Article Text

Abstract
Objectives Children's exposure to secondhand smoke (SHS) is causally linked to childhood morbidity and mortality. Over 38% of English children (aged 4–15) whose parents are smokers are exposed to SHS in the home. Little is known about the prevalence of SHS exposure in the homes of young infants (≤3 months). This study aimed to estimate maternal self-reported prevalence of SHS exposure among infants of women who smoked just before or during pregnancy, and identify factors associated with exposure.
Setting Primary Care, Nottingham, England.
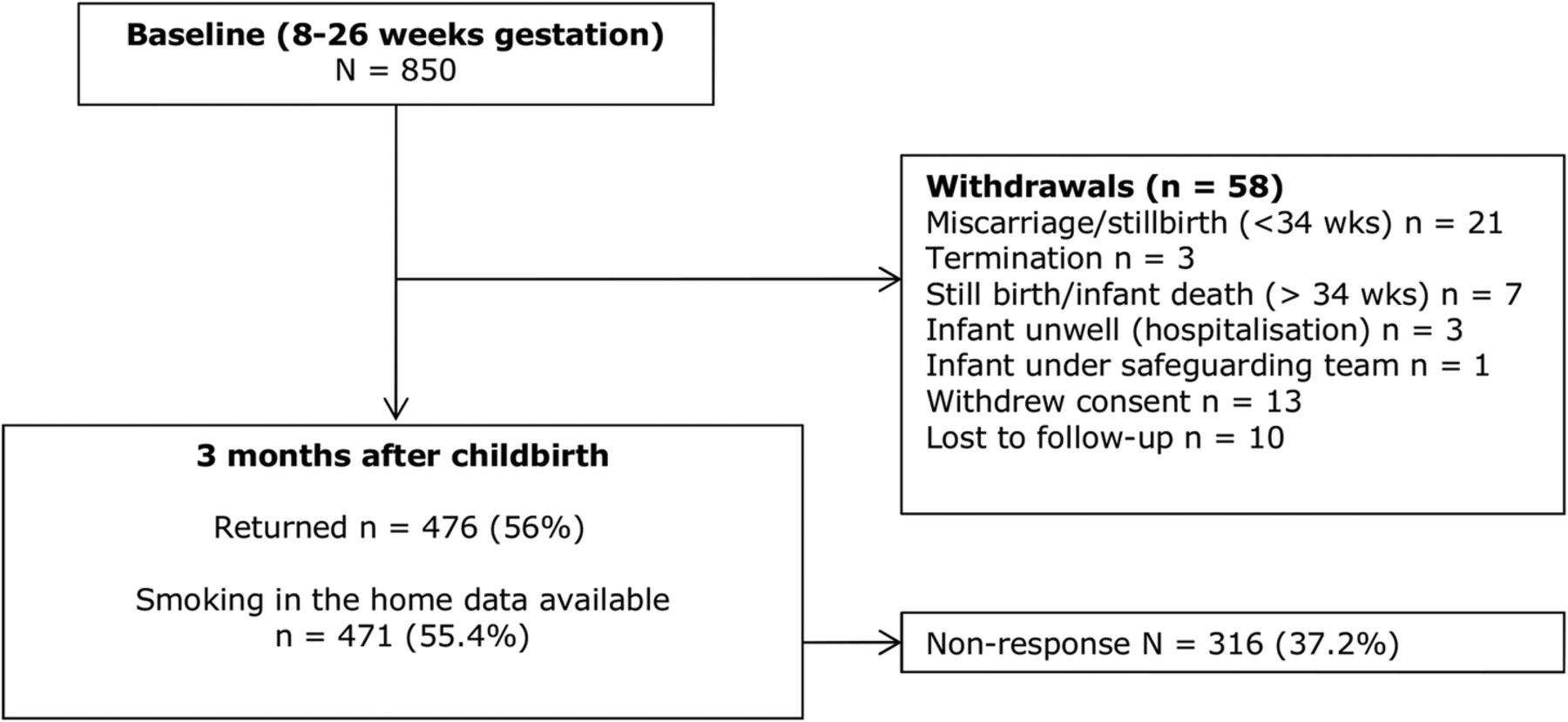
Participants Current and recent ex-smoking pregnant women (n=850) were recruited in Nottingham, England. Women completed questionnaires at 8–26 weeks gestation and 3 months after childbirth. Data on smoking in the home 3 months after childbirth was available for 471 households.
Primary and secondary outcome measures Maternal-reported smoking in the home 3 months after childbirth.
Results The prevalence of smoking in the home 3 months after childbirth was 16.3% (95% CI 13.2% to 19.8%) and after multiple imputation controlling for non-response 18.2% (95% CI 14.0% to 22.5%). 59% of mothers were current smokers; of these, 24% reported that smoking occurred in their home compared to 4.7% of non-smokers. In multivariable logistic regression, mothers smoking ≥11 cigarettes per day were 8.2 times (95% CI 3.4 to 19.6) more likely to report smoking in the home. Younger age, being of non-white ethnicity, increased deprivation and less negative attitudes towards SHS were also associated with smoking in the home.
Conclusions This survey of smoking in the home 3 months after childbirth found a lower prevalence than has been reported in older children. Interventions to support smoking mothers to quit, or to help them restrict smoking in the home, should target attitudinal change and address inequality relating to social disadvantage, younger age and non-white ethnic groups.
- PAEDIATRICS
- PRIMARY CARE
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first survey since the introduction of smoke-free legislation, as far as we are aware, of smoking in the home immediately after childbirth.
During recruitment, 96% of women attending selected antenatal clinics within Nottingham University Hospital Trust were screened for eligibility, accounting for around one-third of all births within Nottingham, England, during this time.
The demographic profile of smokers within this cohort is similar to other UK pregnancy cohorts, meaning the sample is likely to be broadly representative.
A potential limitation was the reliance on reported smoking measures.
There were some differences between those who responded and those who did not respond at follow-up, however appropriate imputation methods were used to allow for this non-response bias.
Background
Exposure to secondhand smoke (SHS) is the involuntary inhalation of other people's cigarette smoke and globally, 40% of children are exposed.1 Children's SHS exposure has been causally linked to respiratory tract infections, middle ear disease, sudden unexplained death in infancy and asthma.2 The WHO believes that SHS is a substantial threat to child health,3 and the US Surgeon General argues there is no safe exposure level.4
In 2008, a study conducted in England reported 52% of children aged 4–15 whose parents were smokers were exposed to SHS in the home.5 This has reduced in recent years, with a reported 38.7% of children of smoking parents aged 4–15 years being exposed to SHS in the home in England in 2012,6 however it clearly remains a significant problem. Similar trends have been observed elsewhere, both in the UK,7–10 and internationally (eg, USA;11 ,12 Ireland, France, Germany and the Netherlands 13). However, current UK prevalence estimates for children's SHS exposure in the home focus on children aged >4 years,6–10 ,14–16 and most studies include children aged 10–11 years.7–10 ,16 There is therefore little research examining SHS exposure in the home among young infants (≤3 months) and few prevalence estimates. We are aware of only one UK study estimating the prevalence of SHS among young infants. Among children of smokers, 82% of infants (average age 3 months) experienced SHS exposure in the home.17 Elsewhere, we are aware of just two studies, from the USA, in which 10.8–21.4% of infants of smoking mothers aged ≤9 months were exposed to SHS in the home18 and 24.5% were exposed to SHS for ≥1 h per day.19 Although these studies suggest SHS exposure may be a substantial issue, they were conducted prior to,17 ,19 or around the time18 that comprehensive smoke-free legislations were introduced. There are no contemporary estimates of prevalence in this age group.
Additionally, of 41 studies investigating factors associated with children's SHS exposure in the home identified by systematic review,20 only three19 ,21 ,22 included infants or children aged <2 years. This review found parental smoking, low socioeconomic status (SES) and being less educated were all consistently independently associated with children's SHS exposure in the home.20 However, due to the small number of studies focusing on younger age groups, little is known about the influences on SHS exposure in the home experienced by young infants; consequently, this paper reports the prevalence of SHS exposure among young infants born to women from an English pregnancy cohort, and identifies factors associated with this exposure.
Methods
This study presents secondary analysis on data collected as part of the longitudinal cohort, the Pregnancy Lifestyle Survey (PLS); methods and cohort characteristics have been described in detail previously.23 The study received a favourable opinion from Derbyshire Research Ethics Proportionate Review Sub-Committee (reference 11/EM/0078).
Participants
The baseline sample size for the PLS was 850, based on the cohort's primary aim to estimate the proportion of smokers who initiate quit attempts in the second or third trimester of pregnancy.23 Women who were aged ≥16 years, between 8 and 26 weeks pregnant, and self-reported being current smokers or having smoked in the 3 months prior to pregnancy were eligible for participation.
Recruitment and data collection
Participants were recruited between August 2011 and August 2012 at two antenatal clinics within Nottingham University Hospitals NHS Trust, England. Participants completed a baseline questionnaire in the antenatal clinic when they were between 8 and 26 weeks gestation, and a follow-up questionnaire when their baby was 3 months old. At Follow-up, hospital administration staff obtained participants’ delivery dates from their antenatal records. Participants were sent a questionnaire 3 months after their delivery date by post or email; if not returned, completion by telephone was attempted.
The questionnaires have been described elsewhere.23 In summary, both the baseline and the follow-up questionnaires were similar in format and content, using yes/no, multiple choice and five-point Likert items. The baseline questionnaire was divided into six sections: screening questions, health and pregnancy, smoking beliefs, current smoking behaviour, interest in getting help to stop smoking and sociodemographic information. At the 3-month follow-up, the same topics were covered but edited to reflect women's postnatal status. Additional questions about smoking in the home, and beliefs about harm caused to infants and children through SHS exposure were included.
Outcomes
The primary outcome measure was maternal-reported smoking by either themselves or someone else in their home 3 months after childbirth, using participants’ responses to the questions ‘how often do you smoke in your home nowadays?’ and ‘how often do other people smoke in your home nowadays?’. Responses used Likert items ranging from 1 (‘never’) to 5 (‘very often’). A binary outcome was created, where participants who responded ‘almost never’ to ‘very often’ (2–5 on scale) to either of these questions were considered to have smoking in the home 3 months after childbirth, and participants who responded ‘never’ to have a smoke-free home.
The maternal sociodemographic characteristics of age, ethnicity, highest qualification, age left full-time education and current employment status were taken from baseline questionnaires. Age left full-time education was categorised as ≤16 years (UK age of compulsory education), ≥16 years and still in full-time education. Ethnicity was categorised as a binary variable (white British vs other ethnicity) due to small numbers of participants in non-white British ethnic groups. A measure of socioeconomic status (SES) was created by mapping participants’ postcodes with corresponding 2007 Indices of Multiple Deprivation (IMD) scores, taken from routine UK Data Service data.24 The 2007 IMD measures a range of domains reflecting economic, social and housing issues, where higher scores reflect greater deprivation. Scores were divided into tertile groups.
Participant's self-reported smoking behaviour was measured at both time points. Women were categorised as being a non-smoker, or smoking 0–5, 6–10, ≥11 cigarettes per day. Heaviness of smoking index (HSI) scores were calculated using the method described by Borland et al25 Partner smoking status at 3 months after childbirth was categorised as non-smoker, smoker or not applicable/no partner.
Attitudes to children's SHS exposure were measured by asking participants the extent to which they agreed with four attitudinal statements using Likert items (figure 1). The items had high-internal consistency (Cronbach's α=0.9),26 and so responses were combined into a single summed score (out of 20), whereby a higher score reflected a more negative attitude towards children's SHS exposure. Attitude scores were highly negatively skewed, and so were categorised into a binary variable; a score of ≥15 represented ‘negative attitudes towards child SHS exposure’ and a score of <15 ‘less negative attitudes towards child SHS exposure’.

Attitudes to child secondhand smoke exposure scale items.
Data analysis
Statistical analyses were conducted using Stata V.13.27 Cohort characteristics and the characteristics of responders and non-responders at 3 months after childbirth are presented, and differences examined using χ2 tests for categorical data and t tests for continuous data. The prevalence of smoking in the home was estimated using those with complete data; given that there was a high level (50%) of missing data at 3 months after childbirth and observed differences in the characteristics of responders and non-responders, multiple imputation methods28 were used to impute values for missing outcome data. Five imputed data sets were considered sufficient29 and were constructed using the mi command in Stata, based on the following baseline variables: smoking behaviour, HSI, age, ethnicity, qualifications, employment, IMD score and partner smoking status. These variables were selected based on characteristics associated with child SHS exposure in the home in a previous systematic review20 and variables associated with non-response.30 The imputed outcome variable was only used for estimates of prevalence of smoking in the home; all other analyses were conducted using the original non-imputed outcome variable.
The variables smoking behaviour at baseline, smoking behaviour 3 months after childbirth, age, ethnicity, highest qualification, age left full-time education, employment status, IMD, partner smoking status and attitude towards child SHS exposure score were entered into a univariate logistic regression analysis and the ORs and 95% CI calculated. For continuous exposure variables, the linearity of the effect was tested using the likelihood-ratio test.
Those variables that were statistically significant in univariate analysis at the p<0.05 level, or with strong a priori assumptions (eg, maternal education) based on the findings of a systematic review,20 were entered into exploratory multivariable logistic regression models. Correlations were observed between smoking behaviour at baseline, smoking behaviour at 3 months after childbirth and baseline HSI. Smoking behaviour at 3 months after childbirth was most strongly associated with the outcome measure, and was therefore included in the multivariable analyses and the other smoking variables omitted to avoid collinearity. Similarly, highest qualification and age left full-time education were considered in the multivariable analysis independently due to collinearity. Those variables reaching significance (p<0.05) were retained in the model, and non-significant variables re-entered into the model sequentially. Participants with missing data for exposure variables were excluded from multivariable analysis (n=6). ORs, 95% CI, and likelihood ratio test p values and Wald's p values for trend for ordered categorical exposure variables are reported.
Results
Cohort characteristics
The cohort consisted of 850 pregnant women, of which 56.6% were current smokers at baseline (table 1). The demographic profile of smokers within the cohort was similar to other UK pregnancy cohorts.23
Cohort characteristics and comparison between responders and non-responders at 3 months postnatal
Follow-up response rates
At follow-up, the response rate was 56% (n=476) after non-response and withdrawal (figure 2). Owing to missing data in some of the returned questionnaires, smoking in the home information was available for 471 participants. Table 1 shows the characteristics of women who did and did not respond to the follow-up questionnaire 3 months after childbirth.

{kind=link}
{kind=link}
Consort diagram of response rates and reasons for withdrawal.
Smoking in the home 3 months after childbirth: prevalence and determinants
The ‘raw’ prevalence of smoking in the home 3 months after childbirth was 16.3% (95% CI 13.2% to 19.8%). At this time, 59% of mothers were current smokers; of these, 24% reported smoking in the home compared to 4.7% of non-smokers (table 2). After controlling for non-response bias using multiple imputation methods, prevalence of smoking in the home 3 months after childbirth was 18.2% (95% CI 14.0% to 22.5%).
Prevalence of smoking in the home, and univariate and multivariable analysis of associated factors
Table 2 shows the results of univariate analysis for factors associated with smoking in the home 3 months after childbirth, using non-imputed data. The strongest observed associations were for maternal smoking at 3 months after childbirth; those mothers smoking ≥11 cigarettes per day were 10.5 times more likely to report that smoking occurred in their home compared to non-smoking mothers at this time point. Maternal age, ethnicity, highest qualification, age left full-time education, IMD, partner smoking status and attitudes towards child SHS exposure score were also significantly associated with smoking in the home in univariate analysis.
In exploratory multivariable logistic regression modelling, smoking behaviour at 3 months after childbirth, younger maternal age, being of non-white British ethnicity, being more deprived as measured by IMD and holding less negative attitudes towards child SHS exposure were significantly associated with smoking in the home 3 months after childbirth (table 2). The strongest observed association was for mothers who smoked ≥11 cigarettes per day, who were over eight times more likely to report smoking occurred in their home.
Discussion
After multiple imputation to control for non-response, the prevalence of smoking in the home at 3 months following childbirth was 18.2%. Prevalence was higher in homes where mothers who smoked lived compared to those where mothers were non-smokers (24% and 4.7%, respectively). Mothers who were currently smoking ≥11 cigarettes per day, younger, of non-white ethnicity, more deprived and held less negative attitudes towards child SHS exposure were significantly more likely to report that smoking occurred in their home 3 months after childbirth.
As far as we are aware, this is the first survey to investigate smoking in the home immediately after childbirth since the introduction of UK smoke-free legislation. Our estimate of the prevalence of SHS in the home was similar to estimates among slightly older infants from the USA, where 10.8–24.5% of infants of smoking mothers were exposed.18 ,19 However, this was substantially lower than in the only previous UK survey in infants who were a similar age as those in our sample.17 In that study, 82% of infants aged on average 3 months old whose parents were smokers were exposed to SHS in the home. A number of factors are likely to have influenced our lower estimate of SHS exposure. Blackburn et al's17 study was conducted in 2003; smoke-free legislations have since been implemented across the UK and this may have increased awareness of SHS and its implications. Additionally, UK smoking prevalence has reduced since the earlier survey, in particular among those of childbearing age31; increasing numbers of UK households are reported as smoke-free2 and older children's SHS exposure in the home has reduced.5 ,10 Together these factors suggest that rates of smoking in the home will have declined since Blackburn's study.17
The observed prevalence of young infant's SHS exposure in the home is much lower than the most recent estimates of prevalence among older children in England, where 38.7% of children aged 4–15 years whose parents were smokers were exposed in the home in 2012.6 This finding is positive; young infants are particularly susceptible to the risks of SHS exposure as they have a higher respiration rate32 and underdeveloped lungs.33 This is exacerbated further as young infants experience increased SHS exposure due to the amount of time spent indoors in close proximity to smoking parents and surfaces such as carpets that have been contaminated with smoke, and having more hand to mouth contact compared to older children.34 However, SHS exposure is dangerous for children of all ages2; it is not yet known at what age parents or carers start to consider their children to be less vulnerable to the effects of SHS exposure and relax their home smoking restrictions. The early postnatal period, where the prevalence of SHS exposure in the home appears greatly reduced, may be a significant time-point to prevent future SHS exposure, before smoking in the home becomes an established behaviour.
In a recent systematic review,20 children whose parents were smokers, of low SES, less educated or held less negative attitudes towards SHS were at an increased risk of SHS exposure in the home, with the largest risks observed for children living in households with smokers. With the exception of parental education, the factors associated with young infant's SHS exposure in this study are similar to those among older children. The findings also show similarities to the current limited evidence base examining this in infants aged <2 years elsewhere; in the USA, having more children in the household, being of white ethnicity, low maternal education, low maternal age, being unmarried, lower income and markers of disadvantage during pregnancy were associated with infant SHS exposure.18 ,19
A strength of this study was that during recruitment, 96% of women attending selected antenatal clinics within Nottingham University Hospital Trust were screened for eligibility, accounting for around one-third of all births within Nottingham, England, during this time.23 The demographic profile of smokers within this cohort is similar to the composition of other UK pregnancy cohorts,23 meaning that the sample is likely to be broadly representative. A potential limitation of this research was the lack of power within analysis due to small numbers of participants in some exposure variable groups. Furthermore, there were some differences between those who responded and those who did not respond at follow-up, which are described. These differences may have impacted on our prevalence estimates, however appropriate imputation methods were used to allow for this non-response bias. Non-response biases are less likely to have impacted on estimates of association with smoking in the home. A further potential limitation was reliance on reported smoking measures; parents may be inclined to give socially desirable responses resulting in under-estimates of children's SHS exposure.35 However, maternal-reported SHS exposure has been found to correlate with urinary cotinine and home environmental nicotine (r range 0.3–0.6) in infants aged <2.5 years.36 As the cohort included only women who were current or recent ex-smokers during pregnancy, the prevalence estimate obtained does not reflect children's SHS exposure in the home in the general population. However, as parental smoking, and in particular maternal smoking within the home, is the primary source of children and infant's SHS exposure,20 this study gives a useful indication of the scale of young infant's SHS exposure.
While the demographic characteristics associated with smoking in the home after childbirth are not easily modifiable, they may help to inform which infants, parents or families are best targeted in future interventions. The findings highlight that the best way to prevent or reduce smoking in the home immediately after childbirth is to help smoking mothers to quit and stay abstinent after childbirth. However, a recent systematic review did not find a significant effect of any behavioural intervention approach to prevent postpartum smoking relapse,37 and as such more research is needed to identify interventions which can support women at this important time. Where women are unable or unwilling to quit smoking, making their home smoke-free is the next most effective way to protect children.38 This study, consistent with research in older children,20 shows that less negative attitudes towards SHS exposure is associated with smoking in the home after childbirth. Interventions targeting attitudes towards SHS by supporting parents to recognise the benefits of protecting children from SHS may therefore be useful to promote smoke-free homes.
Conclusions
The prevalence of smoking in homes where young infants live is lower than has been reported in older children (>3 months), suggesting that the early postnatal period may be an ideal time to intervene to prevent future SHS exposure in the home. The factors associated with smoking in the home immediately following childbirth were similar to those previously reported among older children. Interventions to support smoking mothers to quit, or to help them restrict smoking in the home, should target attitudinal change and address inequality relating to social disadvantage, younger age and non-white ethnic groups.
Acknowledgments
The authors would like to thank Nottingham University Hospital NHS Trust for facilitating this research. The authors also thank Katharine Bowker, Rachel Whitemore, Felix Naughton, Michael Ussher, Kate E Pickett, Jo Leonardi-Bee and Stephen Sutton for their invaluable input and assistance in the Pregnancy Lifestyle Survey.
References
Footnotes
Contributors SO, TC, LLJ, SC and SL conceived and designed the experiments. SO performed the experiments. SO and SL analysed the data. SO, TC, LLJ, SC and SL wrote the paper. All authors read and approved the final manuscript.
Funding SO is funded by the National Institute for Health Research (NIHR) School for Primary Care Research (NIHR SPCR). The NIHR SPCR is a partnership between the Universities of Birmingham, Bristol, Keele, Manchester, Nottingham, Oxford, Southampton and University College London. This article presents independent research funded by the NIHR under the Programme Grants for Applied Research programme (RP-PG-0109-10020). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Ethics approval Derbyshire Research Ethics Proportionate Review Sub-Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.