Article Text

Abstract
Objectives To study patient selection for and persistence with ADP receptor-inhibiting oral antiplatelet (OAP) treatment after acute coronary syndrome (ACS).
Design Observational, retrospective, cohort study linking real-life patient-level register data.
Setting Nationwide drug usage study using data of patients with ACS discharged from hospitals in Finland.
Participants The study population consisted of 54 416 patients (aged ≥18 years) following hospital admission for unstable angina pectoris or myocardial infarction during 2009–2013. Patients were classified as either OAP or non-OAP users based on drug purchases within 7 days of discharge.
Outcome measures Initiation of and a 12-month persistence with OAP medication.
Results In total, 49% of patients with ACS received OAP treatment after hospital discharge. Women represented 40% of the population, but only 32% of them became OAP users (adjusted OR for initiation compared with men 0.8; p<0.001). Patients not treated with percutaneous coronary intervention (PCI), elderly and patients with dementia/Alzheimer's disease, atrial fibrillation or warfarin treatment were less likely to be treated with OAP. If initiated, they were less likely to complete the recommended 12 months’ medication (adjusted risk increment >38% and p<0.001 for all). The OAP users showed good compliance with immediate initiation (92% within 1 day of discharge) and high mean medication possession rate (99%). Among OAP users, the usage of other secondary prevention drugs after ACS was more common than in non-OAP-treated patients (difference >20 percentage points for each).
Conclusions Only half of the patients with ACS received guideline-recommended ADP receptor-inhibiting OAP treatment after hospital discharge, suggesting suboptimal treatment practices. Non-PCI-treated patients and patients with increased age, unstable angina, dementia or atrial fibrillation appear to have the highest risk of deficient treatment with OAPs. OAP users, however, showed good compliance during drug usage.
- oral antiplatelet
- drug utilization
- persistence
- unstable angina pectoris
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Nationwide register data, population-wide coverage.
Sophisticated methodology in drug exposure measurements.
Detailed clinical data (weight, laboratory samples, blood pressure, etc) are not available.
Introduction
Recurrent ischaemic events are frequent after acute coronary syndrome (ACS), but sudden cardiac deaths have become less common.1 ,2 Progress has been made in the invasive treatment and general management of ACS, particularly related to health promotion activities and pharmacotherapy optimisation in secondary prevention.3 Outpatient education also improves adherence to cardiovascular pharmacotherapy.4
Recent improvements in clinical outcomes of patients with ACS are largely attributable to progress made in antiplatelet therapy. Dual antiplatelet treatment with low-dose acetylsalicylic acid (ASA) and ADP receptor P2Y12-inhibiting oral antiplatelet agent (OAP) improves outcomes after ACS.5–7 Guidelines recommend OAP to be maintained for 12 months in invasively and non-invasively treated patients after ACS, unless contraindications, such as a high risk of bleeding, are present.8 ,9 Short-term outcomes of ACS are better if in-hospital medication is in line with guidelines,10 and the suboptimal usage of guideline-recommended medications and interventions is associated with increased mortality rates in patients with myocardial infarction.11
Compliance to OAP medication after hospital discharge is essential in preventing adverse outcomes, such as stent thrombosis.12 ,13 In addition to clopidogrel, new potent OAPs, prasugrel and ticagrelor, have been introduced for ACS treatment.8 ,9 The use of these multiple OAP treatment options in clinical practice is, however, not known. Previously, only about 70% of the patients have been reported to fill the prescriptions of cardiovascular pharmacotherapy after the first month following acute myocardial infarction.4 In order to improve adherence to secondary prevention medication, it is imperative to know patient characteristics associated with lower OAP treatment initiation and persistence.
The aim of this nationwide drug usage database study was to study clinical characteristics in association with real-life patient selection and switch patterns of, persistence with, and compliance to OAP treatment after ACS.
Patients and methods
Data sources
This observational, retrospective, cohort study was conducted by linking patient-level data from different nationwide administrative healthcare registers in Finland. Diagnoses, interventions and hospitalisation periods were extracted from the Finnish Care Register for Healthcare, dispensed prescriptions and certain special reimbursement statuses from the Prescription Register. Data for institutionalisation periods other than hospitalisation (Care Register for Social Welfare), living abroad (places of domicile) and for possible mortality (Statistics Finland) were also acquired from the authorities in order to interpret the gaps in drug exposure and persistence with treatment.
Study population
The study population consisted of patients discharged from Finnish hospitals following admission for unstable angina pectoris (International Classification of Diseases (ICD)-10 code: I20.0) or myocardial infarction (ICD-10 code: I21) between 1 January 2009 and 15 December 2013. The first ACS event during the study period was considered the index event. Patients under 18 years old were excluded. The study focused on mainland Finland excluding the autonomic Aland Islands.
Patients were classified as OAP-treated or non-OAP-treated based on their drug purchases within 7 days of discharge. Comorbidity data were searched for 5 years prior to index event (including all-level diagnoses in the hospital care data, special reimbursements statuses for treatment of chronic diseases and certain long-term drug treatments for chronic diseases). The patients were followed up until end of the study, moving abroad or death.
Drug exposure
Prescription Register searches were based on the Anatomical Therapeutic Chemical Classification System (ATC coding). OAPs of interest were clopidogrel (B01AC04), prasugrel (B01AC22) and ticagrelor (B01AC24). The duration of OAP medication was based on the number of purchased tablets, because after the initiation dose given in the hospital, the daily dosing is uniform for all patients: one tablet of clopidogrel (75 mg), one tablet of prasugrel (either 5 mg or 10 mg), and two tablets of ticagrelor (90 mg). Exposure measurements for other drugs were based on defined daily doses (DDDs). Baseline medication history data were scrutinised for 120 days prior to index event hospitalisation and secondary prevention drug purchases (other than OAPs) for 30 days after the index date. For patients with previous use of these drugs, purchases were scrutinised for 90 days post event, as this is the length of possible drug possession period according to Social Insurance Institution guidelines.
For OAPs, treatment gaps up to 30 days were considered representative of continuous treatment. Hospitalisation and institutionalisation periods were taken into account when ignoring these gaps. Medication possession rate (MPR) of OAP treatment was measured from discharge to the last day of medication. MPR and time to initiation were used as factors to estimate OAP compliance.
Statistical methods
Adjusted ORs and 95% CIs for the probability of OAP treatment initiation within 7 days of discharge after the index ACS event were estimated using logistic regression. Kaplan-Meier curves were used to illustrate OAP persistence (the total duration of time from initiation to discontinuation). The Cox proportional hazards model was used to estimate the HRs and the 95% CI for the risk of OAP treatment discontinuation within 350 days from treatment initiation. The ORs and HRs were adjusted for age, sex, ACS type, invasive procedure type, hospital type, geographical hospital region, comorbidity history, Charlson Comorbidity Index, medication history and calendar year. Statistical significance was inferred at p<0.05. All data management and statistical analyses were performed using R programming language.14
Ethical aspects
This was a non-interventional register-based study without any patient contacts. The study was conducted by following the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) Code of Conduct and Guidelines for Good Pharmacoepidemiology Practice (GPP).15 ,16 The study was registered into the EUPAS e-register (EUPAS6161). The protocol is available online via ENCePP: http://www.encepp.eu/encepp/openAttachment/fullProtocolLatest/7228 (accessed 12 Feb 2016). Data permits were applied for from each registry holder separately: National Institute for Health and Welfare (THL/522/5.05.00/2014), Social Insurance Institution (Kela 21/522/2014) and Statistics Finland (TK-53-532-14). The identification numbers of the patients were encrypted by the registry holders before data delivery to the researchers.
Results
Cohort entry and index event
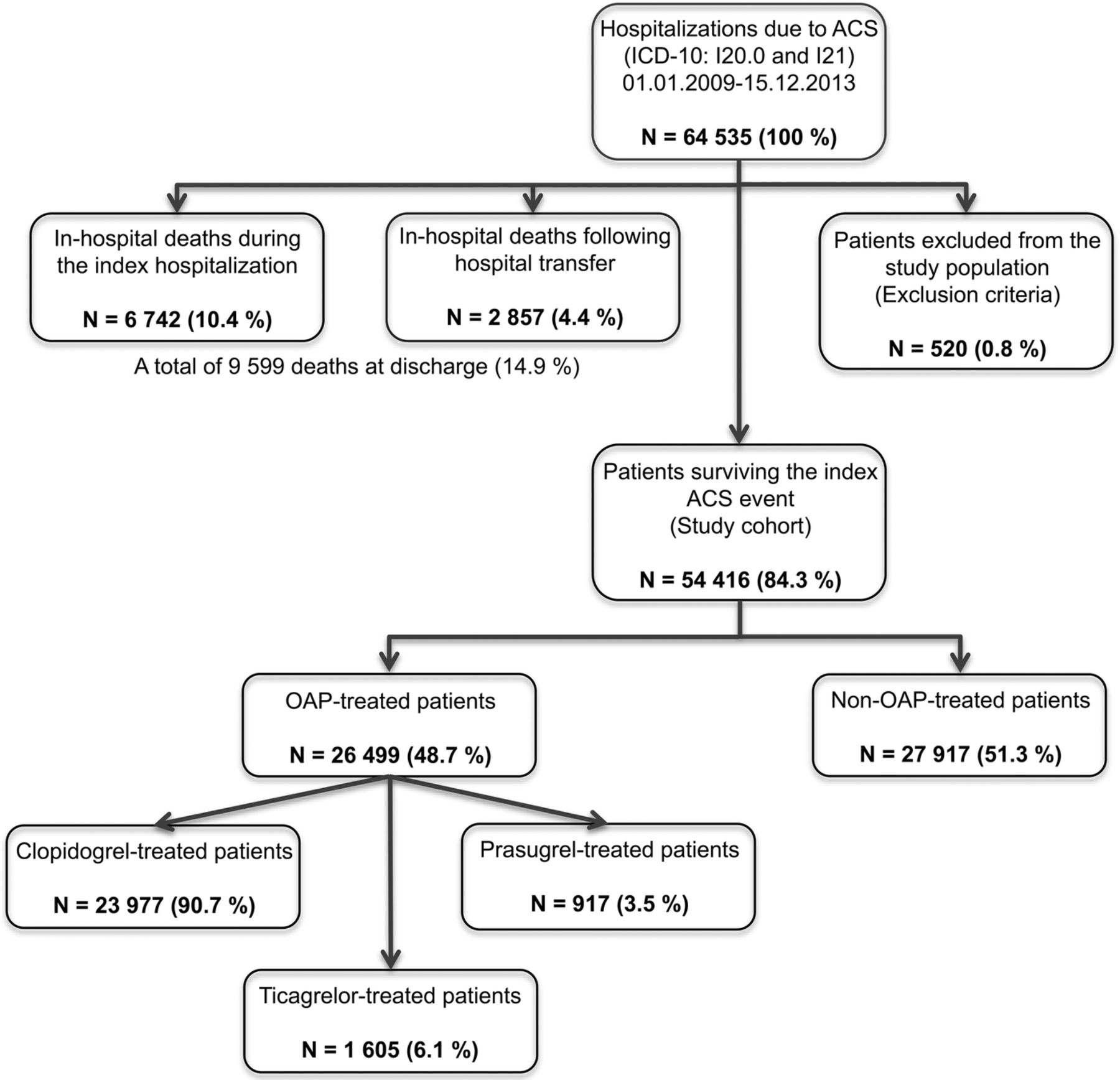
Figure 1 shows a flow chart about the patients forming the study population. The final study cohort consisted of 54 416 patients with ACS. Of the cohort, 49% (N=26 499) were treated with OAPs while 51% (N=27 917) formed the non-OAP-treated group. Of the OAP-treated patients, 91% (N=23 977) received clopidogrel within 7 days of discharge; 6.1% of the patients formed the ticagrelor group and 3.5% the prasugrel group. In 2013, when all three OAPs were available, the proportions were 74% for clopidogrel, 6.2% for prasugrel and 20% for ticagrelor. In 95% of the cases, there was no previous OAP treatment.

Population flow chart.
Patients were older (mean age 76 years) in the non-OAP-treated group compared with the OAP-treated group (mean age 68 years; p<0.001), patients in the prasugrel group being the youngest (mean age 60 years) (table 1). The difference between sexes was smaller in the non-OAP-treated group (53% men) compared with the OAP-treated group (68% men; p<0.001). This was further highlighted in the prasugrel group, in which 78% were men.
Characteristics of the patients at ACS event
The majority of the patients had no history of ACS events. Non-ST elevation myocardial infarction (NSTEMI) was the most common (53%) reason for the index ACS hospitalisation (table 1). ST elevation myocardial infarction (STEMI) was the most common event type (81%) among prasugrel users.
After percutaneous coronary intervention (PCI), OAP was used in 90% of the patients. Prasugrel-treated patients had the highest PCI rate (85%) (table 1). Patients revascularised with coronary bypass grafting (CABG) constituted 7.4% of all patients with ACS and only 13% of these patients were treated with OAPs after discharge. Those not undergoing any invasive procedure frequently did not receive OAP treatment post event (77%). Mean duration of hospital stay due to the index event was 18 days in the non-OAP-treated group (including transfers between hospitals) and 7 days in the OAP-treated group.
Patient selection to OAP and non-OAP users
Elderly patients were less likely to receive OAP treatment than younger ones (OR 0.6; p<0.001 for >85 vs <65 years of age), and the OR for OAP initiation was 20% lower in women (p<0.001) (table 2). STEMI patients had a 2.6-fold and NSTEMI patients 1.7-fold OR for OAP treatment compared with patients hospitalised for unstable angina pectoris (p<0.001 for both). Patients undergoing PCI had significantly higher likelihood of OAP medication (OR 19.5) than patients who did not undergo any invasive procedure, while treatment of ACS with CABG was associated with a very low rate of OAP initiation (OR 0.3 vs no invasive evaluation/treatment) (p<0.001 for both). Dementia/Alzheimer's disease was associated with about 50% decrease in the OR of OAP use. The other major clinical features decreasing OAP use were atrial fibrillation, warfarin medication, major bleedings and heart failure (p<0.001 for all). Previous OAP use predicted OAP treatment after discharge by a 3.7-fold increase compared with those with no OAP medication at baseline (p<0.001). The use of OAPs increased during the study period from 2009 to 2013; the OR for initiation was >1.5 during the last three study years compared with the first study year (p<0.001 for all).
ORs (multivariate analysis) for OAP treatment initiation within 7 days of discharge after the index ACS event
OAP compliance and persistence
As many as 92% of the OAP-treated patients made the first OAP purchase on or 1 day after the day of discharge (table 3). The mean MPR in the OAP-treated population was 99%. It was >98% in men and women, and in all age groups.
Time to initiation from index event and within 7 days of discharge, and medication possession rate (MPR) of the OAPs from discharge to the last day of medication
Patients receiving OAP treatment were more likely to be prescribed other guideline-recommended secondary prevention drugs: statin, β-blocker and ACE inhibitor or angiotensin receptor blocker (ARB) (p<0.001 compared with non-OAP-treated patients) (table 1). A β-blocker was the most commonly prescribed secondary prevention drug in the non-OAP-treated population, while statin was the most commonly prescribed secondary prevention drug in all OAP-treated groups.
Of those prasugrel-treated and ticagrelor-treated patients who switched the original treatment to another OAP (not discontinuing OAP treatment), >99% switched to clopidogrel. Treatment switches were few (1.7% of OAP users), but 15% (N=4249) of the non-OAP users started OAP (93% of them clopidogrel) during the follow-up. The mean time to switch from non-OAP to OAP was 196 days (N=1102 for >180 days).
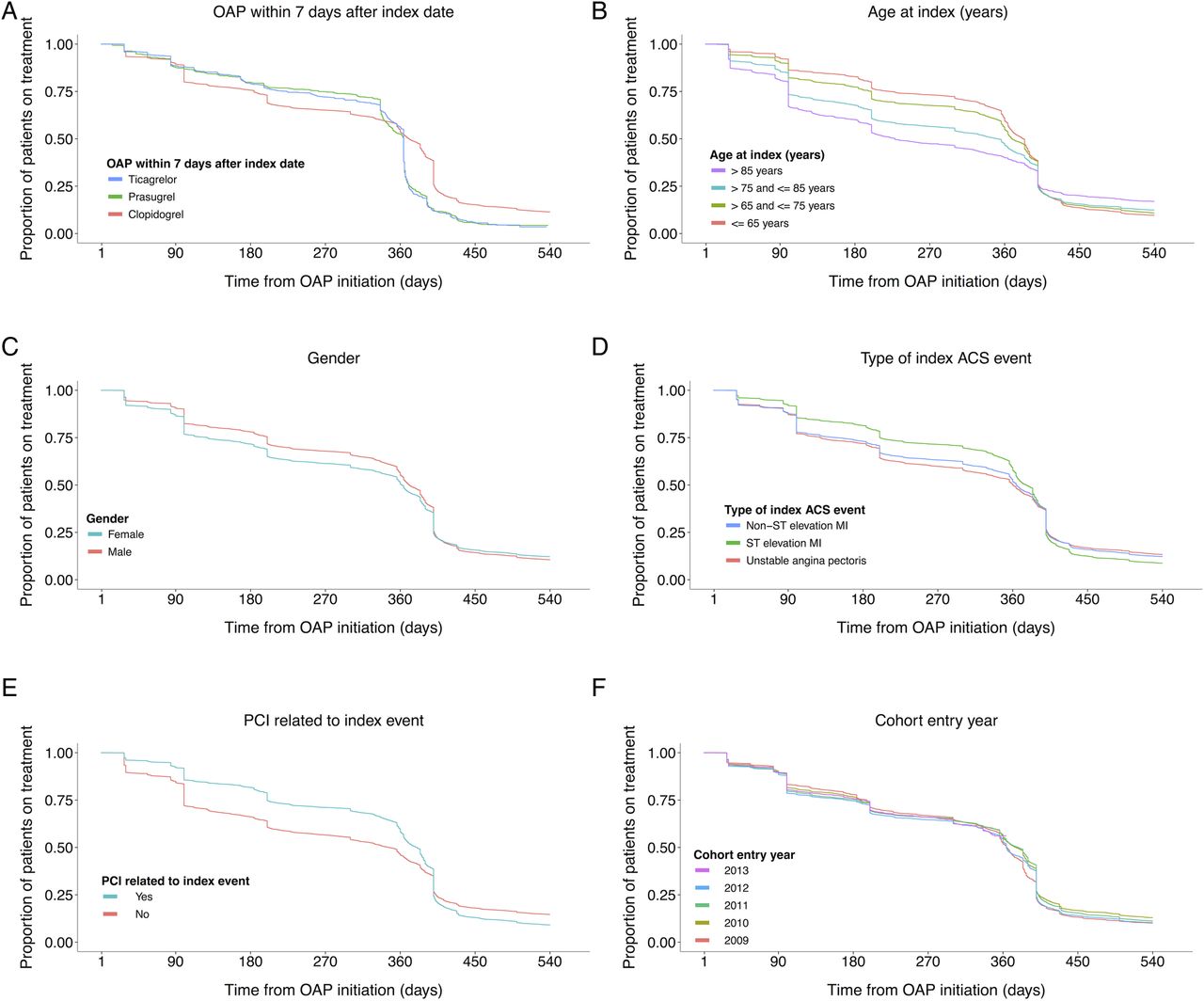
Figure 2A shows the treatment persistence with all OAPs. Ticagrelor and prasugrel followed the same trend: ∼75% of the patients completed their 1-year treatment. For clopidogrel use, there were also persistence drops at 1, 3 and 6 months, and in a minority of patients, clopidogrel was continued longer than 12 months. The package sizes explain why there are certain delays in clopidogrel drops compared to calculated months. Almost 70% of the purchases were 100-pill packages and the 1-year drop in the Kaplan-Mayer curve was at 400 days. On the contrary, in 70% of the prasugrel and ticagrelor cases the 1-year drops were closer to 364 days (13 times 28-pill package). Persistence with the 350-day treatment was higher with clopidogrel than with prasugrel (p<0.001), while no difference was observed between ticagrelor and clopidogrel discontinuation ratios (table 4). The mean follow-up duration for OAP-treated patients, censoring time after OAP discontinuation, was 304 days. In Cox models, censoring time after 350 days, the mean follow-up time was 242 days.
Multivariate HRs for OAP treatment discontinuation within 12 months

{kind=link}
{kind=link}
Treatment persistence stratified by (A) OAP within 7 days after index date, (B) age at index date, (C) gender, (D) type of index ACS event, (E) PCI related to index event and (F) cohort entry year. ACS, acute coronary syndrome; OAP, oral antiplatelet; PCI, percutaneous coronary intervention.
The OAP persistence decreased with increasing age (figure 2B). Patients aged >75 years discontinued their OAP medication before 1 year of treatment more often than those aged ≤65 years (p<0.001) (table 4). Additionally, women had lower persistence with OAP treatment (HR 1.05; 95% CI 1.00 to 1.09; p=0.039) (figure 2C).
The Kaplan-Meier persistence curves stratified by the type of ACS events showed a similar pattern, the one for STEMI associated with the highest treatment persistence (figure 2D). The STEMI patients had a 30% and NSTEMI patients a 17% higher probability of continuing OAP medication up until 1 year (p<0.001 for both) (table 4). Patients who went through PCI and started OAP medication at discharge were 38% more likely to use OAP for 1 year than non-invasively treated patients (p<0.001) (figure 2E). Persistence curves had a similar shape through the study period (figure 2F).
The patients with OAP medication in their regimen prior to the index ACS event were 49% more likely to have continuous OAP treatment for 1 year (p<0.001) (table 4). History of hypertension decreased the likelihood of OAP persistence by 16%, atrial fibrillation by 39% and dementia/Alzheimer's disease by 47% (p<0.001 for all). For patients being treated with warfarin at baseline, the HR for discontinuing the OAP treatment before 1 year was 2.2 (p<0.001).
Discussion
This cohort study comprised 54 000 patients with ACS, of which 80% were hospitalised due to myocardial infarction and 20% due to unstable angina pectoris during 2009–2013. Only half of the patients were OAP users after discharge (51% of the patients with myocardial infarction and 36% of the patients with unstable angina pectoris). Initial compliance is determined early, as over 90% of the OAP-treated patients made their first OAP purchase within 1 day after discharge. After OAP initiation, treatment was rarely switched. Elderly and patients not undergoing PCI were, to a large extent, discharged without OAP, and had an increased risk for shorter duration of OAP treatment. Dementia, atrial fibrillation and unstable angina pectoris were associated with a higher risk of being discharged without OAP and risk of shorter OAP treatment. Our results suggest that when treating patients with ACS, more attention should be paid to initiating appropriate OAP, as well as taking efforts for minimising treatment discontinuation too early despite a significant 67% increase in the adjusted OR of OAP use during the study period.
ACS was invasively treated in about two-thirds of the OAP-treated patients but only 20% of the non-OAP-treated patients. The adjusted OR for postevent OAP use was 19.5 in PCI-treated patients, but those undergoing CABG rarely received OAP treatment with an OR of 0.3 (p<0.001 for both compared with non-invasive procedures). Warfarin treatment and atrial fibrillation were more common in non-OAP-treated patients, and they both decreased the probability of OAP initiation by 40%. Both of these may reflect increased risk of bleeding, and atrial fibrillation and heart failure may be associated with type 2 infarction with no acute coronary lesions.17 ,18 Dementia/Alzheimer's disease was the strongest (50% OR) predictor of non-OAP treatment followed by high Charlson Comorbidity Index. Not surprisingly, the mean age of non-OAP-treated patients was higher and they were more often women.
Hvelplund et al19 have shown that secondary prevention is initiated more often in patients undergoing coronary revascularisation (85–92%) than in those not examined with coronary angiography (46–71%; p<0.001). They also showed that the rate of secondary prevention was higher in men (81–84%) than women (73–79%; p<0.001), but this was associated with the invasive strategy. This study only included patients surviving for at least 2 months, causing respective survival bias. In our study, 43% of the women underwent invasive evaluation or treatment, while the rate for men was 63% (p<0.001). The mean age among women was, however, almost 10 years higher than in men.
Shore et al20 observed the paradox that high-risk patients with myocardial infarction do not receive evidence-based medication as often as lower-risk patients during hospitalisation, and they also question the optimal long-term management of high-risk patients after hospitalisation. In our study setting, we could not collect information on actual OAP prescriptions at discharge, but more than half of the patients did not fill an OAP prescription within 7 days. In comparison to results from Sweden, Norway and Denmark, in which about 70% of the patients received OAP treatment after myocardial infarction, OAP use in this study was low.21–23 Our study, however, also included patients with unstable angina pectoris who were less likely to receive an OAP than patients with myocardial infarction.
In a US cohort of Veterans Affair hospitals during 2005–2010, 7.2% of the patients undergoing PCI did not fill their clopidogrel prescription on the day of discharge.24 This was associated with increased risk of major adverse events. In a UK study, the median time for filling clopidogrel prescription after hospital discharge was 1 day, but one-third of the patients failed to fill their prescription within 3 days.25 The risk of long-term adverse events increased with the time delay and the patients who never filled a clopidogrel prescription were at greatest risk. In our data, only half of the patients with ACS became OAP users after discharge, but of those who did fill the prescription, 90% did it within 1 day.
In this study, the exposure measurements were based on reimbursed drug purchases in Finland. For ASA use, we could not make any estimations, as over-the-counter and non-reimbursed purchases are not registered in the reimbursed prescriptions' database. Medications used during hospitalisations were not available either, but the hospitalisation and institutionalisation periods, as well as moving abroad, were accounted for in the exposure definitions by setting rules for continuous treatment and gaps in the analyses. Ticagrelor has been on the Finnish market since 2010 but the reimbursement status was given in 2012. For prasugrel, we had data from 2010. Clopidogrel data covered the whole study period.
European guidelines recommend secondary preventive drug therapy with dual antiplatelet therapy, statin, β-blocker and ACE inhibitor or ARB in patients with ACS.8 ,9 OAP treatment for 1 year in the absence of excess bleeding risk was a class IA recommendation in the 2011 European Society of Cardiology guideline,8 which was reflected in the rapid increase of OAP use (table 2). Treatment persistence curves (figure 2A) indicate that prasugrel and ticagrelor are accordingly withdrawn after 12 months. Premature discontinuation of OAP therapy has been defined as an independent risk factor for thrombotic events.25 For clopidogrel, in addition to 12 months, drops also occurred at 1, 3 and 6 months without observable improvement during the study period. Old age, dementia, high Charlson Comorbidity Score, atrial fibrillation and, particularly, warfarin treatment were indicators for not completing 1 year of OAP medication. In general, studying patients older than 85 years as a separate group could give additional information about OAP treatment patterns.
The quality of the Finnish nationwide hospital data is reported to be high,26 ,27 and in the case of the three OAPs, the exposure definition can be considered to be highly reliable. In pharmacoepidemiological studies using prescription data, the exposure is usually determined by the amount of purchased drugs in DDDs, but since the dosing per day is fixed for clopidogrel, prasugrel and ticagrelor, we were able to define OAP exposure by counting tablets. The treated and untreated periods were detected in detail, and then MPRs were calculated for each OAP-treated patient.
In our study, the mean MPR for the whole exposure time on OAP for each OAP-treated patient was excellent: 99%. No sex or age differences were found in MPRs. Regarding secondary prevention medication other than OAPs after discharge, statin was in the regimen of 84%, β-blocker in 81% and ACE inhibitors or ARB in 67%. The adherence to combination medication reportedly decreases by time after the discharge and by age.28 Good adherence to polytherapy is associated with lower mortality.29 The risk reduction associated with antiplatelet therapy was reported to decline, however, at the age of 70–75 years.20 The polypharmacy persistence is also lower in high-risk patients. Another recent study reported that one-third of the patients with myocardial infarction discontinued at least one secondary prevention drug by 6 months after the event, but older age explained this risk by only 1.07 times.30 In our cohort, the proportion of patients using all the three secondary prevention drugs (other than OAP) was higher in under 75-year-old patients than over 75, and in men than in women (42% vs 22% and 36% vs 27%, respectively; p<0.001 for both).
The present study has some limitations. One major limitation is the retrospective nature of observational registry data. Thus, diagnoses and procedural coding were made by treating physicians, which may have affected the included patient population and the accuracy of comorbidity and procedural data. Furthermore, national differences in risk factors, socioeconomic factors and treatment algorithms may limit the generalisability of the results.
In conclusion, only half of the 54 000 patients with ACS in our study cohort, mainly PCI-treated patients, received ADP receptor-inhibiting OAP treatment after hospital discharge. The OAP users, however, showed good compliance with immediate initiation and extremely high mean MPR of their medication during drug usage. In line with the guidelines, a clear drop occurred at 1 year in the persistence curves, and most of the OAP users also had statin and β-blocker medication in their regimen. Increased age, non-PCI-treated ACS event, dementia, atrial fibrillation and warfarin medication appear to have highest risk of being undertreated, in terms of no initiation and early discontinuation of OAP treatment. Healthcare professionals and patient educators should be particularly careful about when to deliver evidence-based OAP treatment after ACS for these subpopulations.
Acknowledgments
Ilona Iso-Mustajärvi is acknowledged for professional study coordination. We thank Shannon Kuismanen for revising the language of the manuscript.
References
Footnotes
Contributors TP has been involved in planning, organisation and execution of the study project. She designed and reviewed statistical analyses, and wrote the manuscript. TP was the principal investigator of the study. HK participated in the planning and execution of the study project. He planned and executed the statistical analyses, and wrote the manuscript. He was the main statistician in this study. AD and PH are representatives of the sponsor. They participated in study planning, statistical analyses review and manuscript writing phases of the study. AD also performed coordination work and PH was involved in designing the statistical work. VK, ER and JA are members of the steering group. They were involved in reviewing results and the manuscript. ER and JA also reviewed the study protocol.
Funding The study was fully sponsored by AstraZeneca Nordic-Baltic.
Competing interests TP and HK are employees of EPID Research, which is a contract research organisation. EPID Research performs commissioned pharmacoepidemiological studies, and thus its employees have been and currently are working in collaboration with several pharmaceutical companies. VK, ER and JA have received fees from pharmaceutical industry for consultancy regarding educational or advisory activities. AD and PH are employees of the sponsor, AstraZeneca Nordic-Baltic.
Ethics approval Ethical Review Board of the Hospital District of Helsinki and Uusimaa, Finland.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The study was conducted by following the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) Code of Conduct and registered into the EUPAS e-register (EUPAS6161). This ensures transparency of the study process including access to full-length study report via ENCePP web pages.