Article Text

Abstract
Objective To determine what, how, for whom, why, and in what circumstances educational interventions improve the delivery of nutrition care by doctors and other healthcare professionals work.
Design Realist synthesis following a published protocol and reported following Realist and Meta-narrative Evidence Synthesis: Evolving Standards (RAMESES) guidelines. A multidisciplinary team searched MEDLINE, CINAHL, ERIC, EMBASE, PsyINFO, Sociological Abstracts, Web of Science, Google Scholar and Science Direct for published and unpublished (grey) literature. The team identified studies with varied designs; appraised their ability to answer the review question; identified relationships between contexts, mechanisms and outcomes (CMOs); and entered them into a spreadsheet configured for the purpose. The final synthesis identified commonalities across CMO configurations.
Results Over half of the 46 studies from which we extracted data originated from the USA. Interventions that improved the delivery of nutrition care improved skills and attitudes rather than just knowledge; provided opportunities for superiors to model nutrition care; removed barriers to nutrition care in health systems; provided participants with local, practically relevant tools and messages; and incorporated non-traditional, innovative teaching strategies. Operating in contexts where student and qualified healthcare professionals provided nutrition care in developed and developing countries, these interventions yielded health outcomes by triggering a range of mechanisms, which included feeling competent, feeling confident and comfortable, having greater self-efficacy, being less inhibited by barriers in healthcare systems and feeling that nutrition care was accepted and recognised.
Conclusions These findings show how important it is to move education for nutrition care beyond the simple acquisition of knowledge. They show how educational interventions embedded within systems of healthcare can improve patients’ health by helping health students and professionals to appreciate the importance of delivering nutrition care and feel competent to deliver it.
- EDUCATION & TRAINING (see Medical Education & Training)
- Realist review; nutrition; educational interventions; doctors; healthcare professionals
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- EDUCATION & TRAINING (see Medical Education & Training)
- Realist review; nutrition; educational interventions; doctors; healthcare professionals
Strengths and limitations of this study
Application of the principles of realist synthesis to nutrition and education research is novel.
The characteristics and conditions of educational interventions that can improve the delivery of nutrition care, identified by this review, are important to the work of policymakers, researchers, health professions educators and course developers.
Few reports of failed educational interventions were found, indicating a risk of positive publication bias.
Until our conceptual model is tested and refined in the real world, we consider it to be an indefinite candidate theory, presenting elements worth considering by those concerned with the design, implementation and evaluation of educational interventions to improve the delivery of nutrition care by doctors and other healthcare professionals.
We cannot assume that the research evidence we identified represents ‘real-world’ practices, and therefore our claims for the transferability of this research must be guarded.
Introduction
Nutrition is an important component of healthcare. It plays a critical role in the prevention and treatment of most cardiovascular and cerebrovascular diseases, which are leading causes of morbidity and mortality throughout the world.1–3 Nutrition is even more important in sub-Saharan Africa because malnutrition is a major cause of morbidity and mortality, particularly among children.4
Several landmark reports5 ,6 have identified the delivery of nutrition care as one of the core responsibilities of doctors. Research has also shown that nutrition counselling delivered by them has positive influence on patients’ clinical outcomes. They and other healthcare professionals whose primary role is not nutrition care, however, often miss opportunities to advise patients on diet and health.7 ,8 Health workers in primary care settings are particularly important providers of nutrition care because they can motivate even healthy individuals to adopt healthier lifestyles.9 The care expected from primary care health workers includes nutrition assessment, education and counselling interventions, monitoring and evaluation. Lack of knowledge,10 skills and confidence,11 ,12 as well as negative attitudes towards delivery of nutrition care and low outcome expectancy,13 are barriers to healthcare professionals providing nutrition care. In addition to these individual-related factors, several system-related factors such as lack of time, office space, payment, materials and education14 also prevent the delivery of nutrition care by these healthcare professionals.
Many educational interventions have been designed and implemented to improve nutrition care, but their effects have been inconsistent and often weak.15–17 There remains a need, therefore, for interventions that can change healthcare professionals’ behaviour in practice.15–17 It is imperative to identify contextual factors, which mediate or inhibit their competence and delivery of nutrition care.18 ,19 In order to meet those needs, researchers have to identify components of effective educational interventions and processes.
To date, only one secondary research investigation has synthesised conclusions from existing evidence about nutrition care.20 The authors of that review concluded that in-service nutrition training improved healthcare professionals’ knowledge, nutrition-related counselling skills and malnutrition management skills. The main limitation was that this was a traditional systematic review, which only considered in-service nutrition training programmes. Its authors found that the evidence base was very heterogeneous; studies had widely varying study designs with heterogeneous outcome measures; and there were wide differences in the competence, experience and backgrounds of participating healthcare professionals. As the authors acknowledged, systematic review methodology limited their ability to recognise and account for the complexity of interactions within such interventions.
We reasoned that we could move the field forward by conceptualising nutrition education interventions as complex ones within a realist research approach. As noted in our published review protocol,21 we recognised that educational interventions involve multiple actors operating at different levels with a range of artefacts in varied material environments.22 We assumed that these components operate in non-linear ways to yield context-dependent outcomes. Realist synthesis explores ‘what is it about this intervention that works, for whom and in what circumstances?’ and is therefore an appropriate way to study complex interventions.23 It is an iterative, theory-driven approach, which aims to unpack the theories that inform decisions and actions adopted in the design and implementation of interventions.24 Realist synthesis begins with the development of an initial programme (or candidate) theory about how interventions work, the contexts in which they do and do not work, and the differentiated patterns of outcomes that they generate.25 As the review progresses, researchers test the initial programme theory and refine it as more evidence becomes available.26
Thus, the aim of this realist review was to determine what, how, for whom, why and in what circumstances educational interventions improve the delivery of nutrition care by doctors and other healthcare professionals work.
Methods
VM is a nutritionist working in sub-Saharan Africa, which provided a context for the research. Other members of the team included scholars of medical education, evidence synthesis, social science, nutrition and an experienced clinician.
Alteration from protocol
The review question above is broader than in the published protocol21 because the search showed important findings from research in health professions other than medicine, which the team felt could make a valuable contribution.
Search methods
Search terms pertaining to nutrition, care, healthcare professionals, training etc were scoped on two electronic databases. Resulting articles were reviewed, and refinement of search terms was not considered necessary. Further explanation and a full list of the search terms can be found in our published protocol.21 A search strategy was created for Ovid MEDLINE (available in online supplementary appendix 1) and adapted for the rest of the databases. These databases were CINAHL, ERIC, EMBASE, PsycINFO, Sociological Abstracts, Web of Science, Science Direct and Google Scholar, the latter of which was used to search for grey literature. Email alerts were set for journals and RSS feeds for databases to ensure that we identified new papers as soon as they became available.
supplementary appendix
Inclusion criteria
Study participants: Medical students, students of other health professions and practising healthcare professionals (eg, nurses, physician assistant).
Focus of intervention: Developing participants’ competencies in any aspect of nutrition practice behaviour.
Study design: All.
Context of intervention: Medical schools, residency and fellowship programmes, and interventions at community and hospital settings.
Publication language: English.
Publication date: January 1994 to December 2014 inclusive. This date range was chosen because preliminary searches indicated that educational interventions to improve nutrition care competencies and delivery among doctors and other healthcare professionals gained prominence within published literature around 1994.
Exclusion criteria
We sought to understand generalists’ delivery of nutrition education, and therefore we excluded research that only considered the education of dietitians and/or nutritionists since nutrition is their main responsibility. While we excluded conference proceedings, opinion pieces, case studies and abstracts, we used them to develop the initial candidate theories reported in our protocol.21 We also excluded systematic reviews, although they informed the design of our data extraction form and provided an insight into context, mechanism outcome (CMO) configurations and additional references. Papers were also excluded if they lacked evaluation or outcome data and not being about improvement in nutrition care competencies.
Study selection
Figure 1 shows the flow chart of the search and selection processes. The final search yielded 4500 hits. VM and TD initially screened the titles of 100 hits independently and compared their findings. There was almost complete agreement, and VM continued with the screening. After eliminating duplicates, 357 studies were selected. Having obtained their abstracts, VM, TD and MGC determined independently whether each study was concerned with improving nutrition care competencies and delivery of nutrition care. At a face-to-face discussion, we compared our choices, for which the κ statistic of agreement was 0.9. This yielded 74 studies, 6 of which were excluded because they were conference abstracts. Seven studies could not be obtained despite repeated attempts. VM read the reference lists of the remaining 61 studies, and all identified systematic reviews, identifying 11 more studies.
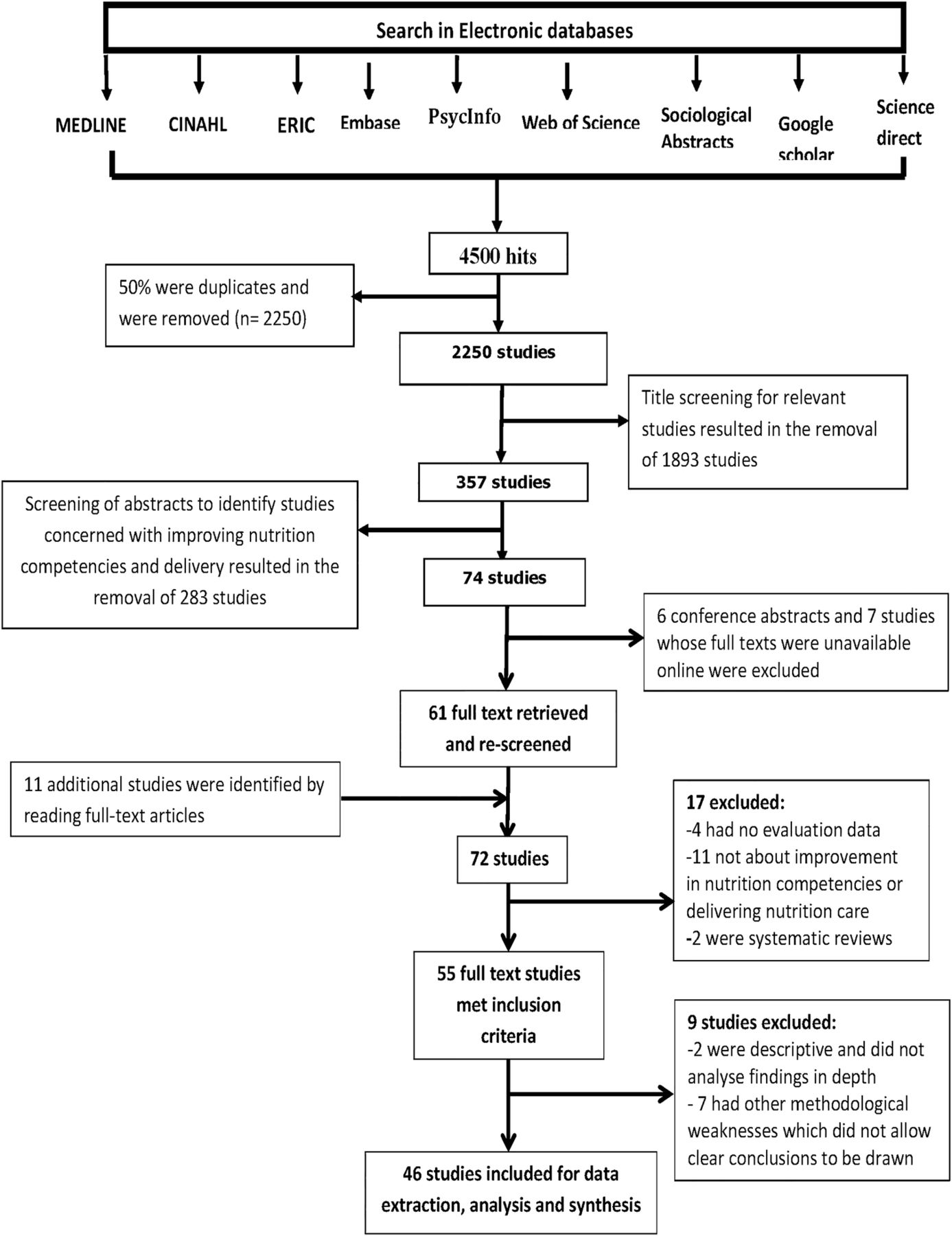
Search and selection process.
Quality assessment
It is regarded as acceptable in realist synthesis to include part(s) or whole studies for analysis and synthesis, provided that the methods employed for collecting such data are robust.27 As recommended by Pawson,25 the appraisal of primary studies was informed by their relevance as well as their rigour.25 Our judgements of a study's relevance were informed by the extent to which the whole study or parts of it were relevant to our published initial programme theory.21 Our assessment of rigour was informed by the trustworthiness of studies’ design, sample size and data collection tools in relation to the outcomes reported. The Mixed Methods Appraisal Tool28 helped us assess rigour.28 Based on the exclusion and inclusion criteria, VM selected 55 of the 72 studies for quality assessment. Quality assessment was conducted by AS, TD, FS and MGC. This process resulted in the exclusion of nine studies from which clear conclusions could not be drawn because of methodological weaknesses. The remaining 46 studies were included into our data analysis. We kept notes of our reasons for including or excluding each study and resolved doubts about our judgements of study quality by discussing between ourselves. The processes of quality assessment and data extraction proceeded concurrently.
Data extraction, analysis and synthesis
For the purpose of data extraction, we followed guidance from previous related systematic reviews20 ,22 ,29–31 and iteratively refined our procedures in accordance with the focus of the review. VM initially extracted data from a sample of 10 studies, discussed the findings with the other members of the team and used those discussions to guide further data extraction. Data extracted included the following:
Study design, sample size and outcome data
Educational levels of study participants (students vs practising health workers)
How course material had been developed
Topics covered
Methods of teaching and learning
Methods of evaluating outcomes including data collection tools
Intervention type (eg, workshops, curriculum designs)
Durations of intervention
Contexts of intervention (eg, practising healthcare professionals, students)
Mechanisms generated
Learning outcomes
Impacts (if any) of intervention on clinical outcomes
Any theories or mechanisms postulated by author(s) explaining the effects of interventions
We read all 46 included studies twice, transferring relevant data into our data extraction form. We identified the CMOs and interactions between them for each study as well as the theory informing each intervention. To do that, we assumed that the design of each study was informed by a theory, which the authors stated explicitly or implicitly. Identifying those theories helped us understand how interventions worked to generate outcomes. We discussed and reflected on all the data we had identified for each study, sometimes using extracts of publication narratives to foster reflection.
The next stage was to identify themes that were common to different studies. Using an interpretative and narrative approach, we discussed and synthesised initial conclusions, which we used to refute or refine the candidate theories in our published protocol.21 We chose this process of synthesis in preference to a meta-analysis, which would not have been possible given the diversity in study populations, designs, interventions and outcomes.32
Results
General characteristics of the studies
Table 1 provides a summary of the 46 studies. Twenty-seven (59%) came from the USA, 7 (19%) from Europe, 4 each from South America (all from Brazil) and Asia, 2 from Canada and 1 each from Africa (ie, South Africa) and Australia. In total, 4816 participants participated in them (median=76 participants; IQR: 47, 178). Interventions that had healthcare professionals as participants had somewhat larger numbers (median=98; IQR: 46, 163) than those having students as participants (median=54 participants; IQR: 32, 152).
Summary of findings of studies reviewed (n=46)
The studies had varied study designs (shown in table 2) with a preponderance (n=39, 85%) of quasi-experimental designs. Twenty-one studies had follow-up evaluations after the pre-test and post-test evaluations. The time period between post-test and follow-up evaluations ranged between 2 weeks and 12 months.
Study designs and data collection methods
Most studies (n=32, 70%) evaluated outcomes using surveys of knowledge, attitudes, self-reported practice behaviours, self-efficacy, confidence and feedback. A large proportion of these surveys were developed by the authors, who did not usually report the psychometric properties of their instruments. All the interventions that set out to improve knowledge used multiple-choice questions (ranging between 1 and 78 questions). Changes in attitude before and after interventions were assessed using the Likert scales, anchored with statements describing attitudes.
Most questionnaires measuring behaviour changes used self-reported changes in nutrition practice behaviour. A few studies observed clinical behaviour to measure changes in nutrition practice. For example, one study in the Netherlands42 used incognito standardised patients to assess the impact of an intervention on the nutrition practice behaviour of general practitioner (GP) residents. Another study in Brazil54 measured nutrition indices (ie, wasting, stunting and underweight) of children to determine the impact of an educational intervention that aimed to improve the provision of nutrition counselling to mothers and/or caregivers by doctors.
Intervention focus, types, teaching and learning formats, duration of interventions and expected learning outcomes
Only 11 studies (24%) explicitly stated the theoretical underpinning of their interventions. These included experiential, social and cognitive learning theories as well as cognitive theory of multimedia learning. The purpose of most interventions was to improve participants’ competencies (ie, knowledge, skills and attitudes) in a variety of nutrition topics (shown in table 1). Studies originating from developing countries tended to cover topics related to infant and young child feeding practices, whereas those from developed countries covered topics related to hospital malnutrition and nutritional management of chronic diseases. Most studies in which students participated aimed to increase curriculum contact hours and nutrition content. Studies involving practitioners were usually continuous medical education (CME) programmes aiming to improve knowledge, attitudes, skills and practice behaviour in specific topics such as breastfeeding practices and dietary counselling. Teaching and learning formats included lectures, problem-based learning tutorials, nutrition slogans, demonstrations, role plays, group discussions, games and video presentations. All interventions used more than one teaching and learning format except six, which were either lecture based or computer based only.38 ,42 ,46 ,55 ,64 ,69 Almost all of the interventions used innovative teaching and learning methods. Interventions involving students were usually obligatory and lasted from 2 weeks to 4 years. Those involving professionals were generally shorter. The shortest intervention was a 1-hour intensive session for GPs and other healthcare professionals on the benefits of giving folic acid to women of child bearing age;52 the longest were two 4-year integrated nutrition curricula for medical students.35 ,51 Inconsistent reporting of the length of interventions (including use of terms like credit hours) made it difficult to determine their average lengths.
Context–mechanisms–outcomes configurations
Table 3 lists the CMOs identified from the included studies. We describe here how those interacted to yield CMO configurations.
Context, mechanism and outcome configurations
Emphasising skills development instead of knowledge outcomes (‘Let me be skilful’)
Researchers were often triggered to design interventions by professionals’ lack of knowledge about nutrition. This was particularly true of undergraduate education,36 ,39 ,59 ,64 ,66 ,67 where all but one52 of the interventions primarily targeting knowledge took place. Yet interventions that only aimed to improve knowledge were less likely to change practice behaviour. In four studies, for example, significant gains in knowledge did not predict practice scores,37 improve students’ assessment of the nutrition status of overweight patients,34 influence behaviour change intentions38 or affect dietary counselling for mothers/caregivers of children aged 12–24 months.49 Furthermore, there were interventions, which did not significantly increase knowledge yet changed behaviour. For example, a significant improvement in diet counselling during audiotaped physician–patient interactions43 ,50 and increased self-reported counselling behaviour and confidence50 took place without any significant increase in knowledge. In one study, Ockene et al43 noted that ‘a large proportion (1.5 hour) of the entire 3 hour CME training program was devoted to the learning of counselling and dietary assessment skills’. These findings show that it is important to train skills and create learning environments that encourage the acquisition of skills in order to change healthcare professionals’ nutrition care behaviour.78 ,79
Superiors role modelling the delivery of nutrition care (‘I look up to you’)
A candidate theory in our published protocol,21 that healthcare professionals would be more likely to deliver nutrition care if they saw their superiors model the same behaviour, was apparent in the evidence. Seeing superiors model nutrition care led research participants to feel more confident, accepted and credible. They anticipated their actions being valued, which led them towards changing their nutrition practice. Virtual physician mentors,39 simulation of GP consultations using video clips,42 physicians describing how they addressed nutrition in practice68 and role modelling by physicians in classes68 were among the interventions that provided positive role modelling.
Meeting the needs of potential participants of an intervention (‘Ask me what I want’)
Most interventions were modelled on the theory that education will be most successful when it is designed to meet participants’ needs.33 ,34 ,37 ,48 ,50 ,52 ,59 ,62 ,63 ,67–69 Assessment of needs identified gaps in learners’ knowledge or practice behaviour,62 and how they learnt best. It informed the content, format and design of curricula. It helped select teaching and learning methods to which participants were receptive, which they found interesting and satisfying, and which led them to value their education.
Addressing structural and systemic factors (‘Is my consulting room enabling?’)
As well as education, interventions that improved working environments influenced participants’ behaviour and helped maintain changes that had been achieved.57 Eight studies helped participants address lack of support33 ,47 ,48 ,69 and systematic barriers.14 ,50 ,54 ,57 They restructured office environments to make them more conducive to providing nutrition care.14 Pelto et al,54 for example, stated that ‘structural conditions in the public health system in Pelotas provided an environment in which physicians could utilize their knowledge’ (p. 360). Other researchers provided nutritional messages that busy primary care providers could deliver to patients.33 Presentations on change management and leadership48 and provision of guidelines on office organisation14 helped improve nutrition care. Collaboration between education and care delivery leaders helped remove structural and systemic barriers.30 These created working environments that were conducive to the delivery of nutrition care.
Incorporating technology-based education (‘My computer is a learning tool’)
Seven studies used technology to resolve challenges relating to healthcare professionals having insufficient time to attend continuing education programmes, programmes having inadequate nutrition content and faculty being unavailable to teach.39 ,42 ,46 ,55 ,64 ,68 ,74 Computer-based and internet-based interventions allowed easy updating of content,42 permitted self-directed and independent study of nutrition information,42 ,46 presented content consistently,68 were accessible,74 promoted interactivity74 and were convenient for participants because they were self-administered42 ,68 and self-paced.74 These interventions led to significant gains of knowledge,39 ,46 ,55 ,64 positive attitudes,42 ,46 increase in self-assessed nutrition counselling skills42 ,55 and real-time practice behaviour.42 The convenience, interest and independent nature of this type of education contributed to those outcomes.
Providing participants with local, practically relevant tools and messages (‘Give me tools’)
Some researchers theorised that making local, practically relevant tools and messages available in practice contexts would change the behaviour of trainee healthcare professionals. The tools they provided included memorable slogans,33 simple ‘key take home messages’,33 ,37 ,40 ,63 personalised nutrition messages33 and locally relevant examples.54 Researchers simplified nutrition messages,33 provided resource materials and tools to resolve problems in counselling and assessing patients,54 ,63 and adapted advice for local conditions.54 Those interventions helped professionals engage in specific rather than generic discussions with patients and provided advice and recommendations that patients found relevant.54 The authors of a randomised controlled trial (RCT), which improved physicians’ counselling of mothers with malnourished children aged 12–24 months in Brazil,54 attributed children's improved nutritional status to this provision of locally appropriate messages and tools.
Using non-traditional teaching and learning strategies (‘The right strategy for the right job’)
Another theory, which guided interventions, was that non-traditional teaching and learning strategies would change professionals’ behaviour. For instance, Hillenbrand and Larsen41 hypothesised that providing a series of interactive educational interventions to paediatric residents would increase their knowledge about breastfeeding and lactation problems and increase their confidence to counsel breastfeeding women. Interventions, which sometimes complemented lectures, included discussions, simulated patient cases, group work, role plays, hands-on demonstrations, group practice, panel discussions and case-based learning. Other interventions included problem-based learning tutorials, computer-based or web-based cases, student-led debates, self-assessment exercises and clinical case presentations.58 ,62 ,68 These interventions provided practical experience and promoted active learning. They emphasised the development of skills rather than just knowledge. They engaged participants’ interest and helped them assume responsibility for their own learning. These interventions caused significant changes in participants’ knowledge, personal health habits, confidence to provide exercise and dietary counselling, ability to counsel obese patients and ability to manage malnutrition. Carson et al68 attributed the enhanced nutrition counselling skills of students in a 4-week ambulatory care rotation to their innovative combination of teaching strategies.
Improving self-efficacy (‘I feel that I can do it, so I will do it’)
Self-efficacy is a basic tenet of Bandura's social learning theory.80 This term describes individuals’ confidence in their ability to perform a task or achieve an outcome. It is a key influence on behaviour.80 Eight studies explicitly set out to improve participants’ self-efficacy by increasing their confidence. They adopted strategies like role modelling by practising physicians,68 role playing using either simulated or real patients,41 ,43 ,47 ,58 providing demonstrations and hands-on practice sessions33 ,41 ,43 ,45 ,47 ,61 ,68 and viewing then discussing videos and web-based cases.43 ,68 Four each of these interventions were conducted among future healthcare professionals and practising healthcare professionals. They were effective in both settings.
Improving the personal health habits of the healthcare professional (‘Do as I do’)
Four interventions, which stimulated practising45 ,60 and health professions students58 ,61 to take better care of their own health, had positive outcomes. These included regular consumption of fruits and vegetables, personal awareness of calorie consumption, engagement in regular physical activity and development of culinary skills. In both settings, these led to better self-reported healthy lifestyles and self-reported ability to undertake dietary assessment,61 counselling confidence,45 ,58 ,61 self-assessed knowledge60 and even treating a higher proportion of diabetic patients with diet alone.60 Healthcare professionals, who considered themselves role models for patients, felt more confident to advise patients to do as they had done.45 ,58 ,61
Initial and revised programme theory
Our published protocol21 presented candidate theories and a theoretical model, which we briefly repeat here. Drawing on social cognitive theory, we postulated the following:
Healthcare professionals’ ability to deliver nutrition care is influenced by their competence, which is the outcome of a learning process, which is influenced by factors within academic environments. Those factors include the quantity and quality of nutrition content in curricula, the teaching and learning methods employed, and the extent to which learning is reinforced.
Professionals are more likely to care for patients’ nutrition if they have high self-efficacy for nutrition care and vice versa.
Professionals’ delivery of nutrition care is a behaviour demonstrated in the social context of workplaces, which is influenced by observing and modelling the behaviours, attitudes and emotional reactions of others (eg, superiors).81 It is also influenced by the structural determinants of behaviours such as the workplace settings themselves (eg, hospital/community, emergency/paediatric/general ward), job descriptions/role, time and availability of other staff to undertake particular roles.
The review process described above examined those theories, which led us to revise, add components to and broaden our theoretical model (shown in figure 2). ‘Outcomes’, in realist terminology, can be short, medium and long terms.82 We have added a hierarchy of outcomes to our theoretical model.

{kind=link}
{kind=link}
Revised theoretical model or programme theory.
The items in the model are inter-related as opposed to operating in isolation from one another. They do not operate in a linear fashion. Several context–mechanism–outcome configurations could be generated from the data. For instance, assessments of needs identify knowledge, skills and attitude gaps and other educational needs of potential participants. The outcome of the needs assessments informs the design of the educational intervention as well as its characteristics. It informs what kind of characteristics or strategies the intervention should adopt in order to realise the desired outcome. These strategies could include improving the personal health habits of healthcare professionals, adopting technology-based education, improving skills development, adopting innovative teaching and learning strategies, role modelling and others. These generate mechanisms (not indicated in the diagram) such as interest, receptivity and acceptance, which generate short-term outcomes such as improved knowledge, attitude, skills, self-efficacy, values and personal habits. The immediate and short-term outcomes may act as mechanisms to bring about change in nutrition practice behaviour (medium-term outcome). Doctors and other healthcare professionals may change their nutrition practice behaviour as a result of having adequate knowledge, skills, attitudes, confidence and self-efficacy. A change in nutrition practice behaviour will mean increased delivery of nutrition care to patients, which may result in the long-term goal of improved clinical outcomes (long-term outcomes) of patients. However, these outcomes can best be enhanced and maintained if there is an enabling healthcare setting (context). This could be realised by enhancing certain conditions/contexts such as restructuring the healthcare system, removing structural and systemic barriers, adopting favourable policies for nutrition care, providing appropriate tools to deliver nutrition care, investing more in preventive care and providing an office that makes it easier to provide nutrition care. Providing an enabling healthcare setting was central to all of the CMO configurations identified.
We present in table 4 a summary of the characteristics of interventions in accordance with what works, for whom and under what conditions.
Overview of what works, for whom, under what circumstances and to achieve what
Measurement issues
The ultimate aim of health education is to improve health outcomes. Few studies have, however, even tried to show improvements in patients’ health because it is very difficult to do. Authors acknowledged that this limited the conclusions they could draw from their evidence,62 which meant that they could often only speculate on how their interventions might affect patients’ health. The impact of educational interventions is often ranked according to its position in Miller's pyramid of assessment.83 Some studies achieved the highest level—the performance level—which is most likely to impact patient outcomes. They did so by directly observing the delivery of nutrition care in clinical settings,14 ,41 ,44 ,49 ,54 recording videos of doctors counselling patients,14 auditing charts40 ,65 ,68 and using incognito simulated patients.42 Most studies were at lower levels of the pyramid. For example, they assessed participants’ reported changes in practice behaviours by means of self-administered surveys. As observed by the authors of one such study,58 reliance on students’ self-reported confidence in counselling rather than an objective measure of counselling skills (such as an objective-structured clinical examination) limits the generalisability of the findings. Schlair et al61 acknowledged the potential for social desirability bias in self-reports. While self-report would be invalid evidence in a systematic review or meta-analysis, it is safer to use it in realist synthesis, which aims to produce progressively more refined theories of change rather than incontrovertible evidence.
For future studies, Scolapio et al62 suggested that ‘harder’ data could be obtained using patient surveys and chart reviews, or having participants give specific examples of improved patient outcome that were directly linked to competences they had acquired from educational interventions. Our review shows the need for future studies to explore innovative ways of collecting this information.62
Discussion
There is increasing pressure for medical education to be socially accountable.84–86 This research may be seen as socially responsive because it arose out of a pressing health need in sub-Saharan Africa: improvement of the competencies of doctors and other healthcare professionals in order to deliver effective nutrition care. Our study provided practical guidance to educators trying to meet this need in Africa and elsewhere by showing the importance of moving education for nutrition care beyond the simple acquisition of knowledge.
The CMO configurations identified in this realist review are preliminary and non-exhaustive and should be considered as a set of generic hypotheses derived from the best available evidence. Nonetheless, they provide information to policymakers about what may improve the nutrition practice behaviour of healthcare professionals, how, under what conditions and in what settings. Our review has identified a set of conditions that facilitate the success of interventions in varied contexts.
A key finding of this review is that improving the skills, self-efficacy and attitudes of learners by adopting appropriate teaching and learning strategies is critical to the success of nutrition education interventions. Improving learners’ skills and attitudes provides them with confidence and a sense of enactive mastery of the specific tasks they have to perform. Role modelling of the delivery of nutrition care by superiors, providing appropriate physical space in which to deliver nutrition care and adopting favourable policies are important because they increase professionals’ sense of being accepted, credibility, relatedness and assurance.
Our analysis shows that planners of educational interventions would be well advised to assess potential participants’ needs and interests. Computer-based education presents new opportunities for course designers and planners. Already considered as a potentially efficient form of teaching and learning in the health professions,46 ,87–89 this presents novel ways of incorporating nutrition content into healthcare professional curricula. Given that healthcare professionals say they have too little time to attend training programmes and provide nutrition care, the convenience of computer-based and internet-based education has potential to overcome barriers to learning.
The main strengths of our review were its integrative nature and our use of realist synthesis methodology, which allowed for practical theories to be generated for future testing and implementation. However, the review had limitations. One is that we did not consult individual experts in the field when we developed our initial model. Had we done that, we might have included more candidate theories. We also acknowledge the interpretive and subjective nature of qualitative research and the likelihood that a different team of researchers might have arrived at different candidate programme theories. We acknowledge that the model shown in figure 2 is but one of several possible interpretations, as is typical of the models that emerge from realist synthesis. We acknowledge limitations in the evidence base. The synthesis that results from any review is only as good as the primary studies it is able to include. Many of the primary studies provided limited, superficial descriptions of their educational interventions. This made it difficult for us to test all components of our candidate theories and to provide rich descriptions of some of the mechanisms that were identified. As has been found by other reviewers in medical education,22 ,29 ,30 this review was limited by a lack of descriptions of the contexts of the intervention, implementation processes and mechanisms.
Other limitations included the unavailability of the full text of seven studies.90–96 While it is a limitation, realist synthesis is less dependent on the inclusion of complete sets of studies than, for example, traditional systematic reviews.82 So, it may limit the scope of our findings but does not invalidate them. While the backbone of meta-analysis and traditional systematic review is aggregation, realist synthesis refines theories by obtaining a rich (rather than necessarily complete) evidence base of reports of how interventions generate certain pattern of outcome.82 We also consider as a limitation the delay in preparing the review for publication after the end of the search in December 2014. During this period, new studies might have been published, the inclusion of which may enrich further our findings. Finally, initial screening by just one author might be seen as a limitation, but we found such high consistency between that author's judgement and a second author in a pilot phase of the project that we judged single screening to make the best use of the inevitably limited resources in the country, where the research was conducted.
We conclude that it has been possible to assemble, from a heterogeneous database, some patterns in the links between CMOs that are consistent enough to guide the practice of nutrition education. Our findings have refined some existing candidate theories, which researchers, also, apply to their work on nutrition education.
Acknowledgments
The authors wish to thank MrFuseini Abdulai Braimah, senior library assistant, School of Medicine and Health Sciences, University for Development Studies, Ghana for his support in helping to retrieve full texts of some of the included studies.
References
Footnotes
Contributors VM and TD were responsible for the conception and design of the study. VM was principally responsible for searching, sourcing and initial screening of studies. VM, MGC and TD further screened studies based on abstracts. Quality assessment was performed by VM, AJJAS, FS and MGC. VM was responsible for data extraction, synthesis and interpretation of the data and drafting of the manuscript. AJJAS, TD, FS, MGC and PA contributed to interpretation of the data and revision of the article. All authors approved the article for publication.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement VM had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.