Article Text

Abstract
Objectives To determine the proportion of maternal and perinatal mortality and morbidity cases, identified by the Perinatal and Maternal Mortality Review Committee (PMMRC), that are also reported within the annual serious adverse events (SAEs) reports published by the Health Quality and Safety Commission (HQSC).
Setting Nationally collated data from the PMMRC and HQSC, New Zealand.
Participants Analysis of maternal and perinatal mortality and morbidity data 2009–2012.
Interventions Every SAE report published by the HQSC from 2009 to 2012 was scrutinised for maternal and perinatal cases using the case history provided by district health boards (DHB). Further detail of each case was requested from each DHB to establish whether they had been identified as maternal or perinatal mortalities or morbidities by the PMMRC.
Primary outcome measure The proportion of maternal and perinatal mortality and morbidity cases identified by HQSC SAE reports, compared with PMMRC reporting.
Results 58 maternal and perinatal SAEs were identified from the SAE reports 2009–2012. Of these, 50 fit under the PMMRC reporting definitions, all of which were also reported by the PMMRC. In the same time frame, the PMMRC captured 536 potentially avoidable maternal and perinatal mortalities and morbidities that fitted the HQSC SAE definition. Fewer than 9% of maternal and perinatal SAEs are captured by the HQSC SAE reporting process.
Conclusions The rate of maternal and perinatal adverse event reporting to the HQSC is low and not improving annually, compared with PMMRC reporting of eligible events. This is of concern as these events may not be adequately reviewed locally, and because the SAE report is considered a measure of quality by the DHBs and the HQSC. Currently, the reporting of SAEs to the HQSC cannot be considered a reliable way to monitor or improve the quality of maternity services provided in New Zealand.
- AUDIT
- OBSTETRICS
- NEONATOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The strengths of this study include its use of robust and accurate data on maternal and perinatal serious adverse events captured by the PMMRC, and the careful matching of cases with those reported by the HQSC SAE reports with the help of data from individual DHBs. This means the data presented are reliable.
The main limitation of the study is the analysis of data between two reporting bodies that claim to have different purposes and aims. However, the purpose of the HQSC SAE report is to provide transparency, and to improve the quality and safety of health and disability services, which may be compromised if only a fraction of cases are being reported.
Maternal and perinatal serious adverse events (SAE) are significantly under-reported by the Health Quality and Safety Commission (HQSC) annual report, when compared with those reported to the Perinatal and Maternal Mortality Review Committee (PMMRC).
Under-reporting of SAE to the HQSC suggests that cases are not undergoing adequate local review and that the report is not a useful way to monitor the quality, safety and experience of maternity services in New Zealand.
This paper highlights the need for the HQSC and PMMRC to work towards improving the recognition, reporting and review of SAE, and to prevent the duplication of reporting by healthcare staff.
Introduction
Since 2008, the Health Quality and Safety Commission (HQSC) has published an annual report on serious adverse events (SAEs; formerly known as serious and sentinel events).1 According to the HQSC, a SAE is defined as ‘‘one which has led to significant additional treatment, is life-threatening or has led to an unexpected death or major loss of function.’’2 It is recommended that district health boards (DHBs) review these events and report them to the HQSC, which publishes rates and case summaries on an annual basis.2 However, unlike the Perinatal and Maternal Mortality Review Committee (PMMRC), which is a statutory committee of the HQSC, where reporting is mandatory, reporting SAEs is voluntary and relies on local systems.
From 2006 to 2007, respectively, the PMMRC has reported on maternal and perinatal mortalities, and from 2010, the PMMRC has also reported on maternal morbidities, as defined by the Australasian Maternity Outcomes Surveillance System (AMOSS), and on cases of neonatal encephalopathy (NE; survivors and deaths).
The HQSC New Zealand was established to lead and coordinate work across the health and disability sector, for the purposes of monitoring and improving the quality and safety of health and disability services. The Commission works towards the New Zealand Triple Aim, which is improving the quality, safety and experience of care, improving health and equity for all populations, and providing better value for public health system resources.3
Since the inception of SAE reporting, the PMMRC has noted that maternal mortalities are infrequently reported to the HQSC, and, more recently, that NE cases are also rarely reported. The purpose of this study was to establish if all relevant maternal and perinatal SAEs reported to the HQSC were also captured and reported by the PMMRC, and vice versa. This information will help the PMMRC to establish whether it is achieving full case ascertainment, and what proportion of PMMRC cases fitting the SAE definition are being reported as SAEs.
Methods
The PMMRC reports both perinatal and maternal mortality and morbidity data. These data are the result of the collaborative efforts of the PMMRC, lead maternity carers, local coordinators and clinicians in each DHB, supported by a national coordination service, the Mortality Review Data Group of the University of Otago and the HQSC. The data are collected under section 59E of the New Zealand Public Health and Disability Act 2000.
Maternal death is defined as the death of a woman while pregnant or within 42 days of the termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.4
Perinatal-related deaths are deaths of babies from 20 weeks gestation (or if gestation is unknown a birth weight from 400 g) to 28 completed days of life.
The PMMRC has developed a system of reporting contributory factors, and potentially avoidable maternal and perinatal mortality. There are three domains of contributory factors: organisational and management factors, personnel factors and factors related to barriers to access and/or engagement with care. Each domain includes a checklist of items to be considered. A death is categorised as potentially avoidable if the absence of the contributory factors could have prevented the death.5
The PMMRC's reporting remit includes all perinatal and maternal mortalities, which the SAE reports would not be expected to capture. Therefore, we limited the mapping of PMMRC cases to those that had been identified by the PMMRC as potentially avoidable as they would fulfil the definition of a SAE as unexpected deaths. We excluded cases that the PMMRC identified as potentially avoidable secondary to barriers to accessing care as the only contributory factor.
NE is defined as ‘‘a clinically defined syndrome of disturbed neurological function within the first week of life in the term (≥37 weeks) infant, manifested by difficulty in initiating and maintaining respiration, depression of tone and reflexes, subnormal level of consciousness and often seizures.’’6 NE is associated with brain injury including cerebral palsy. Of those infants affected by NE, approximately one-quarter will die and an unknown proportion of the survivors will have long-term neurological complications (brain damage) resulting in chronic disability.5 ,7 Data are not currently available on whether surviving cases of NE were potentially avoidable, however, SAE reports record cases of NE, therefore all cases of NE have been included in our searches.
Maternal morbidity data collection also started in 2010 and has been conducted in collaboration with AMOSS. AMOSS is a national surveillance mechanism designed to study a variety of rare or serious conditions in pregnancy, childbirth and the postnatal period. The following are AMOSS notifiable conditions reported between 2009 and 2012: amniotic fluid embolism, antenatal pulmonary embolism, eclampsia (reported until September 2010), morbid obesity in pregnancy (reported until December 2010), placenta accreta, influenza in pregnancy requiring intensive care admission and peripartum hysterectomy (reported until December 2012).5 ,7 ,8 Of these conditions, only peripartum hysterectomy definitively fulfils the criteria for a SAE and has been included in searches.
The HQSC has several descriptions of a SAE. The National Reportable Events Policy describes an adverse event as an incident that results in harm to a consumer, which may include events defined as incidents, near misses and reportable events.9 The HQSC website describes a SAE as one that has led to significant additional treatment, is life-threatening or has led to an unexpected death or major loss of function.2 The SAE report states that ‘‘the precise definition of a SAE has often been difficult to pinpoint, as every case is different. However, some DHBs are reviewing their own threshold for reporting SAEs resulting in more incidents being classified as SAE.’’10 Health and disability service providers are required to establish each event's Severity Assessment Code (SAC), which is a numerical rating that defines the severity of an adverse event and, as a consequence, the expected level of reporting and investigation to be undertaken for the event.9 All health and disability service providers are expected to report adverse events that meet the criteria of SAC 1 and 2 within 15 working days from the date an event is reported to the provider using Part A of the Reportable Event Brief (REB).9 SAC 1 and 2 events are defined as those that have incurred either severe or major consequences to the patient with any likelihood of recurrence, or an event that has incurred moderate consequences with at least a moderate likelihood of recurrence.11 Part B of the REB is required within 70 working days of the event being initially reported to the provider, and includes a summary of the findings and recommendations related to the reportable event.
The reportable events are summarised and published annually as the SAE report. Each published report between 2009 and 2012 was searched for perinatal and maternal cases using the short case summary provided by the DHB. The PMMRC requested the National Health Index number and date of event for each case from the notifying DHB. Using this information, the PMMRC databases (perinatal, maternal, NE, AMOSS) were searched to establish whether these cases were also reported to PMMRC and, if they were perinatal or maternal deaths, whether they were potentially avoidable.
Results
From 2009 to 2012, a total of 58 perinatal and maternal SAE were reported. There were eight cases of maternal morbidity secondary to conditions that are not AMOSS reportable conditions (4 women with postpartum haemorrhage, 1 woman with fulminating hemolysis, elevated liver enzymes, low platelet count, 1 woman who suffered a medication error at caesarean section, 1 woman who suffered respiratory arrest and 1 woman with retained products of conception).
The remaining 50 SAE were reported by one of the PMMRC processes (figure 1).

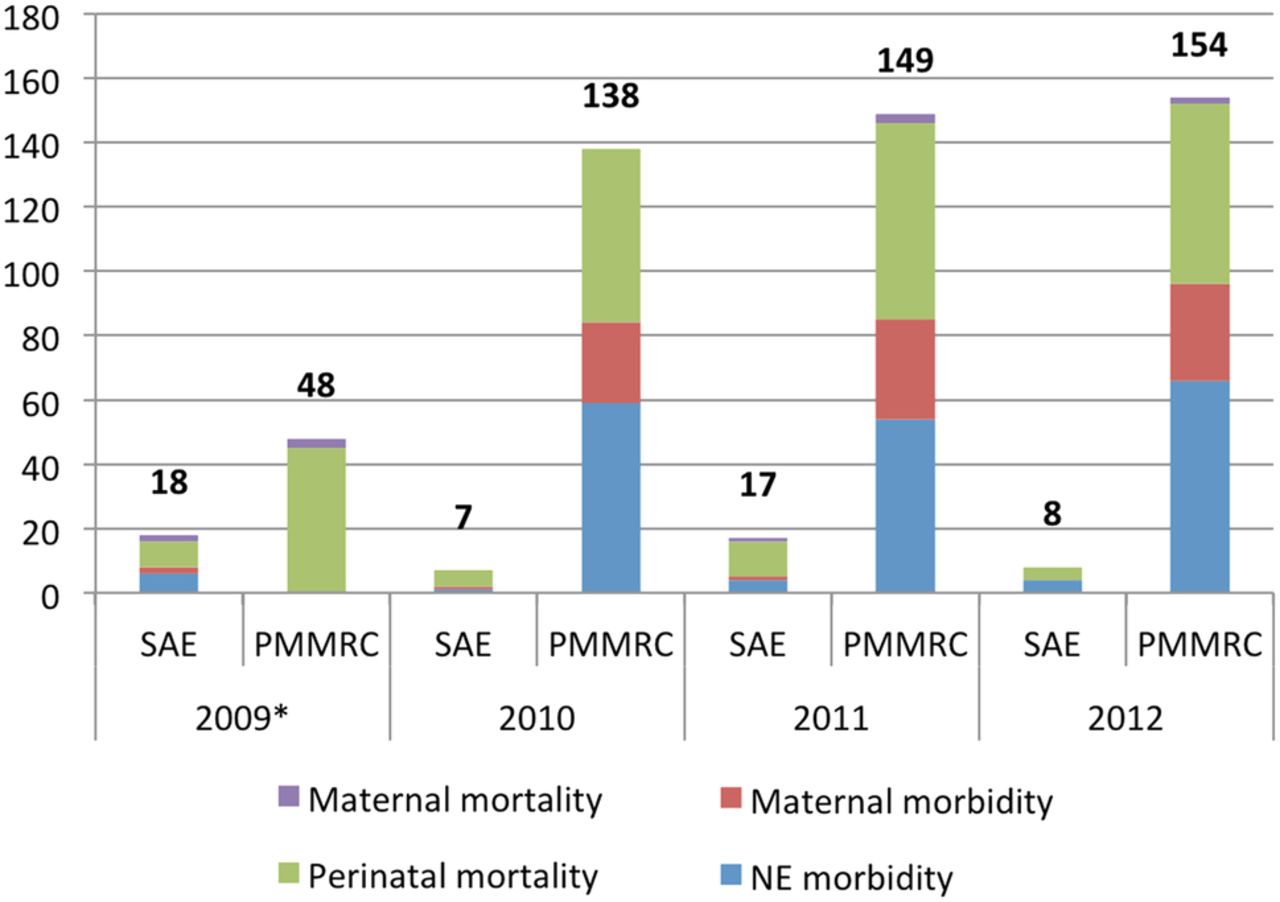{kind=link}
Maternal and perinatal morbidities and mortalities recorded by the PMMRC and SAE per annum. *The PMMRC started data collection on NE and maternal morbidity in 2010 (NE, Neonatal encephalopathy; PMMRC, Perinatal and Maternal Mortality Review Committee; SAE, serious adverse event).
Maternal deaths: There were three maternal deaths identified as having been reported as SAE: one by searching the SAE reports between 2009 and 2012 and two further maternal deaths were identified as having been reported as SAE from PMMRC data. We surmise that these two deaths were reported within the SAE report, but that it was not clearly stated that these were maternal deaths. In this time-frame, the PMMRC identified eight maternal deaths that occurred while the woman was an inpatient and were considered to be potentially avoidable with contributory organisation, management and/or personnel factors.
Maternal morbidity: There were four women with severe maternal morbidity (peripartum hysterectomy) who met the AMOSS notifiable conditions definition who were also reported in the SAE reports between 2009 and 2012. AMOSS started its collection of data on severe and rare disorders of pregnancy in 2010. Since then, 86 women who had a peripartum hysterectomy were reported by AMOSS.
Perinatal deaths: There were 28 perinatal deaths reported in the SAE reports between 2009 and 2012. Within the same time-frame, the PMMRC reported 216 deaths that were considered potentially avoidable with organisational, management and/or personnel contributory factors. Lack of protocols and guidelines were the major organisational factors, and failure to follow best practice was the most common personnel-related factor. Of the 28 perinatal deaths reported as SAE, 21 were reported in the PMMRC data as potentially avoidable perinatal deaths. The remaining seven were identified as deaths by the PMMRC but not determined to be potentially avoidable. The most common antecedent cause of death among potentially avoidable perinatal deaths reported by the PMMRC and perinatal deaths reported in the SAE reports, was hypoxic peripartum death, which occurred in 40 of 216 (18.5%) PMMRC reported cases and 11 of the 28 (39%) perinatal SAE reported cases. This was followed by ‘fetal growth restriction’ (15.7%) and ‘specific perinatal conditions’ (14.8%).
Neonatal encephalopathy: There were 15 infants with NE reported within the SAE reports from 2009 to 2012, all of whom survived the perinatal period. The PMMRC reported 227 infants with NE in the same time period, of whom 179 survived (table 1).
A summary of maternal and perinatal morbidities and mortalities reported as SAEs to the HQSC and to the PMMRC
Discussion
This report has compared maternal and perinatal SAEs reported to the HQSC with those reported to the PMMRC over the time period 2009–2012. The purposes of the PMMRC and HQSC SAE reporting differ. They are bodies with different aims and processes. However, despite their differences, they both hold the common goal of improving care.12 With this in mind, it is reassuring that the PMMRC has identified and reported all the maternal and perinatal cases within the SAE reports that fall under PMMRC and AMOSS reporting definitions.
There are, however, significant numbers of cases of maternal and perinatal mortality and morbidity that appear to fulfil the definition of SAE that have not been reported to the HQSC.
The purpose of the SAE reports is ‘‘to provide transparency, and improve the quality and safety of our health and disability services.’’1 ,13 The Commission's national reportable events policy sets out a process for ensuring that SAEs are reviewed appropriately by the provider organisation, and subsequently reported to the Commission.9 The latest report notes that comparing data between years is problematic because more events are being reported and reviewed each year. It also recommends that the data should not be used to measure safety because there is considerable variation in the rates of reporting as well as the provision of services and the size of the community that each DHB serves. The clinical lead for the commission has stated that ‘‘accurate information and analysis helps the health sector understand the extent and type of patient harm occurring.’’14
The WHO has published guidelines for implementing effective reporting systems, outlining its core concepts: to enhance patient safety by learning from failures, ensuring reports are handled in a non-punitive manner, that reporting is followed by a constructive response with feedback, and that there is a meaningful analysis and dissemination of lessons learnt with recommendations for changes.15 Despite this transparent approach, there remains a recognised problem with local and national incident reporting systems.16 These problems include fear of punitive action, poor safety culture in an organisation, lack of understanding among clinicians about what should be reported, and how the reports will ultimately impact on patient safety.16
It has been identified by a similar patient safety organisation in England and Wales, the National Reporting and Learning System, that organisations reporting low numbers of patient safety incidents are often reporting these events locally, but not nationally.17 Therefore, to overcome the same problem encountered by the process in New Zealand, the HQSC could work with the mortality review committees and the DHBs to consider how these organisations might share data submitted on severe adverse events to prevent duplication of reporting and utilise data reported to the HQSC for different purposes. Some statutory changes to the legislation would be necessary to allow the mortality committees to report their data to the HQSC Central Repository Group.
While local investigation and reflection on SAEs is to be commended, there may be perceived barriers to submitting reports, for example, time pressure, lack of perceived benefit, lack of recognition of an event as being a significant maternal morbidity, damage to the reputation of the organisation and duplication of reporting, all of which have been cited as strong disincentives to reporting adverse events in healthcare.18 Additionally, there may be a concern by healthcare workers about the potentially identifiable nature of case histories that are published in the report for each SAE. This is in contrast to the mandatory nature of reporting to the PMMRC, with corresponding statutory protection of information. The mandatory nature of reporting to the PMMRC may account for the differences in the two reports.
We recognise that the purpose of SAE reporting and PMMRC reporting differs. It is also important to recognise that low reporting of SAE does not necessarily mean that lessons are not being learnt and that positive changes are not being made locally. However, we have identified under-reporting of maternal and perinatal SAEs to the HQSC, which suggests that a significant number of these cases are not undergoing adequate local review and that the report is not a useful way to monitor the quality, safety and experience of maternity services in New Zealand.
Footnotes
Contributors CF conceived the idea for the paper. BK, VM and SA were responsible for the data gathering and extraction. SA wrote the initial draft, which was edited by LS, CF and VM.
Competing interests CF is the past Chair of the PMMRC. VM is the National Coordinator of the PMMRC. LS is the epidemiologist for the PMMRC.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Details of possible cases from published HQSC SAE reports were sent to the relevant DHB with a request that they provide National Health Index number and date of event.