Article Text

Abstract
Objectives To conduct the first systematic review from an epidemiological perspective regarding the association between high-heeled shoe wear and hallux valgus, musculoskeletal pain, osteoarthritis (OA) and both first-party and second-party injury in human participants without prior musculoskeletal conditions.
Setting A systematic review of international peer-reviewed scientific literature across seven major languages.
Data sources Searches were conducted on seven major bibliographic databases in July 2015 to initially identify all scholarly articles on high-heeled shoes. Supplementary manual searches were conducted. Titles, abstracts and full-text articles were sequentially screened to identify all articles assessing epidemiological evidence regarding the association between high-heeled shoe wear and hallux valgus, musculoskeletal pain, OA and both first-party and second-party injury in human participants without prior musculoskeletal conditions. Standardised data extraction and quality assessment (Threats to Validity tool) were conducted.
Primary and secondary outcome measures Musculoskeletal pain or OA as assessed by clinical diagnosis or clinical assessment tool. First-party or second-party injury.
Results 644 unique records were identified, 56 full-text articles were screened and 18 studies included in the review. Four studies assessed the relationship with hallux valgus and three found a significant association. Two studies assessed the association with OA and neither found a significant association. Five studies assessed the association with musculoskeletal pain and three found a significant association. Eight studies assessed first-party injury and seven found evidence of a significant injury toll associated with high-heeled shoes. One study provided data on second-party injury and the injury toll was low.
Conclusions High-heeled shoes were shown to be associated with hallux valgus, musculoskeletal pain and first-party injury. No conclusive evidence regarding OA and second-party injury was found. Societal and clinical relevance of these findings is discussed. Concern is expressed about the expectation to wear high-heeled shoes in some work and social situations and access by children.
- ACCIDENT & EMERGENCY MEDICINE
- EPIDEMIOLOGY
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We present the first systematic review of high-heeled shoes and health from an epidemiological perspective.
We situate the evidence in the context of wider public debate.
We were able to consider evidence published in seven languages.
We could not include non-European languages and two articles were not retrievable.
There was a lack of standardisation of heel height cut-offs between studies.
Introduction
High-heeled shoes (high heels) are a powerful symbol of modern female sexuality1 that have been shown to increase women's attractiveness to men and influence men's behaviour towards women in experimental studies.2 ,3 It has been suggested that this effect may result from an exaggeration of prototypical feminine gait.3 Compliance to social norms4 ,5 is a key driver of human behaviour and fashion6 including use of high heels7 ,8 is a clear manifestation of this. Being associated more with occasions than non-occasions,7 ,8 use of high heels may be seen as highly desirable and even compulsory at certain workplaces and social events.9–12
Concerns regarding the potential impact of high heels on women's health have been expressed in medical circles for over 50 years13 and in 2001 podiatrist William Rossi declared footwear to be the primary cause of foot disorders.14 A narrative review from an experimental biomechanical perspective in 201415 concluded that high heels cause qualitatively consistent alterations to the neuromechanics of walking gait and affect the kinematics and kinetics of bodily structures from the toes to the spine in ways that may be seen as biomechanical markers of musculoskeletal conditions such as hallux valgus (HV) and osteoarthritis (OA), which are both more common in women than men.16 ,17 However, no review from an epidemiological perspective could be identified and indeed a relative lack of epidemiological evidence was cited over 15 years ago9 as a barrier to the introduction of measures to prevent women being required to wear high heels as part of employer dress codes.
Moreover, the potential for high heels to inflict injury both on the wearer and on bystanders should be considered. For example, Williams and Haines18 identified 240 emergency department (ED) presentations over a 5-year period in the Australian state of Victoria resulting from first-party injury from high heels and a further 65 resulting from second-party injury from high heels. Since pressure is inversely associated with the cross-sectional area through which a force is applied,19 the potential for high heel shoe wearing to result in injury to both the wearer and on bystanders should be considered. Such shoes are exempt from restrictions on wear in public places and age restrictions on sale that are imposed on other sharp bladed objects such as knives in countries such as the UK20 and Australia.21
The systematic review presented in this article sought to assess existing epidemiological evidence associating exposure to high heels with at least one of the following outcomes in human participants without clinically significant musculoskeletal conditions prior to measurement: (1) OA, musculoskeletal pain or HV verifiable either by clinical diagnosis or clinical assessment tool or (2) injury to first or second party.
Methods
Design
A systematic review design was used following the PRISMA statement22 adapting the approach to the epidemiological rather than interventional nature of this review. MSB was the lead reviewer and JB performed independent quality assurance on a 20% sample of title screening, abstract screening, full-text screening, data extraction and quality assessment. Any discrepancies were resolved by discussion between the reviewers. Searches were designed and conducted by MSB.
Data sources
The bibliographical databases MEDLINE (Ovid), EMBASE (Ovid), AMED (Ovid), PsycINFO (Ovid), Cochrane Central Register of Controlled Trials (Cochrane), CINAHL (EBSCO) and Web of Science (Thomson Reuters, excluding patents) were searched from inception to July 2015. In order to maximise coverage, it was decided to search for all scholarly articles on high heels and then achieve greater focus through screening. Since there were no appropriate MeSH terms, databases were searched with the following keywords linked by the OR function: ‘positive heel inclination’, ‘high heel’, ‘high-heeled’, ‘high heeled’, ‘wedge heel’, ‘platform heel’, ‘platform shoe’, ‘stiletto’ and ‘elevator shoe’. This same exact combination of search keywords was presented to each database. Supplementary searches were conducted using Google Scholar, reference lists of relevant retrieved articles and also general internet searches using the Google search engine to identify media coverage and/or press releases on high heels and health in order to seek the original publication source.
Inclusion criteria
The following inclusion criteria were applied sequentially. Initially, titles and abstracts were screened and then full-text copies of all potentially relevant articles were sought. Full-text articles were retrieved in electronic form where this was available, otherwise in paper copy. An array of leading research libraries were accessible to the authors including the British Library. If an article could not be retrieved from any of these sources, it was excluded. A list of excluded articles with reasons is provided in online supplementary table S1.
Full-text original empirical peer-reviewed scientific journal articles.
Published in English, French, German, Spanish, Italian, Dutch or Portuguese.
Able to be retrieved.
Providing data to associate use of high heels with at least one of: (1) OA, musculoskeletal pain or HV verifiable either by clinical diagnosis or clinical assessment tool or (2) injury to first or second party.
Assessing human participants without prior history of clinically significant musculoskeletal conditions or other serious medical conditions likely to affect outcomes.
Using any quantitative epidemiological design including epidemiological elements embedded into biomechanical studies.
Data extraction and quality assessment
Data were extracted onto a standardised data extraction form. The following data were collected: bibliographic details, language of publication, country of study, study design, participants, measures of exposure, measures of outcome and principal findings. MSB contacted corresponding authors where appropriate to seek required clarifications. Measures of heel height that had been expressed in inches were converted to cm at 1 inch=2.54 cm.23 Only aspects of studies that meet inclusion criteria for this review are presented. Quality assessment was conducted at the study level using the Threats to Validity tool,24 which is a dynamic tool that is designed to be adaptable to any observational data set.
Results
A concise summary of the included studies is provided in table 1. Detailed study characteristics are shown in online supplementary table S2, detailed results in online supplementary table S3 and detailed quality assessment in online supplementary table S4. Meta-analysis was unable to be undertaken due to the heterogeneity of results. Results were thematically described.
Summary of included studies
Study profile
Searches identified 644 unique records, of which 56 were screened at the full-text stage and 18 included in the review. Database searches yielded 95% of unique records and supplementary searches yielded 5% (see figure 1 for detailed study flow chart). The total sample size was 14 647. Eleven studies (61%) assessed heel height only in women, while seven studies (39%) assessed both men and women. All studies fulfilling the inclusion criteria were published in English. Five studies were conducted in the USA, four in the UK, three in Australia, two in Taiwan and one in each of Brazil, Japan, Malaysia and Thailand. Six studies (33%) were assessed as high quality, eight (44%) as moderate quality and four (22%) as low quality.

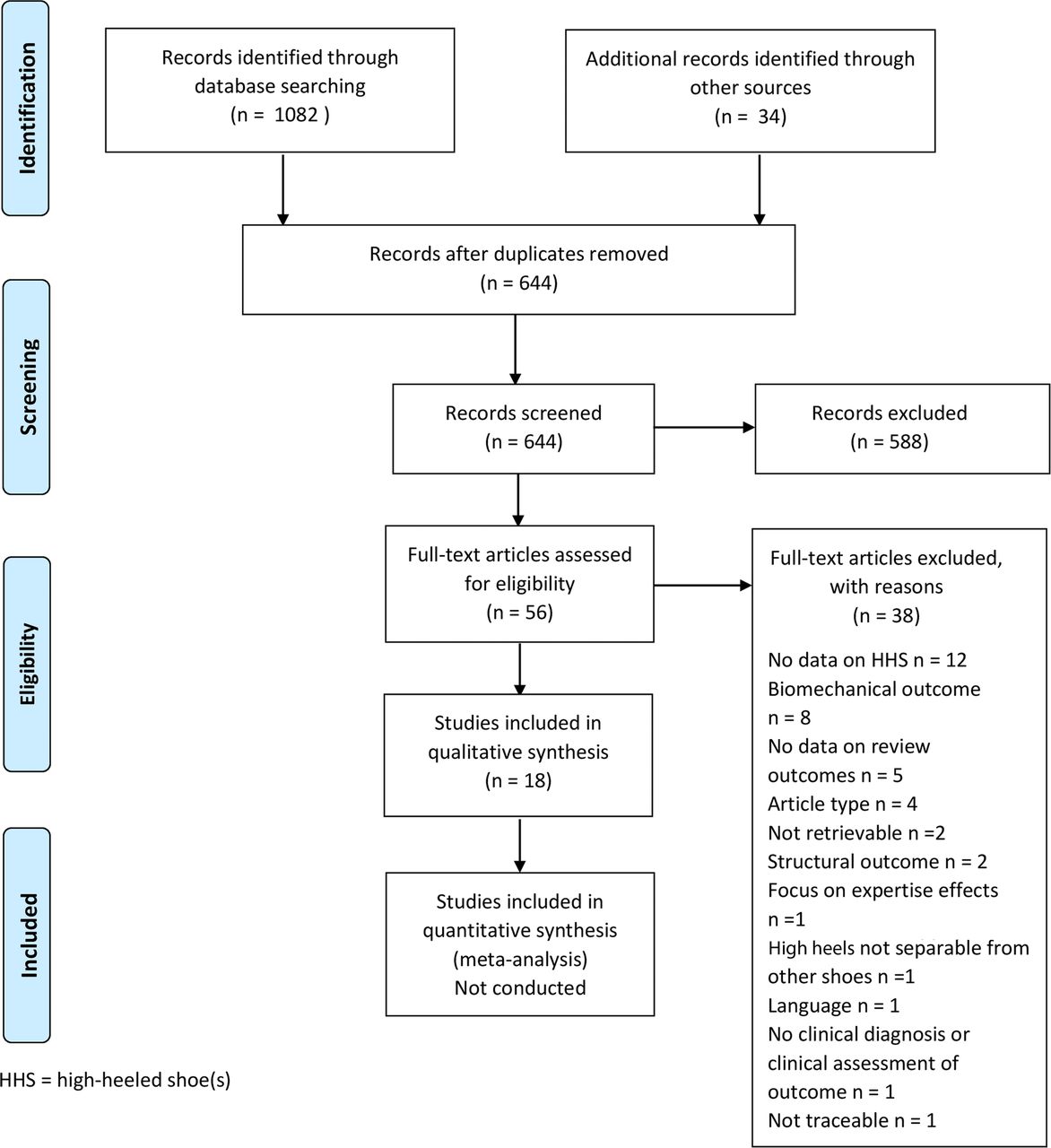{kind=link}
PRISMA flow diagram.
Musculoskeletal conditions
Four studies assessed the association between high heels and HV risk, of which three25–27(75%) found a significant association and one28 did not. Of the three positive studies, one25 was assessed as high quality and two26 ,27 as moderate quality. The negative study had a sample size of only 93 and was assessed as low quality. Menz and Morris26 found a significant association only with current not past use of high heels. Dufour et al25 and Menz and Morris26 both reported ORs. The former reported an OR of 1.24 for HV for those who ‘sometimes’ wore high heels in the past compared to those who ‘never’ wore high heels and an OR of 1.47 for those who ‘always’ wore high heels, while the latter reported an OR of 2.48 for HV for those who currently wore high heels outdoors compared to those who did not.
Two studies29 ,30 assessed the association between high heels and OA risk and neither found a significant association. One29 was assessed as moderate quality and the other30 as low quality. Five studies assessed the association between high heels and musculoskeletal pain risk, of which three31–33(60%) found a significant association and two28 ,34 (40%) did not. Of the three positive studies, two32 ,33 were assessed as moderate quality and one31 as low quality. Both negative studies were assessed as low quality. Chua et al31 provided an OR of 1.60 for the association between use of high heels and foot pain. Hong et al32 and Yung-Hui and Wei-Hsien33 provided analysis of variance F values of 56.8 and 46.8, respectively.
Injury
Eight studies assessed the association between high heels and first-party injury, of which seven18 ,35–40 (88%) were positive and one41(12%) was negative. Of the positive studies, five18 ,35 ,37 ,38 ,40 were assessed as high quality and two36 ,39 as moderate quality. The only negative study was assessed as moderate quality. Studies on first-party injury differed more in terms of design than other studies included in this review so require more detailed in-text results.
Chaiklieng and Suggaravetsiri35 found a significant association between use of high heels and repetitive strain injury in teachers (OR=1.60). Keegan et al37 profiled footwear worn at time of fall by participants who fractured and those who did not and found that medium-to-high heel height was associated with increased risk of fracture of the foot (OR=2.0), distal forearm (OR=1.7), proximal humerus (OR=1.5), pelvis (OR=1.5) and shaft of the tibia/fibula (OR=1.7). Tencer et al40 found a significant association between high heels and fall risk in older adults (OR=1.9). Gabell et al36 found that heel height habit was among the top 2 predisposing factors for falls in older adults even though no participant was wearing high heels at the time of falling. Moreover, past wear of high heels was associated with increased risk of multiple rather than single falls. Nagata39 found that 74% of occupational stair injuries to women under the age of 24 involved high-heeled or semi-high-heeled shoes, with women wearing these shoes being particularly prone to fall after catching the heel on the edge of the steps. Sherrington and Menz,41 however, found that only 2% of participants were wearing high heels at time of fall-related hip fracture and that no association was found between tripping or slipping and use of high heels.
Two studies18 ,38 took a very different approach to assessing the association between use of high heels and injury. Rather than surveying people and comparing outcomes between those that were and were not wearing high heels, they used pre-existing data from major databases regarding ED presentation to profile the number of injuries presenting to ED that were clinically attributed by the ED physician to be caused by use of high heels. Williams and Haines18 studied ED presentations over a 5-year period in the Australian state of Victoria and found 240 ED presentations resulting from first-party injury from high heels. Women accounted for 98% of patients and men 2%. The most common injury site was the ankle (51%) followed by the foot including the toes (26%). The most common age brackets were 20–24 (26%) and 25–29 (19%). Twelve presentations (5%) concerned children up to and including the age of 14 with 24 further presentations (10%) in the 15–19 age range. The estimated cost of the first-party injury presentations to the Victorian public hospital system was estimated to be $A71,579.62 over a 5-year period. In a larger-scale study, Moore et al38 studied ED presentations over a 10-year period in the US Consumer Product Safety Commission's National Electronic Injury Surveillance System, which provides a scalable estimate for the whole US. They identified 3294 ED presentations relating to first-party injury from high heels in women, which provides a US-wide estimate of 123 355 presentations taking into account the sampling weight. The most common injury site was the ankle (39%) followed by the foot (33%). The most common injury type was strain or sprain (53%) followed by fractures (19%). The most common age brackets were 20–29 (33%) and 30–39 (20%). There were 4737 injuries (4%) to children aged 0–9 and a further 17 530 injuries (14%) in the 10–19 age bracket.
Only one study18 presented any data regarding the association between high heels and second-party injury. In this study, which was assessed as high quality, the authors presented the number of second-party injuries from high heels over a 5-year period in Victoria in their ED presentations database and then excluded second-party injuries from further analysis. There were 49 ED presentations resulting from being stepped on by high heels and 16 resulting from assault with high heels.
Discussion
This is the first review of the potential health impact of high heels from an epidemiological perspective. The first major finding is that the identified body of literature taking this approach (18 studies) is smaller than the body of literature taking a biomechanical approach, which a preliminary search ahead of this review estimated to be in the order of 100 studies. The second major finding is that there is strong evidence that high heels are associated with first-party injury but that scientific evidence regarding second-party injury is limited. The third major finding is the injury toll among underage girls including 4737 injuries to those under the age of 10 in the study by Moore et al.38 The fourth major finding is that the balance of evidence is in favour of an association between high heels and increased risk of both HV and musculoskeletal pain. The fifth major finding is that no evidence was found of an association between high heels and OA.
The biomechanical and epidemiological approaches both have their associated strengths and limitations and should be considered complementary. Combining evidence from both approaches, which is called triangulation, can strengthen and corroborate the evidence base.42 In comparison with biomechanical studies of high heels, epidemiological studies do not rely on biomechanical proxies of clinical conditions, consider habitual exposure to high heels beyond the data collection session and tend to be conducted on larger samples. However, they tend to be observational, may be subject to recall bias regarding past exposure, may be affected by residual confounding and may not be able to separate the effects of different shoe parameters. With regard to confounding, for example, studies included in the current review have a wide variety of age ranges and the effects of high heels and the ageing process on outcomes may not be entirely separable. On the other hand, biomechanical studies such as that by Kerrigan et al43 can separate the effects of heel height and heel width. Recall bias may be particularly problematic in case–control studies,44 which may partly explain the negative findings of McWilliams et al30 and Dawson et al29 regarding OA. The use of pre-existing databases as in the studies of Williams and Haines18 and Moore et al38 offers a unique population-level insight into the burden of high heels-related injury and overcomes issues of selection bias in recruitment. However, as acknowledged by the authors, this approach may be subject to clinical misclassification bias—in the case of high heels-related injury, it is likely that the bias is in the direction of under-reporting of the role of high heels where alcohol was also a factor in ED admission. Moreover, although the epidemiological approach offers greater direct insight into clinical features than the biomechanical approach, differences in diagnostic criteria, grading systems and classifications may present a further limitation.
The balance of the evidence regarding the association between high heels and musculoskeletal pain, taking into account study quality, supports the existence of an association. This is corroborated by women's everyday experience of high heels as explored, for example, in the qualitative research of Dilley et al.8 All but one low quality study identified an association between high heels and HV, which is corroborated by biomechanical evidence, for example, an increase in forefoot pressure and loading at the first metatarsal head.45–48 The lack of association between high heels and OA is an unexpected finding, which may partly be explained by low study quality, recall bias regarding past shoe exposure and a particularly small sample size (n=29 for cases) in one study.29 In contrast, there is considerable biomechanical evidence suggesting an association between high heels and OA of the knee, for example, increased knee flexion49–52 and patellofemoral joint pressure.53
The body of evidence regarding first-party injury is larger than the other outcomes in this review and is consistently positive with the exception of one study41 in which only footwear worn at the time of fall was considered and very few participants (2%) in this study were wearing high heels at the time of their fall, which would result in statistical power problems in comparing the outcome of times when high heels were or were not worn. Nagata39 usefully highlights the potential hazard of climbing stairs in high heels, while Gabell et al36 highlight that the physiological impact of wearing high heels may predispose women to a greater risk of falling even when they are not wearing high heels at the time of their fall. This finding should be interpreted in combination with evidence of stiffening and shortening of the Achilles tendon54 and radiographic evidence of alterations to the spinopelvic structure55 associated with use of high heels. Indeed, these structural adaptations may be a possible explanation for the finding of Gabell et al36 that high heels wearing habit may predispose women to falling even when not wearing high heels at the time of the fall. The two studies assessing ED presentations18 ,38 provide insight into the clinical significance of first-party injury from high heels and especially the larger study by Moore et al38 gives insight into both the clinical and demographic spectrum of injuries incurred. The injury toll among girls under the legal age of adulthood including a large number of under 10s is striking. However, neither study classified age in a way that allows precise division of legal adults from those below the legal age of adulthood.
In this context, it is important to note that there are styles of high heels specifically marketed for children,56 ,57 there is no age restriction on the sale of high heels in countries such as England and Australia, where such restrictions exist for many other items,20 ,21 ,58 ,59 and in our experience few high schools prohibit girls under the legal age of adulthood from wearing high heels to school functions such as proms, while some schools encourage it (M. Barnish, personal communication). It is also important to note that some employers’ dress codes and social event organisers require women to wear high heels.9–12 Some health-related organisations have called for compulsory wear of high heels at work to be outlawed, however to the best of our knowledge no country has enacted such legislation. For example, in 2009 the Society of Chiropodists and Podiatrists (UK) made a statement that “women workers should not be made to adhere to a dress code that can damage their feet and should have the choice to wear footwear that will not leave them prone to long term foot health problems.”10 In light of the findings of our review with regard to HV, pain and especially injury, we recommend that health-related organisations engage in further constructive dialogue with governments and other policymakers regarding the compulsion to wear high heels at work as well as social events and regarding access to high heels among girls under the legal age of adulthood.
We have a number of suggestions for future research. First, noting that the absence of evidence is not evidence of the absence of a relationship,60 further epidemiological research is required to assess the potential association between high heels and OA as suggested by biomechanical studies but not evidenced in the current review. Second, the risk of second-party injury associated with clothing in general and high heels in particular is an area that has been under-researched and deserves further attention. Third, building on the work of Dilley et al8 and Woodward,7 it is recommended to investigate the level of awareness of health issues relating to high heels, what role this plays in footwear choice and whether certain categories of women (eg,competitive sportswomen and health professionals) are less likely to wear high heels than the general population. These studies would help determine the likelihood of a health educational intervention being effective, noting that considerable information on high heels and health is already available to the public from sources such as WebMD61 and media reports of research on high heels. Fourth, we suggest that use of high heels is taken into account in future studies of women's and musculoskeletal health to address the potential confounding effects of the use of high heels on the relationships being investigated.
This review has several notable strengths. First, it provides what is to our knowledge the first review of the relationship between high heels and health from an epidemiological perspective. Second, it situates the evidence in the context of wider public debate. Third, it offers a systematic approach to inclusion, data extraction, quality assessment and reporting in order to minimise the risk of bias. Fourth, drawing on the linguistic skills of the authors, articles in seven languages could be considered for inclusion. Fifth, this review included a range of clinically relevant outcomes in order to maximise clinical and policy relevance.
There are, however, a few limitations to this review that should be taken into account. First, while the range of eligible languages was relatively wide, it was focused on European languages and may not allow complete coverage of the world's literature. Second, two articles (4% of those selected for full-text screening) could not be retrieved. Third, while two reviewers conducted screening, data extraction and quality assessment, only one reviewer designed and conducted the searches. Fourth, the variety of outcome measures and the cut-offs for what constituted high heels precluded the use of meta-analysis. If these aspects could be better-standardised in future epidemiological research on high heels, a meta-analysis could be considered when this systematic review is due for update. In addition, the variability of cut-offs for heel height and the frequent failure of studies to take into account factors such as heel shape may reduce the precision of the findings and in some cases may explain the absence of significant results. With regard to heel shape, it is possible that the effect of stiletto, platform and wedge heels for example, may differ and that curved heels and ‘heelless heels’, which are now fashionable, may have a different effect than more traditional heel styles.
Here we present a systematic review of epidemiological evidence relating the use of high heels to musculoskeletal health outcomes. A future review on this topic could seek to integrate the hitherto relatively separate bodies of biomechanical and epidemiological literature.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
- Data supplement 4 - Online table 4
Footnotes
MSB is the senior author and is currently at Epidemiology Group, Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, UK.
Contributors MSB was responsible for conceptualisation and project management, search design and execution. MSB and JB were responsible for screening, data extraction, quality assessment and interpretation. MSB prepared the first draft. MSB and JB were responsible for revisions and approval to submit manuscript. MSB is the guarantor.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.