Article Text

Abstract
Objective Protective ventilation (PV) has been validated in patients with acute respiratory distress syndrome. However, the effect of PV in patients undergoing major surgery is controversial. The study aimed to explore the beneficial effect of PV on patients undergoing a major operation by systematic review and meta-analysis.
Setting Various levels of medical centres.
Participants Patients undergoing general anaesthesia.
Interventions PV with low tidal volume.
Primary and secondary outcome measures Study end points included acute lung injury (ALI), pneumonia, atelectasis, mortality, length of stay (LOS) in intensive care unit (ICU) and hospital.
Methods Databases including PubMed, Scopus, EBSCO and EMBASE were searched from inception to May 2015. Search strategies consisted of terms related to PV and anaesthesia. We reported OR for binary outcomes including ALI, mortality, pneumonia, atelectasis and other adverse outcomes. Weighted mean difference was reported for continuous outcomes such as LOS in the ICU and hospital, pH value, partial pressure of carbon dioxide, oxygenation and duration of mechanical ventilation (MV).
Main results A total of 22 citations were included in the systematic review and meta-analysis. PV had protective effect against the development of ALI as compared with the control group, with an OR of 0.41 (95% CI 0.19 to 0.87). PV tended to be beneficial with regard to the development of pneumonia (OR 0.46, 95% CI 0.16 to 1.28) and atelectasis (OR 0.68, 95% CI 0.46 to 1.01), but statistical significance was not reached. Other adverse outcomes such as new onset arrhythmia were significantly reduced with the use of PV (OR 0.47, 95% CI 0.48 to 0.93).
Conclusions The study demonstrates that PV can reduce the risk of ALI in patients undergoing major surgery. However, there is insufficient evidence that such a beneficial effect can be translated to more clinically relevant outcomes such as mortality or duration of MV.
Trial registration number The study was registered in PROSPERO (http://www.crd.york.ac.uk/PROSPERO/) under registration number CRD42013006416.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review shows that protective ventilation can prevent acute lung injury in patients who underwent major surgery.
The study was limited by the relatively small sample sizes of included studies, but the possibility of a small study effect cannot be excluded.
The strength of the study was the use of a Bayesian approach that enhanced the reliability of the systematic review.
There is no evidence that the use of protective ventilation is able to reduce mortality rates in patients who underwent major surgery.
Introduction
Mechanical ventilation (MV) comprises two major functions. One is to provide respiratory force to ventilate the lungs when the patient cannot breathe on his/her own; the other is to open collapsed areas of a diseased lung. A substantial number of patients with healthy lungs require MV for a variety of reasons. In the operating room, patients under general anaesthesia are incapable of breathing, and thus require MV support for respiration drive (eg, during general anaesthesia, respiratory muscle of the patient is paralysed and the respiratory drive is dependent on mechanical ventilation). In the intensive care unit (ICU), it has been reported that about 20% of patients need MV support because of neurological or neuromuscular diseases.1 In a nationwide survey involving 6 469 674 hospitalisations, Wunsch et al2 reported that among 180 326 patients who received invasive MV, only 13.2% had comorbidity of pulmonary disease.
In a diseased lung, typically acute respiratory distress syndrome (ARDS), MV has been extensively studied for its proper use. The most important ventilation strategy is the so-called ‘protective ventilation’ (PV). PV comprises three components that include low tidal volume, higher positive end-expiratory pressure (PEEP) and recruitment manoeuvre. In the landmark study by Acute Respiratory Distress Syndrome Network (ARDSnet), PV with low tidal volume was found to be associated with a relative reduction in mortality rate of 22% (31% vs 39.8%, p=0.007).3 This promising result has triggered numerous subsequent experimental and clinical studies, and PV has been repeatedly found to be beneficial for a diseased lung.4–6 In a recently updated systematic review, Petrucci and De Feo7 found that mortality can be reduced by the use of PV at day 28 and at the end of hospital stay.
It is still controversial on whether PV can provide a similar beneficial effect on healthy lungs. The proponents suggested that PV that has shown significantly reduced mortality in patients with lung injury could be extrapolated to a broader population, because the currently used clinical definition of ARDS lacks specificity that a substantial number of patients included in these trials had no diffuse alveolar damage.8 Furthermore, there is direct evidence from human trials that PV is potentially beneficial for patients with otherwise healthy lungs.9 ,10 However, the opponents contend that lung damage can only be induced with tidal volumes as large as twice the resting aerated compartment, and PV has no additional benefits for healthy lungs.11 ,12 Recently, there have been many trials conducted to investigate the effect of PV on clinical outcomes in patients who underwent general anaesthesia, but with conflicting results. The aim of the present study was to synthesise the best evidence in this topic by systematically reviewing these studies.
Methods
The study protocol had been registered in PROSPERO (http://www.crd.york.ac.uk/PROSPERO/) under registration number CRD42013006416, and detailed study protocol had been previously published by Zhang et al.13 We will briefly describe the method we used to conduct the systematic review.
Search strategy and eligibility
Databases including PubMed, Scopus, EBSCO and EMBASE were searched from inception to May 2015. Search strategies had been described in Zhang et al,13 and briefly it consisted terms related to PV and anaesthesia (see online supplementary file). There was no language restriction. Randomised controlled trials (RCTs) meeting the following criteria were included: (1) patients undergoing MV after induction of anaesthesia; (2) the intervention is lung PV.
Data extraction
The primary study end point was new onset acute lung injury (ALI), and secondary end points included: mortality, length of stay (LOS) in the ICU and hospital, atelectasis, pneumonia, pH value, partial pressure of carbon dioxide (PaCO2), oxygenation, duration of MV and other adverse outcomes such as arrhythmia. Binary outcomes were analysed by extracting data on the number of events in each arm. Continuous outcomes were analysed by extracting data on respective values of that outcome in each arm. Relevant information such as demographics, tidal volume and PEEP settings in the study and control arm and use of recruitment manoeuvre was abstracted from original articles. Qualities of included RCTs were assessed by using the adapted Delphi consensus. The Delphi consensus consisted of the following eight aspects: sequence generation, allocation concealment, blinding, eligibility criteria, baseline characteristics, use of point estimates and variability, intention-to-treat analysis and sample size calculation.
LZ, LC, XZ, XH and CH contributed to data acquisition in the study, and disagreement was settled by a discussion with a third opinion.
Statistical analysis
We reported OR for binary outcomes including ALI, mortality, pneumonia, atelectasis and other adverse outcomes. Weighted mean difference (WMD) was reported for continuous outcomes such as LOS in the ICU and hospital, pH value, PaCO2, oxygenation and duration of MV. The primary hypothesis was that PV with low tidal volume was able to reduce postoperative complication of ALI. The effect sizes were combined by conventional method (as compared with the Bayesian approach). Owing to the heterogeneity in component studies, we used a random-effects model to pool the data. If the number of studies reporting the same end point was enough, we performed subgroup analysis to investigate the heterogeneity. Publication bias was assessed by using Begg's rank correlation test and Egger's regression test. Furthermore, a funnel plot was depicted to visually assess the symmetry. A Bayesian approach was performed by using fixed-effects and random-effects models. Posterior estimates were reported after the simulation showed convergence. Statistical software Stata V.12.0 (College Station, Texas 77845, USA) and WinBugs14 (Imperial College & MRC, UK) were used. Two-tailed p<0.05 was considered statistically significant.
Results
Our initial search identified 125 citations from PubMed, 184 from Scopus, 166 from EBSCO and 289 from EMBASE. After a careful review by three independent reviewers, 25 studies were selected for full-text review. Three studies were excluded because two used the same cohort and one is not a real RCT, which resulted in a total of 22 citations being included for the final analysis (figure 1).14–35

Flow chart of database search and study selection.
Tables 1 and 2 show some important characteristics of individual component studies. In most studies, the mean ages ranged between 50 and 70 years. However, the mean age of Cai K's study was around 20 years. The percentage of male patients varied significantly across component studies, ranging from 41% to 83%. Tidal volumes in the PV group were significantly lower than in the control group, and PEEP was significantly higher in the PV group than in the control group. Risk of bias was assessed from 10 items. As shown in figure 2, all studies reported point estimate and variability for study end points. Baseline characteristics were comparable in most studies. However, the blindness to both outcome assessor and caregiver was not performed or unknown in most included studies.
Characteristics of included studies
Comparisons of ventilator settings between treatment and control groups

Risk of bias for included component studies assessed from items of blindness, sequence generation, allocation concealment, sample size calculation, clear definition of eligibility criteria, comparability of baseline characteristics, intention to treat analysis and use of point estimate and variability. The x axis is scaled to represent the proportion of component studies with either item of ‘yes’, ‘no’ or ‘unclear’.
Figure 3 shows the effect of PV on pulmonary and other adverse outcomes. The result showed that PV had a protective effect against the development of ALI as compared with the control group (27/507 vs 48/501), with an OR of 0.41 (95% CI 0.19 to 0.87). PV tended to be beneficial with regard to the development of pneumonia (14/400 vs 33/396; OR 0.46, 95% CI 0.16 to 1.28) and atelectasis (81/497 vs 101/492; OR 0.68, 95% CI 0.46 to 1.01), but statistical significance was not reached. Other adverse outcomes such as new onset arrhythmia were significantly reduced with the use of PV (82/473 vs 109/466; OR 0.47, 95% CI 0.48 to 0.93). Figure 4 shows the pooled effects of respiratory parameters. PV resulted in significantly increased oxygenation (WMD=17.79, 95% CI 7.99 to 27.60 mm Hg), but at the expense of carbon dioxide retention (WMD 2.87, 95% CI 2.25 to 3.49 mm Hg). Owing to significantly elevated PaCO2, arterial pH value was reduced in the PV group (WMD −0.02, 95% CI −0.03 to −0.02). However, the alveolar-arterial gradient was not significantly different between the two groups (WMD −20.39, 95% CI −45.32 to 4.55), most probably due to the limited number of studies being combined. With respect to other clinical outcomes, only the length of hospital stay could be marginally but statistically significantly shortened with the PV strategy (WMD −0.95, 95% CI −1.29 to −0.61 days). However, there was no evidence that PV could reduce the mortality, LOS in the ICU and the duration of MV (figure 5). A funnel plot was used to assess the publication bias. We arbitrarily selected two outcomes for this purpose (eg, ALI and PaCO2). The figure 6 shows some potential publication bias. Furthermore, Egger’s test showed p=0.006 for ALI and p=0.027 for PaCO2, both indicating significant bias.

Forest plots showing the effect of protective ventilation on outcomes of new onset acute lung injury (ALI), pneumonia, atelectasis and other adverse outcomes. The results show that protective ventilation is protective against new onset ALI (OR 0.41, 95% CI 0.19 to 0.87) and other adverse outcomes (OR 0.67, 95% CI 0.48 to 0.93). The protective ventilation tends to reduce the risk of pneumonia and atelectasis, but statistical significance is not reached.
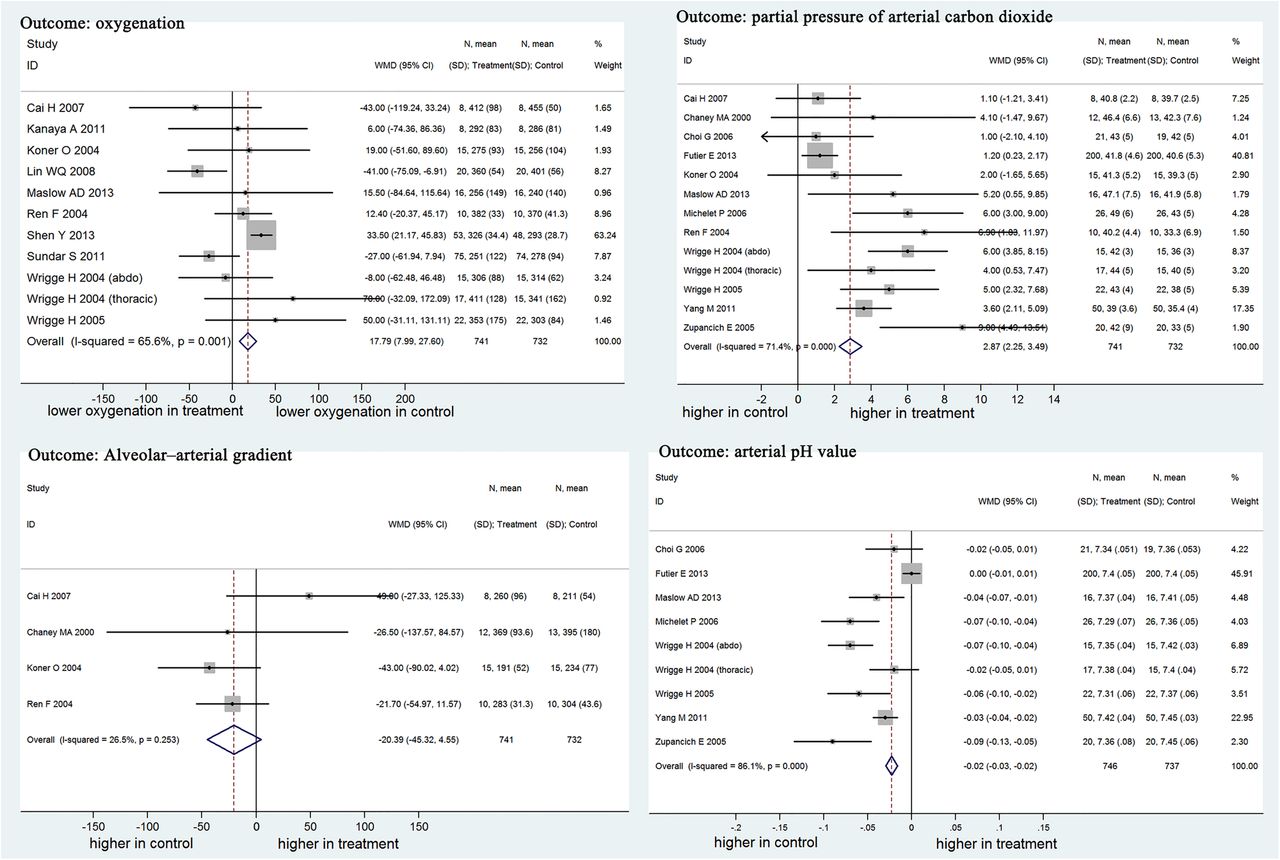
Comparison of respiratory parameters between treatment and control groups. Protective ventilation induces higher oxygenation as compared with the control group (weighted mean difference (WMD) 17.79 mm Hg, 95% CI 7.99 to 27.60 mm Hg), but it results in more carbon dioxide retention (WMD 2.87, 95% 2.25 to 3.49 mm Hg). Alveolar-arterial oxygen gradient is not significantly different between groups. Finally, a lower pH value is found in the protective ventilation group (WMD −0.02, 95% −0.03 to −0.02 mm Hg), which is consistent with the carbon dioxide retention.

Effect of protective ventilation on clinical outcomes. As shown in the figure, protective ventilation can significantly reduce the length of stay in hospital by 1 day as compared with conventional ventilation (weighted mean difference (WMD) −0.95, 95% CI −1.29 to −0.61 days). However, there is no evidence that protective ventilation can reduce the duration of mechanical ventilation, length of stay in the intensive care unit (ICU) and mortality rate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publication bias assessed by funnel plot. Publication bias was assessed using the effect sizes of OR of acute lung injury and weighted mean difference of carbon dioxide retention. The result showed that there was potential publication bias in the present analysis as represented by the asymmetrical appearance of both plots. Egger's tests were statistically significant for both parameters (p=0.006 and 0.027, respectively).
Bayesian approach
Bayesian approaches with random-effects and fixed-effects models were used to synthesise data. For the primary outcome ALI, both random-effects and fixed-effects Bayesian approaches obtained results (OR 0.40, 95% Crl 0.105–0.927 for a random-effects model; OR 0.49, 95% Crl 0.29–0.83 for a fixed-effects model) in agreement with that obtained by the classical method. For pneumonia, only the fixed-effects Bayesian approach showed a statistically significantly improved outcome with PV (OR 0.40, 95% Crl 0.21–0.74). The result of a random-effects Bayesian approach was in agreement with the classical approach. The three approaches arrived at the same result with respect to mortality. The interpretation of the results obtained by the Bayesian approach was more straightforward for subject matter audience. For instance, the result of ALI can be interpreted as follows: there is a 95% probability of the true OR being somewhere between 0.29 and 0.83.
Discussion
This systematic review shows that PV can protect against the development of ALI in patients who underwent major surgery, and the result remains robust by using the Bayesian approach. However, there is no evidence that PV can protect from the development of pneumonia and atelectasis in this group of patients. PV treatment is able to improve oxygenation, but at the expense of mild carbon dioxide retention. With respect to other clinical outcomes, there is a slightly shortened LOS in hospital.
The result that PV reduces the risk of postoperative ALI is in line with that reported by Serpa Neto et al.36 In Neto's study, there is a substantial number of observational studies that are subjective to more bias. We found that the largest observational study contributed more than half of the total population, and it reported a more beneficial effect of PV on ALI prevention than other smaller RCTs.9 With respect to mortality, while our study failed to identify any beneficial effect of PV, Neto's study found that it had a beneficial effect. However, the beneficial effect disappeared after excluding observational studies in sensitivity analysis, which was in agreement with our results. The same study group performed another individual patient data meta-analysis in this topic, and the result was consistent with our findings.37 However, the study included a smaller number of component studies than our study, probably due to the unavailability of individual patient data.
Atelectasis is an important complication of general anaesthesia in major surgery.38 Three underlying mechanisms have been proposed as contributors to the atelectasis: compression atelectasis, absorption atelectasis and loss of surfactant atelectasis.39 ,40 General anaesthesia can cause alterations in chest wall mechanics. With reduced wall motion during anaesthesia, atelectasis is likely to develop in the gravity-dependent region of the lung.41 Other factors contributing to atelectasis include a reluctance to cough after the operation, prolonged intraoperative recumbent position and postoperative diaphragm dysfunction. The use of perioperative PV may be potentially protective against atelectasis, and our systematic review was designed to test this hypothesis. However, we failed to identify any beneficial effect of the PV on postoperative atelectasis. In the result, there is a trend towards a more beneficial effect on the PV arm, but statistical significance was not reached at the predefined level of 0.05. This could be the result of the small sample size in component trials, and the lack of statistical power. The PROVHILO trial has recently been published and it recruited more homogeneous patients and had higher statistical power.42 However, this trial also failed to identify any beneficial effect of high PEEP ventilation on postoperative pulmonary complications. Probably, tidal volume plays a pivotal role in preventing pulmonary complications and the study did not vary tidal volumes between the intervention and control arms.43
Since PV primarily incorporates low tidal volume ventilation (figure 2), it is not surprising that it may result in carbon dioxide retention and ensuing hypercapnia. In our systematic review, PV was associated with significantly increased arterial PaCO2 (WMD 2.87, 95% CI 2.25 to 3.49 mm Hg) and reduction in pH value (WMD −0.02, 95% CI −0.03 to −0.02). However, this alteration is minimal as compared with the notion of ‘permissive hypercapnia’ used during PV for patients with ARDS. Since the effect of hypercapnia on clinical outcome is not harmful,44 PV induced minimal increase in PaCO2 retention is less likely to be harmful in patients who underwent general anaesthesia. Conversely, there are a few evidences supporting that hypercapnic acidosis is protective against tissue damage during inflammatory response.45–47 Another finding in the study is that PV had a beneficial effect on improving oxygenation. However, this may be of limited clinical significance because most patients who underwent elective general anaesthesia have preserved respiratory function. This is in contrast to the situation encountered in the management of patients with ARDS when hypoxaemia is the major clinical problem.
The strength of the systematic review is the incorporation of the Bayesian approach. It is common that trials included in meta-analysis are usually small in sample size, and the systematic review is not an exception. Small studies when combined with a classical approach are subject to the so-called small study effect.48 The classical approach to meta-analysis of trials is to assume that the summary statistics have a normal likelihood, which however may not hold true when a trial is small. The Bayesian approach overcomes this issue by providing a unified modelling framework.49 Fortunately, the sensitivity analysis shows that the Bayesian approach does not significantly alter the result obtained with the classical method. Furthermore, the median or mean value and associated credible interval obtained from posterior distribution obtained via iteration can be more directly interpreted. For instance, we obtained an OR of 0.41 (95% CI 0.19 to 0.87) for the risk of ALI. The common interpretation of this result is: there is a 95% probability of the true OR being somewhere between 0.19 and 0.87. However, this is a misunderstanding of the classic or frequentist approach and is actually the interpretation from the Bayesian perspective. The correct interpretation should be: if repeated samples were taken and the 95% CI computed for each sample, 95% of the intervals would contain the population mean. This rather convoluted language prohibits the probabilities that clinicians are seeking for. In this sense, the Bayesian approach provides a more comprehensible 95% credible interval for subject matter audience.50
In conclusion, the systematic review demonstrates that PV can reduce the risk of ALI development in patients who underwent major surgery. However, there is insufficient evidence that such beneficial effect can be translated to more clinically relevant outcomes such as mortality, LOS in the ICU or duration of MV. Owing to the significant number of observational studies being conducted in this field, further data synthesis can be performed by incorporating evidence from observational studies as the prior distribution. In this way, the importance of the prior information can be discounted by using a series of powers as we have already done in another study.51
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors BD conceived the idea and designed the study. ZZ performed statistical analysis and drafted the manuscript. LZ, LC and XZ (both Xia Zhang and Xiuqi Zhu) collected the data and helped with statistical analysis, and LC and XH helped to extract data and review the manuscript. CH helped in data acquisition and result interpretation during revision. BD and ZZ are identified as the guarantors of the paper, taking responsibility for the integrity of the work as a whole, from inception to published article.
Funding ZZ received a grant from the Science and Technology Research plan of Jinhua city (2012-3-031). CH received grants from the Zhejiang traditional Chinese medicine research project (Program: No. 2011ZZ001), the Zhejiang medical and health science and technology project (Program: NO.2013KYB004), and the Hall of Zhejiang province science and technology intensive medical technology innovation team research project (Program: No.2011R50018-02).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.8679n.