Article Text

Abstract
Objective To evaluate the efficacy of a targeted screening for melanoma in high-risk patients following the receipt of a mailed invitation to an annual skin examination by a general practitioner (GP).
Methods A prospective cohort study was conducted in a primary care setting in western France. A total of 3897 patients at elevated risk of melanoma (identified using the Self-Assessment of Melanoma Risk Score) consented to participate in a targeted melanoma screening project in 2011. One year later, the participants were invited by mail to consult their GP for an annual skin examination. Efficacy of the procedure was evaluated according to patient participation and the number of melanomas detected. The consultation dates and results were collected during the 12 months postreminder and were analysed using SAS. Analyses of whether participation decreased compared with that during the year of inclusion and whether populations at risk for thick melanoma showed reduced participation in the screening were performed.
Results Of the 3745 patients who received the mailed invitation, 61% underwent a skin examination. The participation of patients at risk for thick melanoma (any patient over 60 years of age and men over 50 years of age) was significantly greater than that of the patients in the other subgroups (72.4% vs 49.6%, p<0.001; and 66% vs 52.4%, p<0.001, respectively). The patients referred to the dermatologist after 1 year were more compliant compared with those referred during the first year (68.8% vs 59.1%, p=0.003). Six melanomas were detected within 1 year postreminder; therefore, the incidence of melanoma in the study population was 160/100 000.
Conclusions This study confirms the benefits of developing a targeted screening strategy in primary care. In particular, after the annual reminder, patient participation and the diagnosis of melanoma remained high in the patients at elevated risk of thick melanomas.
Trial registration number NCT01610531.
- PREVENTIVE MEDICINE
- PRIMARY CARE
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study was conducted in a primary care setting.
The participants were patients at elevated risk of melanoma who were recruited using a validated and reproducible procedure based on the Self-Assessment of Melanoma Risk Score.
Six months after receiving an annual reminder to consult their general practitioner for a targeted screening for melanoma, 61% of the patients underwent a skin examination.
The participation of patients at risk for thick melanoma was significantly above average.
Six melanomas were detected. These results yielded a crude melanoma incidence of 160/100 000 in the cohort population and 469/100 000 in the men older than 50.
Introduction
In France, the incidence of melanoma is estimated at 10.8/100 000 for men and 11/100 000 for women.1 Overall, the incidence increased by 3.5 between 1980 and 2012.1 Since the lesions are visible, they should be detected at an early stage through skin examination. However, in 2012, melanoma was responsible for 1672 deaths in France.1 The main prognostic factor is the Breslow thickness (in millimetres) at the time of diagnosis.2 The 5-year survival rate of patients with localised melanoma is 98.1%, compared with only 16.1% for patients with metastatic melanoma.3 Despite these findings, routine screening by full skin examination is not recommended in France,4 the USA,5 Australia or New Zealand, although the latter has the highest incidence of this disease worldwide.6 ,7 Indeed, the efficacy of routine screening in decreasing the mortality rate for these patients has not been proven,5 and routine screening would be expensive to perform.8
Conducting targeted screenings based on the identification of high-risk participants could be a more valuable9 and cost-effective strategy.8 ,10 ,11 The following main risk factors for melanoma are well known:12–14 a personal or family history of melanoma, the presence of greater than 40 naevus, the presence of atypical naevus, skin phenotype I or II, freckles and actinic damage and a history of sunburns. Certain demographic groups have also been identified as being at higher risk of thick melanoma,9 ,15 including men, individuals over 60 years of age16 ,17 and men over 50 years of age.18 However, there is a need to define the best way to identify, screen and follow individuals at high risk of primary cutaneous melanoma.19
A low physician density has also been associated with the identification of thick melanomas.20–22 Melanomas tend to be thinner when they are detected by physicians rather than patients and also when they are detected during screening skin examination rather than during routine care.17 ,23–27 However, only 20% of patients who have had melanoma report that they previously consulted a dermatologist.28 Therefore, general practitioners (GPs) could play a significant role in the screening of these patients. One study has reported that the proportion of melanomas diagnosed by GPs in France increased from 24% in 2004 to 42% in 2008 following the implementation of a system requiring patients to register their attending physician.29
On the basis of these findings, our team has developed a targeted melanoma screening procedure grounded in primary care, using the Self-Assessment of Melanoma Risk Score (SAMScore). This score is based on a 7-item self-administered questionnaire (figure 1) that a patient can answer without specific medical knowledge (30–32) and allows for the selection of a population at high risk of melanoma during primary care consultations.30–33 The SAMScore algorithm allows for the expression of risk in a dichotomous format (either at elevated risk or not for melanoma; figure 1). According to the SAMScore, a patient is considered at elevated risk for melanoma if at least one of the following three criteria is met: (1) the presence of at least three risk factors among the following seven risk factors: phenotype I or II, a freckling tendency, >20 melanocytic naevus on both arms, experienced severe sunburn during the childhood or teenage years, resides in a country at low latitude, a history of previous melanoma and a history of melanoma in a first-degree relative; (2) under 60 years of age and >20 melanocytic naevus on both arms; and (3) 60 years of age or older with a freckling tendency. Previous research based on a literature review has suggested a relative risk of 13.77 in the selected high-risk population.31 ,32 The SAMScore has been used to create a cohort of patients at high risk of melanoma (COPARIME) who were then asked to participate in a pilot targeted screening for melanoma (NCT01610531).33 The targeted melanoma screening procedure comprised the following three steps: (1) identifying high-risk patients using the SAMScore; (2) asking GPs to perform a total skin examination on these high-risk patients; and (3) referring patients to a dermatologist if needed (for patients requiring a specialist opinion according to the GP). Between April and October 2011, 3917 patients were included, nine of whom had melanoma. The crude incidence observed during the first year of screening (229/100 000) highlighted the potential benefit of such a targeted screening.33

Questionnaire used for the Self-Assessment of Melanoma Risk Score.
However, the generalisability of the findings based on a 1-year intervention might be low. A major issue is the compliance of high-risk patients selected by the SAMScore who would be asked to consult yearly for melanoma screening and to consult a dermatologist in the case of a suspicious lesion.34 Specific attention should be paid to patients at high risk of thick melanoma (including men, individuals over 60 years of age and men over 50 years of age) because their concern for melanoma screening has been reported to be lower compared with other high-risk patients.16–18
Our team contacted all patients at risk of melanoma from the COPARIME cohort at 1 year after their inclusion in the targeted screening procedure. They received a mailed invitation to reconsult their GP for an annual skin examination. The aim of the study was to evaluate the efficacy of the mailed reminder, based on the following two variables: patient participation (with a specific focus on populations at risk of thick melanoma) and the number of melanomas detected.
Methods
Design of the study
This study was based on a prospective follow-up of the COPARIME cohort. The patients were initially enrolled between 11 April and 30 October 2011, by 78 GP volunteers in western France, specifically in the departments of Loire-Atlantique and Vendée. All dermatologists in both departments participated in the study. The dermatologist density is 5.3/100 000 inhabitants in Loire-Atlantique, a predominantly urban department, and 2.1/100 000 inhabitants in Vendée, a more rural department. These physician densities are comparable to those of other French departments (national mean: 5.3/100 000).35
Participants
The eligibility criteria to receive the reminder at 1 year were as follows: being at high risk for melanoma according to the SAMScore, having agreed to participate in the targeted melanoma screening 1 year earlier, being over 18, and having no personal history of melanoma. Twenty patients were excluded from the COPARIME database, including 9 who had developed melanoma during the year since initially participating and had been directly recommended for a dermatologist follow-up and 11 who had died. As a result, a total of 3897 patients were eligible (figure 2).
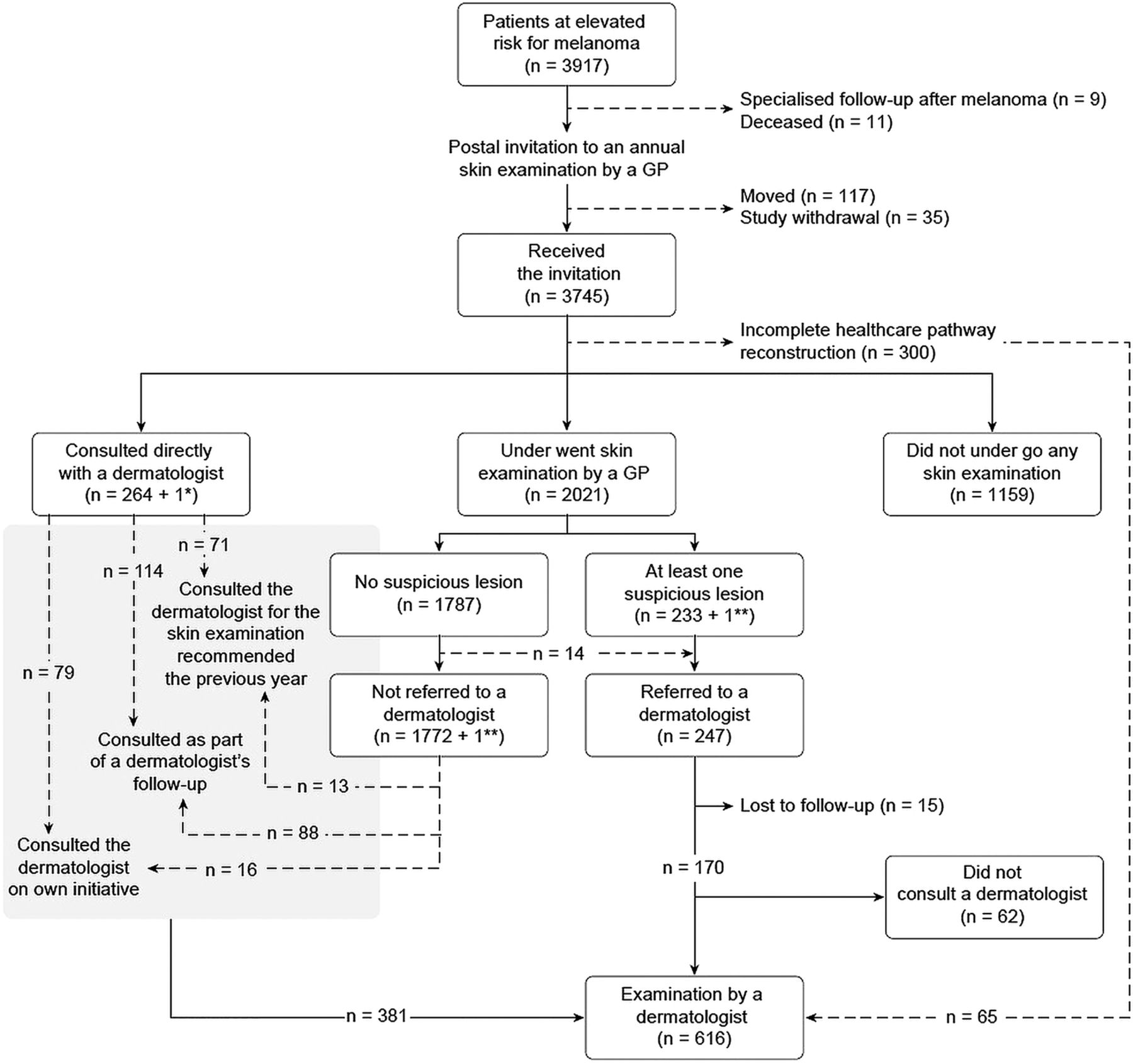
Participation among patients at elevated risk of melanoma at 6 months after a mailed reminder for an annual general practitioner skin examination.
Annual skin examination by a GP
An invitation to reconsult their GP for an annual skin examination was sent to eligible patients by mail at 1 year after their inclusion in the cohort.
The GP was asked to perform a total skin examination. Patients were referred to a dermatologist based on the opinion of the GP (as in routine care). The dermatologists were asked to classify their examinations of these referred patients according to the following three categories: ‘benign lesion’, ‘lesion to monitor’ and ‘indication for exeresis’. When exeresis was indicated, the last step was anatomopathological examination.
Data collection
In addition to sending a reminder to the patients, each GP was mailed a table summarising the following data to be collected for each patient: the date of skin examination, the identification or not of a suspicious lesion and whether the patient was referred to a dermatologist. An updated table was sent to the GPs at months 6 and 12. If data were missing at 1 year after sending the reminder, an investigator contacted the GP by telephone and offered to visit the medical practice to facilitate data collection.
One year after the reminder was mailed to the last patient in the cohort, each dermatologist was mailed a table summarising the data to be collected for each patient, including the date of the dermatological consultation and the conclusion derived from the skin examination, that is, ‘benign lesion’, ‘lesion to monitor’ or ‘indication for exeresis’. The anatomopathological result was also recorded when available. If data were missing, an investigator contacted the dermatologist by telephone and offered to visit the medical practice.
Between June and December 2013, all patients for whom no data were available were recontacted to determine whether they had consulted a dermatologist. All of the data collected during these telephone calls with patients were then confirmed or invalidated based on data from a physician (GP or dermatologist).
All of the data were recorded in an Access database.
Efficacy: patient participation and number of melanomas detected
Participation in the follow-up annual skin examination by the GP was assessed at 6 months after mailing the invitation.
Patient participation following the mailing of the invitation was analysed after the classification of the patients into the following six categories: (1) underwent the skin examination by the GP as expected; (2) directly consulted a dermatologist without reconsulting the GP, even though he/she had not consulted a dermatologist when his/her GP had referred him/her the previous year; (3) directly reconsulted his/her dermatologist as part of his/her dermatological follow-up; (4) directly reconsulted his/her dermatologist on his/her own initiative; (5) had no skin examination by his/her GP and no dermatological consultation; and (6) was referred to a dermatologist following examination by his/her GP but did not consult the dermatologist.
Melanoma cases were described using pathological reports.
Statistical analysis
Quantitative data are presented as the mean and median. Subgroup analysis was performed for the men, patients over 60 years of age, men over 50 years of age, and patients living in rural areas. Data from the first year were compared with data from the second year using the χ2 and Fisher's exact tests. The GP effect was tested using Fisher's variance ratio test. Statistical significance was set at 0.05. R 3.10.0 software was used.
Opinion of the ethics committee
The ethics committee of Tours University Hospital has given a favourable opinion on the performance of the study (n°2011-R2-BRD 10/11-N).
Results
Patient demographics
Of the 3897 patients, 117 moved without leaving a forwarding address, and 35 discontinued their participation in the study, leaving 3745 patients for integration into the analysis. The mean age of the patients was 44.5 (±15.6) years, and there were 1197 (32%) men. In total, 713 (19%) patients were over 60 years of age and 426 (11.3%) were men over 50 years of age. Finally, 2427 (64.8%) patients lived in Loire-Atlantique, 1206 (32.2%) in Vendée and 112 (3.25%) in other departments.
Patient participation
After the 1-year follow-up, 61% of the patients included in the targeted screening procedure reconsulted their GP, and 16% reconsulted a dermatologist (figure 3). A total of 17.1% of the cohort patients were lost to follow-up.

{kind=link}
{kind=link}
{kind=link}
Participation in skin examinations by general practitioners and dermatologists among patients at elevated risk of melanoma based on a 2-year follow-up.
Figure 2 shows the six methods of patient participation, analysed at 6 months after the invitation was mailed to reconsult. A total of 264 (7%) patients directly consulted a dermatologist, 2021 (54%) reconsulted their GP, and 1159 (31%) had no skin monitoring.
The proportion of referred patients who actually consulted a dermatologist increased after the reminder at 1 year compared with that on initial inclusion in the screening (68.8% vs 59.1%, p<0.001). However, the overall proportion of cohort patients who consulted a dermatologist was lower (15.8% vs 23.9%, p<0.001) because the proportion of patients referred to a dermatologist by the GPs was lower (12.2% vs 38.3%, p<0.001; table 1). The GP effect, tested as a random factor for the corresponding variables, was not significant (p=0.10 and p=0.32, respectively).
Patient participation in a pilot melanoma targeted screening after an annual mailed reminder
Melanoma cases
A total of 83 patients underwent exeresis, and 6 melanomas, 5 squamous cell carcinomas and 15 basal cell carcinomas were diagnosed. The characteristics of the six melanomas are provided in table 2. Of the six melanomas, five were identified among the patients initially referred by their GP. The incidence of melanoma standardised to the populations of both departments was 183.7/105 for men and 98.7/105 for women.
Characteristics of melanomas diagnosed during the 2-year follow-up of the COPARIME cohort
The median thickness of the melanomas detected during the second year was 0.405 mm (table 2). One melanoma was greater than 1 mm thick, which was identified in a patient who had not consulted a dermatologist after having been referred the first year.
In men over 50 years of age, the exeresis rate (21% vs 11.6%, p=0.029) and the number of malignant lesions identified after exeresis (66.7% vs 21.5%, p<0.001) were higher compared with the reference group (table 3). In patients over 60 years of age, the number of malignant lesions identified after exeresis (66.7% vs 19.4%, p<0.001) was higher compared with the reference group (table 3).
Malignant lesions and participation in populations at elevated risk of advanced melanoma
Discussion
Main results
Six months after receiving the annual reminder to schedule a total skin examination with their GP, 61% of the patients underwent a skin examination. Of them, 7.1% directly consulted a dermatologist. Of the patients who consulted their GP, 12.2% were referred to a specialist. The participation of populations at risk for thick melanoma was significantly above average. Six new melanomas were detected, corresponding to a crude incidence of 160/100 000.
Strengths and weaknesses
The strengths of this study are the size of the study population, the screening procedure initiated under primary care and under real care conditions, the use of a single validated and reproducible tool to detect high-risk participants, and the prospective follow-up of the cohort.
This study also has certain limitations, including the number of patients lost to follow-up, the inclusion bias (women and young participans were over-represented in the population) and the absence of data on the false-negative rate of the procedure. Female over-representation is usually found in skin screening programmes36–39 and more generally in cancer screening.40 ,41 This bias could also be related to the population seeking consultation in general practice, which is not entirely representative of the general population.33 ,42
Last but not least, this study was conducted in a French setting and involved GPs who were volunteers; thus, the generalisability of the findings should be considered with caution. The study design was grounded in a healthcare system in which GPs have a mission of regulating access to secondary care. This organisation has been implemented in a large majority of European countries.43 However, national specificities may affect the referral and management procedures. Other variations may also appear in relation to discrepancies in the use of dermoscopy.
Interpretation of the results and comparison with data from the literature
The 61% rate of participation in the annual skin examination is higher than the rates observed for other cancers in France, including 52.1% for mammography,44 34.3% for Hemoccult II45 and 58.7% for cervical smear.46 This good participation rate, observed after the 1-year reminder, is a significant result that indicates the success of the screening. Offering a targeted screening rather than a screening of the general population could be associated with better participation.
Six melanomas with a median Breslow thickness of 0.405 mm were diagnosed during the second year of follow-up, and only one melanoma was greater than 1 mm thick. Similarly, other authors have reported that screening procedures help to identify predominantly thin lesions with a median Breslow thickness of approximately 0.3 mm.32 ,47 ,48 The standardised incidence of melanoma in the high-risk population in this study was much higher than that which has been established in this geographic area (7.9 and 3.7 times higher for men and women, respectively). This increased incidence confirms that identifying patients at elevated risk of melanoma is relevant. This result is novel because most studies have only reported the benefit of a screening procedure immediately after the intervention. The observation of transient over-detection in these studies did not allow for an assessment of the benefit that would have been obtained if the screening procedure had been extended.32 ,33 ,49
The present study confirms the potential benefit of GP consultation. First, five of the six new melanoma cases were identified among patients referred by their GP. Second, the concentration effect related to GP consultation was increased. Indeed, the proportion of patients referred to a dermatologist by their GP decreased during the second year compared with the first year (12.2% vs 38.3%). This proportion is more consistent with previously published data that have revealed proportions of referred patients ranging from 7.4% to 26%.36 ,50–52 This evolution could be explained by the need for GPs to perform an initial dermatologist reference examination during the year of inclusion, whereas their role would subsequently be to ensure the absence of evolution of pre-existing lesions.
The benefit of the proposed screening seemed the highest in the populations at risk of thick melanoma. Men, participants over 60 years of age, and men over 50 years of age accounted for 32%, 19% and 11.3% of the cohort population, respectively, but they accounted for 50%, 50% and 33% of the melanoma patients, which is consistent with the findings of other authors.18 ,51 ,53 No very thick melanomas (>3 mm) were detected in our high-risk population over the course of 2 years. We were not able to conclude whether this result was due to the efficacy of the screening procedure or if it was simply related to the low incidence of thick melanomas in the population. The only melanoma greater than 1 mm was paradoxically detected during the second year: the corresponding patient had been referred to a dermatologist during the first year, but he did not consult the dermatologist until more than 1 year later. For this type of minimally compliant patient, our mailed reminder could have communicated to the patient that he or she was responsible for any appointment made. Thus, the benefits of a primary care-based targeted screening on the incidence of very thick melanomas could be due not only to the involvement of GPs trained in screening,52 but also to the impact of a simple annual reminder on minimally compliant patients.
Finally, 95 patients consulted a dermatologist on their own initiative, one of whom had a melanoma. This finding is consistent with the results of other studies showing that certain individuals participating in skin screening programmes appropriately pursue consultations on their own.36 ,49 ,54–57 In our study, it is likely that patients who were sensitised to their risk status and educated in skin self-examination by their GP directly consulted a dermatologist when they identified a suspicious lesion.
Practical implications and perspectives
In our study, we evaluated a generic procedure that addresses the reported limits of numerous national guidelines.19 The identification of high-risk individuals was based on a validated tool. We assessed a reproducible procedure for the clinical management of individuals defined as high risk, involving the mailing of a yearly invitation for a clinical skin examination performed by a GP.
More than half of the patients identified as being at risk for melanoma according to the SAMScore responded positively to our mailed reminder about scheduling an annual skin examination with their GP. The high melanoma incidence and low melanoma thickness identified in this study are both in favour of a targeted screening conducted in primary care.
Extending the follow-up of our cohort would allow for an assessment of the proportion of false negatives related to GP examinations. Other major issues that should be addressed include assessments of the follow-up pace to be proposed in this population and the related costs. The validation of a beneficial effect of this screening procedure on mortality will require a randomised study.
Acknowledgments
The authors wish to thank the French National Institute of Cancer for its financial support and the GPs for their participation in the COPARIME targeted melanoma screening project.
References
Footnotes
Contributors CR conceived the study, participated in its design and supervision and was responsible for the GP network and for drafting the manuscript. CG participated in the design of the study, was responsible for the data collection and helped to draft the manuscript. GQ participated in the design of the study, managed the pathological reports and helped to draft the manuscript. MD participated in the data collection and helped to draft the manuscript. AG performed the statistical analysis and helped to draft the manuscript. AK and BD participated in the design, of the study were responsible for the dermatologist network and provided administrative and technical support. J-MN participated in the design of the study, was responsible for statistical analysis and study supervision, and helped to draft the manuscript. All authors read and approved the final manuscript.
Funding This study was funded and supported by the French National Institute of Cancer (€206 000) (http://www.e-cancer.fr).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The ethics committee of the University Hospital of Tours approved this study (n° 2011-R2-BRD 10/11-N).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.