Article Text

Abstract
Objectives Infant respiratory distress syndrome (IRDS) is a known risk factor for intracerebral haemorrhage/intraventricular haemorrhage (ICH/IVH) and periventricular leucomalacia. These lesions are known to increase the risk of cerebral palsy (CP). Thus, we wanted to examine the long-term risk of CP following IRDS in moderately late and late preterm infants.
Design Population-based cohort study.
Setting All hospitals in Denmark.
Participants We used nationwide medical registries to identify a cohort of all moderately and late preterm infants (defined as birth during 32–36 full gestational weeks) born in Denmark in 1997–2007 with and without hospital diagnosed IRDS.
Main outcomes measures We followed study participants from birth until first diagnosis of CP, emigration, death or end of follow-up in 2014. We computed the cumulative incidence of CP before age 8 years and used Cox's regression analysis to compute HRs of IRDS, comparing children with IRDS to those without IRDS. HRs were adjusted for multiple covariates.
Results We identified 39 420 moderately late and late preterm infants, of whom 2255 (5.7%) had IRDS. The cumulative incidence of CP was 1.9% in infants with IRDS and 0.5% in the comparison cohort. The adjusted HR of CP was 2.0 (95% CI 1.4 to 2.9). The adjusted HR of CP was 12 (95% CI 4.5 to 34) in children with IRDS accompanied by a diagnosis of ICH/IVH. After restriction to children without diagnoses of perinatal breathing disorders other than IRDS, congenital heart disease and viral or bacterial infections occurring within 4 days of birth, the overall adjusted HR was 2.1 (95% CI 1.4 to 3.1).
Conclusions The risk of CP was increased in moderately late and late preterm infants with IRDS compared with infants without IRDS born during the same gestational weeks.
- EPIDEMIOLOGY
- respiratory distress syndrome
- cerebral palsy
- neurodevelopmental disorder
- cohort study
- PERINATOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- EPIDEMIOLOGY
- respiratory distress syndrome
- cerebral palsy
- neurodevelopmental disorder
- cohort study
- PERINATOLOGY
Strengths and limitations of this study
A strength of this study includes the nationwide cohort study design with virtually complete follow-up, minimising the risk of selection bias.
To our knowledge, this is the first study to specifically determine the association between infant respiratory distress syndrome and cerebral palsy using multivariate analysis, and as such, the validity of the estimates presented is unknown.
Even though this study is one of the largest examining a potential association between infant respiratory distress syndrome and cerebral palsy, it still does not clarify the specific causes leading to increased risk of cerebral palsy.
Introduction
Increasing preterm birth rates over the last few decades have kept the overall incidence of infant respiratory distress syndrome (IRDS) high.1–3 IRDS decreases with increasing gestational age and has a prevalence of about 30% after 32 weeks of gestation.4–6 The condition is caused by lack of surfactant in the lungs, which leads to atelectasis, decreased gas exchange and hypoxia. Potential complications of IRDS include intracerebral haemorrhage/intraventricular haemorrhage (ICH/IVH) and periventricular leucomalacia (PVL).7 ,8 Studies have reported increased risk of neurodevelopmental impairments, such as neurocognitive and school performance outcomes as well as attention-deficit hyperactivity disorder (ADHD) in preterm children with subsequent hypoxic conditions, including IRDS.9 ,10
Cerebral palsy (CP) is the most common cause of severe disabilities in early childhood.11 The core symptom of CP is disorder of movement and/or posture, but is often accompanied by other neurodevelopmental disorders or sensory problems, such as disturbances of sensation, cognition, communication, perception, behaviour and/or seizure disorders.12 The disorder has a multifactorial and poorly understood aetiology. The most important risk factor for CP is preterm birth, observed in about 28–35% of all children with CP.13 ,14 Major lesions that contribute to CP include ICH/IVH and PVL.7 ,15 ,16
Few data exist on the long-term prognosis following IRDS. A few case–control studies have reported indications of an association between IRDS and CP.17–19 However, these studies are limited by small sample sizes and lack of absolute risk estimates. In the present study, we therefore examined the association between IRDS and CP in a nationwide follow-up study of children born moderately and late preterm.
Methods
Setting and data linkage
We conducted this cohort study using population-based medical databases covering the entire country of Denmark. Linkage between databases was possible through the Civil Registration System (CRS), which has kept electronic records of birth date, date of emigration and date of death since 1968.20 At birth or on immigration, all Danish residents are assigned a unique Civil Personal Registration (CPR) number that is used in all public Danish registries. The Danish National Health Service provides free tax-supported healthcare to the country's 5.6 million citizens.
Study cohort
Our cohort was identified using the Danish Medical Birth Registry, which contains information on all births in Denmark since 1973. We identified all infants born alive in Denmark from 1 January 1997 to 31 December 2007 (∼710 000 infants)21 ,22 and then restricted our cohort to moderately late and late preterm infants (defined as birth between 32 and 36 full weeks). Adequate representation of children with and without IRDS is available during these gestational weeks.
Infant respiratory distress syndrome
We identified all children diagnosed with IRDS (exposed children) in the Danish National Patient Registry (DNPR). The DNPR contains data on all non-psychiatric hospital admissions in the country since 1977 and on outpatient clinic and emergency room visits since 1995.23 ,24 Data include dates of admission and discharge, surgical procedure(s) performed, and one primary diagnosis and up to 19 secondary diagnoses coded by the discharging physician according to the International Classification of Diseases, Eighth Edition (ICD-8) until the end of 1993 and the Tenth Edition (ICD-10) thereafter.
Cerebral palsy
Children diagnosed with CP were identified from the Danish National Cerebral Palsy Registry (DNCPR). Prerequisites for inclusion in this registry are a prenatal or perinatal aetiology (events occurring within 28 days of birth).
All children included in the registry had their diagnosis externally validated by a child neurologist at the age of 4–5 years, based on review of clinical findings recorded in the medical files. While the registry includes data on prenatally and perinatally acquired cases of CP since 1950, it became nationwide only in 1995. DNCPR is assumed to cover >85% of the children with CP in Denmark.25 Registry data include subtype and degree of CP,11 predefined ranges of developmental quotient (DQ: <50, 50–85, >85), motor handicap measured by the Gross Motor Function Classification System (GMFCS, 0–4) (though only complete until birth year 2003), accompanying neurological diseases and orthopaedic surgeries. Results of ultrasound and CT scans of the brain and evaluation of timing of brain damage are available.25 The DQ were mostly based on a clinical evaluation by a neuropaediatrician, because the results of the psychological assessments were rarely available in the medical files. The GMFCS is a tool used to measure gross motor skills in children with CP. The classification system ranges from level 1 (walking with no support) up to level 5 (immobile/impaired in all areas of motor function).26 We obtained the following study outcomes from the registry: overall diagnosis of CP, selected subtypes of CP (unilateral and bilateral spastic CP), motor handicap degree (GMFCS levels 1–2, 3 and 4–5) and DQ (<50, 50–85 and >85).
Covariates
We obtained information from the Danish Medical Birth Registry for the entire cohort on gestational age at birth, 5 min Apgar score, chorioamnionitis, intrauterine growth restriction, abruptio placenta, multiplicity, maternal age and self-reported maternal smoking during pregnancy.22 Of note, information on administration of antenatal corticosteroids was not available. In the early years, weeks of gestation was based on the first day of the last menstrual period. Later, prenatal ultrasound measurements were also included as a valid measure for the gestational age. However, in the Danish Medical Birth Registry, it is not possible to distinguish between the methods of measurement used to determine gestational age.21 We used data from the DNPR to ascertain the distribution of complications in children with and without IRDS, including bronchopulmonary dysplasia, ICH/IVH, necrotising enterocolitis and patent ductus arteriosus (see online supplementary appendix A). Congenital malformations are associated with increased risk of CP and also may be associated with IRDS. We therefore ascertained from the DNPR all diagnoses of congenital malformations detected during the first year of life.
Supplemental material
A subgroup of children may have had other conditions within 4 days of birth whose symptoms potentially overlapped with IRDS and may potentially lead to misdiagnosis of IRDS. These diseases include perinatal breathing disorders other than IRDS, congenital heart diseases, and viral and bacterial infections. We identified these conditions from the DNPR (see online supplementary appendix A).
Statistical analysis
We followed all children in the study cohort from date of birth until the date of the first diagnosis of CP, emigration, death or 31 December 2014, whichever came first. We computed the cumulative incidence of CP before 8 years of age with death as a competing risk.27 In a subanalysis, the commonest subtypes of CP were analysed as separate outcomes (unilateral and bilateral spastic CP), as well as motor handicap degree (GMFCS 1–2, 3 and 4–5) (only valid until birth year 2003) and developmental quotient (<50,50–85, and >85).
We used Cox proportional hazard regression to estimate unadjusted and adjusted HRs for CP among children with IRDS compared with children without IRDS. The analyses were adjusted for gestational age (32, 33, 34, 35 and 36 weeks of gestation), birth year (1997–1999, 2000–2002, 2003–2005 and 2006–2007), gender, multiplicity (singleton/twins), major malformations and maternal age (<35 and ≥35 years of age). The assumptions of proportional hazards were all verified graphically. We considered a low 5 min Apgar score as a causal intermediate step between IRDS and CP and, thus, did not include this covariate as a confounder in the adjusted analyses. However, we did include 5-min Apgar score in the regression model in a subanalysis. Chorioamnionitis, intrauterine growth restriction and abruptio placenta are important independent risk factors of CP. Moreover, these conditions are associated with IRDS, not independently, but through low gestational age. Though, they did not qualify as confounders in the association between IRDS and CP, we did include the three covariates as confounders in a subanalysis.
We stratified the analyses on gestational age (birth at 32, 33, 34 and 35–36 full weeks), birth year (1997–2002, 2003–2007), gender, multiplicity, 5-min Apgar score (0–6, 7–8, 9–10, missing), and maternal age (<35 and ≥35 years of age) and calculated 95% CIs. ICH/IVH is a known complication of IRDS and an important risk factor for CP. We, therefore, repeated the analyses for children with IRDS and a diagnosis of ICH/IVH within 30 days of birth compared with children with IRDS and no diagnosis of ICH/IVH. Of note, cranial ultrasound is not performed as a routine in moderately late and late preterm infants, so the proportion of infants with a diagnosis of ICH/IVH is based on detection in only infants selected for neuroimaging based on clinical presentation and risk factors.
Perinatal diseases may be misinterpreted as IRDS because of overlapping clinical symptoms or coexist with IRDS. Such perinatal disorders include perinatal breathing disorders other than IRDS, congenital heart diseases and viral and bacterial infections. Thus, in a sensitivity analysis, we restricted the IRDS cohort to newborns with no other perinatal disorders occurring within 4 days of birth.
All analyses were performed using the Stata 13.1 package (StataCorp LP, College Station, TX, USA). According to Danish legislation, registry-based studies do not need permission from an ethical board. The study was approved by the Danish Protection Agency (record number: 2014-41-3183) and did not require informed consent.
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study. No patients were asked to advise on interpretation or writing up of results. There are no plans to disseminate the results of the research to study participants or the relevant patient community.
Results
From the Danish Medical Birth Registry, we identified 39 420 children born moderately and late preterm between 1997 and 2007. Of these, 2255 (5.7%) were diagnosed with IRDS. Having another perinatal disorder occurring within 4 days of birth, including perinatal breathing disorders other than IRDS, congenital heart diseases, and viral and bacterial infection were more prevalent in the children with IRDS (30%) compared with children without IRDS (18%) (table 1).
Characteristics of 39 420 infants born during 32–36 weeks of gestation with and without infant respiratory distress syndrome (IRDS), between 1 January 1997 and 31 December 2007 in Denmark
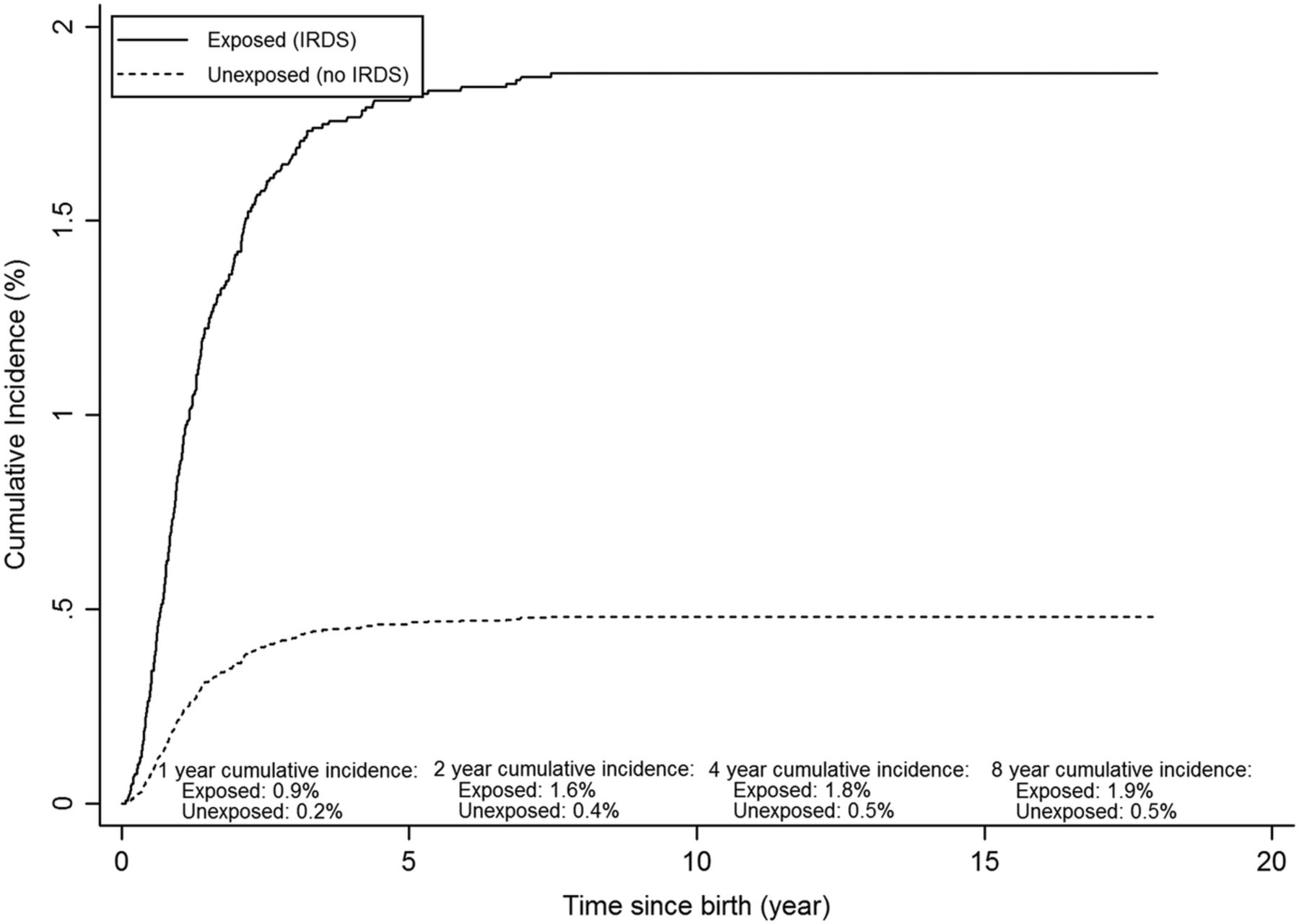
The cumulative incidence of CP before 8 years of age was 1.9 (95% CI 1.4 to 2.5) in children with IRDS and 0.5 (95% CI 0.4 to 0.6) in children without IRDS (figure 1). The overall crude HR for CP in children with IRDS compared with children without IRDS was 4.0 (95% CI 2.9 to 5.6). After adjusting for gestational age, birth year, gender, multiplicity, major malformations and maternal age, the HR was 2.0 (95% CI 1.4 to 2.9) (table 2).

{kind=link}
Cumulative incidence of cerebral palsy in 24 728 children with and without infant respiratory distress syndrome (IRDS) in Denmark during 1997–2003.
HRs of cerebral palsy (CP) by age 8 among children with and without infant respiratory distress syndrome (IRDS) born during 32–36 weeks of gestation between 1992 and 2007 in Denmark. (N=39 410)
When we stratified the analysis by gestational age, we found an increased risk of CP across all strata in children with IRDS compared with children without IRDS. As well, we found no substantial variation in the increased risk of CP in children with IRDS across categories of gender, year of birth, multiplicity, 5-min Apgar score and maternal age, although these estimates were less precise. The adjusted HR of CP was 12 (95% CI 4.5 to 34) in children with IRDS complicated by a discharge diagnosis of ICH/IVH.
Including 5-min Apgar score as a potential confounder in the regression model did not change our estimates substantially. The same was evident, when we included chorioamnionitis, intrauterine growth restriction and abruptio placenta as potential confounders in the regression analysis (overall HR of 2.0 (95% CI 1.4 to 2.9)). When restricting to children diagnosed with IRDS and no other relevant coexisting diagnoses occurring within 4 days of birth (ie, perinatal breathing disorders other than IRDS, congenital heart diseases, and viral and bacterial infections), the overall adjusted HR was 2.1 (95% CI 1.4 to 3.1).
The most common subtype of CP was unilateral and bilateral spastic CP (data not shown). For children diagnosed with IRDS, we found an HR of 1.5 (95% CI 0.8 to 2.9) for unilateral spastic CP and 2.2 (95% CI 1.4 to 3.4) for bilateral spastic CP. The HR was 1.9 (95% CI 1.1 to 3.4) for CP with a normal DQ (above 85), 1.7 (95% CI 0.9 to 3.1) for a DQ between 50 and 85, and 2.9 (95% CI 1.4 to 6.1) for a DQ below 50 (table 3).
HRs of cerebral palsy (CP) among children with and without infant respiratory distress syndrome (IRDS) born during 32–36 weeks of gestation between 1992 and 2007 in Denmark
In children with IRDS born during 1997–2003, the HR was 2.2 (95% CI 1.3 to 3.9) for a mild degree of motor handicap (GMFCS 1–2) and 2.5 (95% CI 1.3 to 4.7) for a severe degree of motor handicap (GMFCS 4–5) (table 3).
Discussion
We found an increased risk of CP associated with IRDS in children born moderately late and late preterm.
Other studies have shown increased risk of neurodevelopmental impairments, defined by psychomotor development and school readiness, in preterm children with IRDS.9 ,10 ,28 ,29 Studies have looked at possible causes or predictors of CP in different settings and found modest associations. In an Australian case–control study, Blair et al reported an OR of CP of 2.3 (95% CI 1.3 to 4.3); and in another case–control study from Western Australia, Dite et al found an OR of 9.4 (95% CI 1.8 to 48) in children diagnosed with IRDS. However, even though they reported increased risk estimates of CP in children with IRDS, the estimates were based on univariate analyses in relatively small study populations. Thus, potential confounders were not taken into consideration, and no absolute measures were available.17–19 In a cohort study, Hirvonen et al found a negative association between IRDS and CP in late preterm infants. However, apparently the multivariate model included intermediate steps between IRDS and CP in terms of mechanical ventilator treatment and intracranial haemorrhage. Furthermore, the analysis was not based on time-to-event methods, but based on logistic regression.30 This may have explained the differences between their results and ours.
Through data linkage performed by the Danish CRS, this population-based study had virtually complete follow-up for death, emigration and hospital admissions, minimising the risk of selection bias. As lack of surfactant cannot be measured directly, the diagnosis of IRDS is based on the clinical appearance of the infant; thus, it is not possible to make a clear and consistent diagnostic test. We previously reported a positive predictive value of 89% (95% CI 75% to 96%) for children with IRDS born between 32 and 36 weeks of gestation in the DNPR.31 In this study, IRDS was based exclusively on clinical symptoms, as X-rays were only used infrequently early in the study period. Additionally, in a sensitivity analysis, we redefined our exposure of children with IRDS to only those having IRDS with no other perinatal disorders occurring within 4 days of birth. Our estimates were virtually unchanged in this analysis. As the CP Registry is a clinical database based on specific inclusion criteria including thorough medical record review of all children with CP in Denmark, we expect the positive predictive value of the CP diagnosis to be close to 100%. A previous validation study of the DNCPR through the DNPR reported its completeness to be 85%.25 As any misclassification is not likely associated with IRDS, such non-differential bias would eventually lead to an underestimation of the association between IRDS and CP.
One of the strongest risk factors for development of CP is known to be low gestational age,32 ,33 which is also the strongest risk factor for IRDS. For this reason, we stratified our analyses on gestational age to ensure that any increased risk of CP in children with IRDS was not masked by this association. After taking this precaution, we still found an increased risk of CP among children born during gestational weeks 32–34. Only a few children diagnosed with CP were born during 35 and 36 weeks of gestation, which made calculations of the HR imprecise.
To study rare disease like CP large study populations are required, especially when the study sample is restricted to children born at 32–36 gestational weeks. For this reason, we were only able to present overall estimates in our analyses of selected subtypes of CP, degree of motor handicap and DQ. These estimates were all increased throughout all levels of CP severity. Of note, the prespecified DQ score category, including scores of 50–85, encompassed children with normal intelligence as well as delayed children, indicating a diverse group. Thus, not too much emphasis should be given to this group.
Even though this study is among the largest studies examining a potential association between IRDS and CP by using data from nationwide databases on preterm infants, it still does not clarify the specific causes of the increased risk of CP. We found a 12-fold increase of CP in children with IRDS and a diagnosis of ICH/IVH compared with our control population. This may suggest an important role of ICH/IVH in the pathogenesis, though this is only a speculation.15 ,34 ,35 In moderately late and late preterm infants, neuroimaging is not routinely performed, indicating that some of these children may have an undiagnosed ICH/IVH. Based on this, the proportion of children with ICH/IVH may have been underestimated in the exposed group as well as in the comparison cohort, making the HR imprecise.
Antenatal corticosteroids decrease the risk of IRDS, as well as ICH/IVH. However, recent studies have reported adverse neurodevelopment outcomes in children receiving antenatal steroids.36 We did not have information of treatment with antenatal corticosteroids, which is a limitation of our study.
IRDS potentially could be a surrogate for another unknown medical condition. However, recognition of an early predictor of increased future CP risk could still be helpful when planning follow-up and/or intervention strategies in children born preterm.
Conclusion
We found that the risk of CP was twice as high in moderately late and late preterm infants with IRDS compared with infants without IRDS born during the same gestational weeks.
References
Footnotes
Contributors SKT conceptualised and designed the study, acquired the data, carried out the analyses, drafted the initial manuscript, reviewed and revised the manuscript and approved the final manuscript as submitted. MO, JRO and HTS conceptualised and designed the study, supervised the data interpretation, critically reviewed and revised the manuscript for important intellectual content and approved the final manuscript as submitted. MO helped to acquire the data and extract the raw data, critically supervised/reviewed the data analyses and reviewed the data interpretation, revised the manuscript and approved the final manuscript as submitted.
Funding This study was supported by grants from the Clinical Epidemiological Research Foundation (‘Klinisk Epidemiologisk Forskningsfond’), Denmark (HTS) and the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck and the Novo Nordisk Foundations (HTS). The funding agencies had no role in the design of the study; the collection, analysis and interpretation of the data; the writing of the article; or the decision to submit the article for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author statement All authors, external and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Transparency declaration SKT affirms that the study hypothesis arose before inspection of the data and that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Data sharing statement No additional data are available.