were effective at reducing hospital readmissions. At least three factors may be contributing to this difference: the heterogeneous general population that was targeted in our review might require very large sample sizes to produce evidence of a comparable impact, personalised interventions in specific populations might be more efficient, and finally study designs involved in our review include observational studies whereas Leppin et al39 only considered randomised trials. In any case, a major implication of our findings is that better standardisation should be used in future studies in order to get a clearer picture of the impact of discharge elements on the general population of patients. For example, a 30-day readmission delay could be considered as a reasonable standardised outcome (long-term outcomes are probably more liable to be biased by confounding factors).
Among the 20 studies included in this review, nine described interventions, only five of which were randomised trials; this finding raises concerns about the potential effect of confounding factors that might have influenced patient outcomes after discharge. Indeed, in many of the studies, features related to elements of the patients' hospital stay (such as disease progression, severity of illness and comorbidities), which were unrelated to discharge components, may have contributed to patients' health outcomes after discharge.
Another concern is the variability of discharge protocols from one hospital department to another. Such protocols are poorly reported in the studies.50 Although 18 of the 20 studies were conducted in the USA (n=14) or Canada (n=4), between-protocol variability might result in variability in the effect of the hospital discharge process on a patient's subsequent health. General recommendations for managing the hospital–primary care interface have been proposed by several societies,69 as well as discharge checklists.70 ,71 Similarly, Kripalani et al33 attempted to identify challenges and to propose recommendations, given the lack of evidence-based recommendations for hospital discharge applicable to a broad range of patients. However, the rate of adoption of standardised evidence-based recommendations in health organisations remains unknown.
Limitations
This review is subject to several limitations. First, a single author was involved in critical steps of the review (initial phases leading to article selection, data abstraction and risk assessment of the included studies). This constitutes a significant risk for individual and systematic bias, and thus is a major limitation of this systematic review.
The second limitation concerns the potential omission of relevant studies. However, our iterative process of screening the bibliographies of included studies is likely to have minimised this limitation. Of note, we did not identify any new studies when we searched the bibliographies of reviews identified during the database searches.
The third limitation concerns the populations studied. The inclusion criteria restricted the analysis to studies on general medical or surgical patients originating from home and discharged to home. Studies on specific populations were excluded, but we decided to keep studies involving patients with heart failure given the prevalence of such patients and the substantial volume of literature available on hospital discharge and continuity of care. However, removing the five studies31 ,50 ,51 ,65 ,67 involving these patients, shown in italic in figures 3 and 4, would not resolve the above-mentioned absence of identification of any consistent pattern. Moreover, despite the exclusion of studies that were focused on specific populations (see exclusion criterion no. 7 in online supplementary file 2), some of the studies included in the review may not have excluded or measured as a covariate any factor related to frailty or socio-economic status and this may have contributed to the heterogeneity of the results.
The fourth limitation was the heterogeneity revealed by our synthesis of the results. This heterogeneity may be linked to the fact that the processes investigated were complex, multifaceted and interconnected. Previous reviews in the domain of hospital discharge process and continuity of care also report such heterogeneity,35 ,36 ,38 ,40–45 likewise attested by the fact that only three reviews performed meta-analyses.37 ,39 ,42
The fifth limitation was the limited scientific evidence of the included studies, given the various designs. Unsurprisingly, studies with a high sample size were observational. Assessment of the methodological quality of the studies indicated that only 9 of the 20 studies were categorised as having a strong score in terms of methodological quality (see figure 2). Finally, one cannot exclude a risk of publication bias against studies that did not find an association between hospital discharge component(s) and patient health outcome(s).
Conclusions and perspectives
This systematic review highlights the wide heterogeneity between studies evaluating the effect of the hospital discharge organisation process on patients' outcomes after discharge in a standard population of patients returning home. The role of this heterogeneity in the variance observed in the study results (ie, either a positive effect or absence of effect) is unknown. Globally, the effect of the complex interrelated hospital discharge and continuity of care processes on patient health outcomes requires further investigations, but because of the inherent multicomponent nature of these processes and the interweaving of these processes in the entire hospital stay, estimating such an effect is difficult. To obtain a clearer global picture, future studies would benefit from better standardisation of the adverse outcomes explored, including follow-up duration. In addition, technological developments may enhance overall management of patients at the hospital–primary care interface. A major challenge concerns the interoperability between hospital and primary care electronic health information systems, for facilitating exchanges of hospital–primary care information. Moreover, implementation of information systems collecting patient opinions after hospital discharge may document important information on current organisation, and constitute the basis of systems devoted to improving management.
Acknowledgments
Sophie Rushton-Smith, PhD (Medlink Healthcare Communications Limited) provided editorial support on the final version of the article and was funded by the authors.
References
Footnotes
Contributors Study conception and design: BC, FC and GH; data acquisition: BC; analysis and interpretation of data: BC and GH; writing of the first draft of the paper: BC and GH; all authors read and approved the final version of the paper.
Funding This work was supported by a grant from Assistance Publique-Hôpitaux de Paris, programme ‘Recherche Infirmière’ (BC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.