Article Text

Abstract
Objectives To investigate the clinical and cost-effectiveness of self-monitoring of coagulation status in people receiving long-term vitamin K antagonist therapy compared with standard clinic care.
Design Systematic review of current evidence and economic modelling.
Data sources Major electronic databases were searched up to May 2013. The economic model parameters were derived from the clinical effectiveness review, routine sources of cost data and advice from clinical experts.
Study eligibility criteria Randomised controlled trials (RCTs) comparing self-monitoring versus standard clinical care in people with different clinical conditions. Self-monitoring included both self-management (patients conducted the tests and adjusted their treatment according to an algorithm) and self-testing (patients conducted the tests, but received treatment recommendations from a clinician). Various point-of-care coagulometers were considered.
Results 26 RCTs (8763 participants) were included. Both self-management and self-testing were as safe as standard care in terms of major bleeding events (RR 1.08, 95% CI 0.81 to 1.45, p=0.690, and RR 0.99, 95% CI 0.80 to 1.23, p=0.92, respectively). Self-management was associated with fewer thromboembolic events (RR 0.51, 95% CI 0.37 to 0.69, p≤0.001) and with a borderline significant reduction in all-cause mortality (RR 0.68, 95% CI 0.46 to 1.01, p=0.06) than standard care. Self-testing resulted in a modest increase in time in therapeutic range compared with standard care (weighted mean difference, WMD 4.4%, 95% CI 1.71 to 7.18, p=0.02). Total health and social care costs over 10 years were £7324 with standard care and £7326 with self-monitoring (estimated quality adjusted life year, QALY gain was 0.028). Self-monitoring was found to have ∼80% probability of being cost-effective compared with standard care applying a ceiling willingness-to-pay threshold of £20 000 per QALY gained. Within the base case model, applying the pooled relative effect of thromboembolic events, self-management alone was highly cost-effective while self-testing was not.
Conclusions Self-monitoring appears to be a safe and cost-effective option.
Trial registration number PROSPERO CRD42013004944.
- CARDIOLOGY
- HEALTH ECONOMICS
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study is the most up-to-date evidence synthesis on this topic, with the largest number of included randomised controlled trials.
Clinical heterogeneity was observed among included trials.
The majority of the trials included participants with mixed clinical indications for anticoagulation therapy, which made it challenging to extrapolate the results to specific clinical populations.
The perspective of the economic modelling was that of the National Health Service (NHS) and personal social services, and did not capture any wider benefit.
Long-term outcomes data on self-management from larger cohorts of people with different clinical indications are needed.
Introduction
Approximately 2% of the population are prescribed long-term oral anticoagulant drugs for atrial fibrillation (AF),1–3 heart valve disease,4–6 or other conditions with high risk of thrombosis.7–9 Historically, treatment has been with vitamin K antagonist therapy, with dose-adjusted warfarin the most commonly used drug. Recently, new oral anticoagulants (NOACs) which do not require dose adjustment, such as dabigatran etexilate, rivaroxaban or apixaban, have been proposed as a possible alternative to warfarin for the treatment of AF.10 ,11 However, NOACs are unsuitable for people with artificial heart valves (AHF), people with liver or renal dysfunctions and those who are taking concurrent medication, which may react with this class of anticoagulants. For these people, warfarin remains the long-term treatment of choice. Furthermore, the lack of long-term evidence on these novel anticoagulants compared with vitamin K antagonists induces some caution in their wide prescription.10
Typically, dose adjustment of vitamin K antagonist therapy involves a blood test of clotting (international normalised ratio, INR) with dose titration to maintain this within a narrow therapeutic range (TTR).12 ,13 Underdosing of anticoagulation therapy increases the risk of thromboembolism, while overdosing increases the risk of bleeding events. Repeated and regular measurements of INR, with dose adjustment when necessary, are necessary to ensure safe and effective anticoagulation therapy.14
Monitoring of anticoagulant treatment can be delivered in a number of different ways. These include full service provision in specialist anticoagulation clinics, in physician offices or general practices (either with samples sent to a laboratory or with near-patient testing) or self-monitoring8 in which patients carry out their own tests at home using approved portable coagulometers, which test a finger-prick blood sample. Self-monitoring includes both self-management, in which patients conduct tests and adjust their treatment according to an algorithm; in self-testing, the patients conduct the tests, but obtain treatment recommendations from a clinician after sending them the results.
Several coagulometers are available, which have CE marketing authorisation and Food and Drug Administration (FDA) approval; these include the CoaguChek system (versions S and XS) (Roche Diagnostics, Basel, Switzerland), the INRatio2 PT/INR monitor, (Alere Inc., San Diego, California, USA) or the ProTime Microcoagulation system (International Technidyne Corporation, ITC—Nexus Dx, Edison, New Jersey, USA). Their precision and accuracy compared with conventional laboratory-based clinical testing have been reported in a number of studies in the literature.15–17
The increased use of oral anticoagulants has intensified pressure on healthcare resources.18 The use of point-of-care coagulometers for self-monitoring may avoid unnecessary visits to hospitals or clinics while permitting more frequent INR monitoring and timely adjustment of warfarin dosing to avoid adverse events.19 The evidence for the effectiveness of self-monitoring is limited20 and previously published economic evaluations have produced conflicting results.14 ,16 The aim of this study is to assess the current evidence on the clinical and cost-effectiveness of self-monitoring (self-testing and self-management) in people receiving long-term vitamin K antagonist therapy as an alternative to standard anticoagulation monitoring care. We focus mainly on the current generation of point-of-care devices (eg, CoaguChek XS), which utilised the most recent technology to minimise measurement inaccuracies.
Methods
Clinical effectiveness
The methods of the systematic review of clinical effectiveness were prespecified and detailed in a research protocol (http://guidance.nice.org.uk/DT/16/FinalProtocol/pdf/English), and reported according to standard guidelines.21–24
Identification of studies
We identified a relevant systematic review published in the Cochrane Library in 2010 by Garcia-Alamino et al,20 which included studies published up to 2007, and had similar objectives to those of this study. Thus, the literature searches for this study were run in May 2013 for the period ‘2007-to date’ to identify newly published reports. All randomised controlled trials (RCTs) included in the Garcia-Alamino et al’s20 review were obtained and included for full-text assessment. Major electronic databases such as MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, EMBASE, Biosis, Science Citation Index, and Cochrane Controlled Trials Register (CENTRAL) were searched for relevant primary studies. Evidence syntheses’ reports, conference abstracts (2011–2013), and ongoing studies were sourced from relevant databases. Reference lists of included studies were perused for additional publications and experts in the field contacted for further information on relevant outcomes and ongoing research in the field. Searches were restricted to publications in English. Full details of the search strategies are presented in online supplementary appendix 1.
Inclusion and exclusion criteria
We included RCTs comparing self-testing and/or self-management of anticoagulation control using point-of-care coagulometers with standard monitoring care, which consisted of INR monitoring managed by healthcare professionals. We included studies of both adults and children with heart valve disease (eg, AHV), AF or other clinical indications who required long-term vitamin K antagonist therapy. Main outcomes of interest were: (1) major bleeding and thromboembolic events; (2) all-cause mortality; (3) anticoagulation control measured as time and INR values in TTR, and other intermediate outcomes (including frequency of testing, frequency of visits to clinics, patient compliance with testing).
Study selection and data extraction
Two authors independently screened the results of the literature searches, retrieved full-text copies of selected studies and extracted relevant data (PS, MC). Information on study design, characteristics of participants, settings, characteristics of interventions and comparators, and outcome measures was recorded for all included studies. The Cochrane Risk of Bias tool was used to assess the risk of bias in the included studies.22 Critical assessments of selection, detection, attrition and reporting biases were performed initially by one author (PS) and cross-checked by a second author (MC). Studies were not excluded purely on the basis of their potential risk of bias. Any uncertainty or disagreements during the study selection, data extraction and risk of bias assessment was resolved by discussion or arbitration by a third author (MB).
Data analysis
Where appropriate, pooled summary estimates were calculated using Review Manager, software (Review Manager V.5.2, Copenhagen: the Nordic Cochrane Centre, The Cochrane Collaboration, 2012). In the presence of either clinical or statistical heterogeneity, a random effects model was chosen as the preferred method for pooling the effect sizes.21 Relative risk (RR) together with 95% CIs were calculated for dichotomous data (Mantel-Haenszel method), while weighted mean difference (WMD) together with 95% CI were calculated for continuous data (inverse-variance method). Where SDs were not given, these were extrapolated, if possible, using test statistics. Heterogeneity across studies was explored by means of the χ2 statistic (with significance level at p<0.05) and the extent of inconsistency between studies quantified by means of the I2 statistic. For trials that had multiple arms contributing to different subgroups, the control group was subdivided into two groups to avoid a unit of analysis error.
Cost-effectiveness analysis
A de novo Markov model was developed25 ,26 in TreeAge Pro (TreeAge Software, Williamstown, Massachusetts, 2013) to assess the cost-effectiveness of self-monitoring (self-testing and self-management). The model structure was based on previous economic models of INR self-monitoring published in the literature,14 ,27–34 including models assessing the cost-effectiveness of NOAC drugs compared with warfarin in people with AF.11 ,35 In addition, an unpublished economic model was provided by Roche Diagnostics, the manufacturer of the CoaguChek XS coagulometer (J Craig, York Health Economics Consortium, 2013). The model was built and analysed in accordance with the National Institute for Health and Care Excellence (NICE) reference case for the evaluation of diagnostic tests and devices.36
Model framework and method of synthesis
The model was populated using data derived from the systematic review of clinical effectiveness, other relevant reviews to inform key parameters (eg, baseline risks), and routine sources of cost data,37 ,38 and information provided by clinical experts. The alternative monitoring pathways were embedded in a Markov model simulating the occurrence of adverse events over time for a hypothetical cohort of people with AF or AHV (figure 1). The model incorporated the pathways of care that individuals currently follow under standard practice in the National Health Services (NHS)—standard monitoring in primary care or in secondary care—as well as proposed pathways for self-testing and self-management. The cost-effectiveness of self-monitoring was assessed as a whole assuming a 50:50 split between self-testing and self-management. The model simulated transitions between the discrete health states on a quarterly (3-month) cycle. Appropriate costs and quality of life weights were attached to modelled events and health states, allowing cumulative health and social care costs and quality adjusted life years (QALYs) to be modelled over time. Full details of the modelling methods are provided in online supplementary appendix 2. The main assumptions made for the base case analysis are summarised in table 1. For the purpose of this study, it was assumed that self-monitoring patients use the CoaguChek XS system.
Main assumptions made for the base case analysis and justification

Schematic of the model structure.
The results of the model are presented in terms of a cost-utility analysis (ie, costs for and number of QALYs generated by each monitoring strategy). Self-monitoring strategies were compared to standard care monitoring, to estimate the incremental costs per QALY gained. Both costs and benefits (QALYs) were discounted at a rate of 3.5% per annum, in line with the NICE reference case.36 Cost are expressed in 2011/2012 Stirling. The model was initially analysed over a 10-year period, but the impact of adopting longer time horizons was explored through sensitivity analyses. Further sensitivity analyses focused on the standard care comparator (primary care, secondary care), the proportional split between the active interventions (self-testing, self-management), the baseline risk of thromboembolic events and the RRs associated with self-testing and self-management. In addition, cost-minimisation scenarios were considered (assuming an equal number of tests with self-monitoring and standard care, and equivalence in effects). Finally, the results of probabilistic sensitivity analyses were used to express the parameter uncertainty surrounding the base estimates of cost-effectiveness.
Results
Clinical effectiveness
Of the 658 records retrieved, 26 RCTs published in 45 papers with a total of 8763 participants met the inclusion criteria. Of the 26 included RCTs, 21 trials with a total of 8394 participants provided suitable data for statistical analyses relevant to the comparisons and outcomes of interest. A flow diagram outlining the selection process is shown in online supplementary appendix 3.
The 26 included trials were conducted in Europe and North America. Seventeen trials (17/26) compared self-management with standard care,39–55 six assessed self-testing,56–61 and one evaluated both self-testing and self-management versus either trained or untrained routine care (four arms).62 The remaining two trials compared self-testing with self-management,63 ,64 one of which focused exclusively on children.63 Two trials enrolled exclusively participants with AF,55 ,59 six trials limited inclusion to participants with AHV41 ,45 ,46 ,50 ,52 ,56 and 18 trials39 ,40 ,42–44 ,47–49 ,51 ,53 ,54 ,57 ,58 ,60–64 included participants with mixed clinical indications. The majority of the included trials (22/26) used the CoaguChek system for INR monitoring. Two trials used either INRatio or the CoaguChek S for INR measurement (but did not present results according to the type of the point-of-care device used),44 ,56 while the other two trials used the ProTime system.53 ,60
Table 2 summarises the characteristics of the included trials (full details are shown in online supplementary appendix 4 table S1). The included trials varied in size (16–2922 participants), the length of study duration (3.5–57 months), the age of the included adult participants (16–91 years) and the type of standard care (63.6% of the participants measured INR in secondary care, 27.2% in primary care and 9.2% in mixed care setting). In approximately 95% of the included participants, mean age was between 50 and 70 years. Nine trials, which includes 75% of the total participants, had study duration of more than or equal to 12 months.41 ,43 ,46 ,47 ,50–52 ,60 ,63 Three trials recruited participants who were new to anticoagulation therapy,46 ,48 ,51 two trials included participants receiving anticoagulants for the past 1–2 months,53 ,61 12 trials recruited participants who had been on anticoagulants for at least 3 months before randomisation39 ,40 ,42 ,43 ,47 ,54 ,57–59 ,62–64 while the remaining trials did not provide this information.
Summary of the characteristics of included trials
Only four trials were assessed to have adequate sequence generation, concealed allocation and blinded outcome assessment and therefore were judged at low risk of bias.47 ,61 ,63 ,65 The remaining trials were judged at ‘unclear’40–46 ,48–50 ,52 ,56 ,58 ,59 ,62 ,64 or ‘high’39 ,53–55 ,57 ,60 risk of bias (figure 2) (full details of the risk of bias assessment are presented in online supplementary appendix 4 table S2).
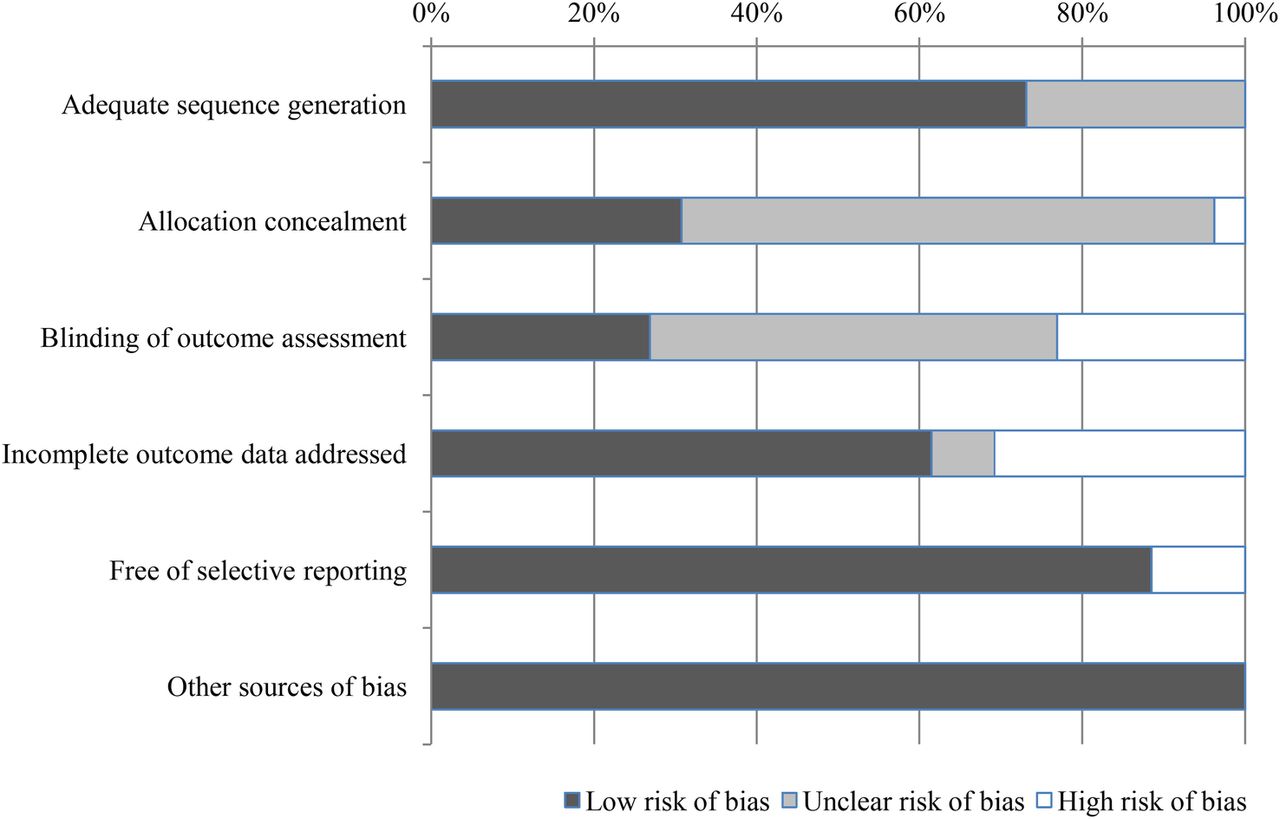
Summary of risk of bias of all included studies.
Major clinical outcomes
Major bleeding and major thromboembolic events were reported in the majority of trials. Definitions varied between the trials and not all trials used well-defined criteria. In general, major events (bleeding or thromboembolic) were defined as complications requiring hospital admission or medical assessment. Fatal bleeding and thromboembolic events were counted as deaths.
Table 3 shows the main findings of self-monitoring (self-testing and self-management) compared with standard clinical monitoring.
Meta-analyses results of major clinical outcomes and time in therapeutic range
Bleeding events
Twenty-one trials reported a total of 1472 bleeding events (major and minor). No statistically significant differences were observed between either self-management or self-testing, and standard monitoring care for major bleeding events (RR 1.08, 95% CI 0.81 to 1.45, p=0.60 and RR 0.99, 95% CI 0.80 to 1.23, p=0.92, respectively) (figure 3 and table 3). Self-testing was associated with a small increased risk of minor bleeding events (RR 1.23, 95% CI 1.06 to 1.42, p=0.005) and all bleeding events (RR 1.15, 95% CI 1.03 to 1.28, p=0.02) while self-management was not (the RR for minor bleeding events was 0.84, 95% CI 0.53 to 1.35, p=0.47 and for all bleeding events 0.94, 95% CI 0.68 to 1.30, p=0.69).

Forest plot of comparison: major bleeding events.
No statistically significant subgroup differences were found for bleeding events by clinical indication for anticoagulant treatment (AHV only, AF only or mixed) or by the setting for standard care (anticoagulant clinics only, physician/GP offices only, or mixed practices).
Thromboembolic events
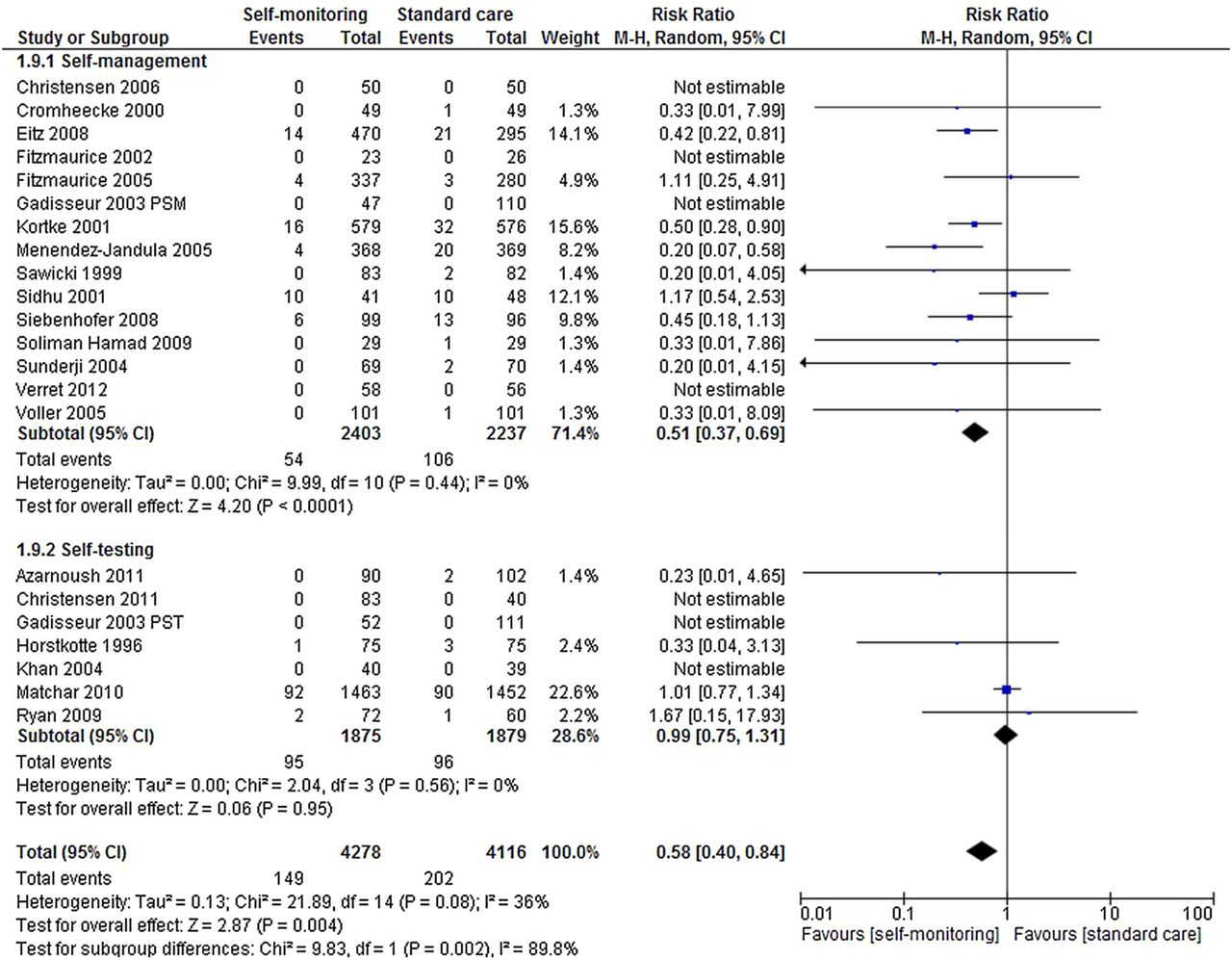
Twenty-one trials reported a total of 351 thromboembolic events (major and minor) involving 8394 participants.39–43 ,45–57 ,59–62 Self-monitoring was associated with a statistically significant reduction in the risk of thromboembolic events (RR 0.58, 95% CI 0.40 to 0.84, p=0.004) compared with standard care (figure 4). This reduction was still apparent when the analysis was restricted to major thromboembolic events (RR 0.52, 95% CI 0.34 to 0.80, p=0.003). The reduction in thromboembolic events was observed only in studies of patients carrying out self-management (RR 0.51, 95% CI 0.37 to 0.69, p<0.0001). There was no significant risk reduction among trials of self-testing (RR 0.99, 95% CI 0.75 to 1.31, p=0.56).

Forest plot of comparison: thromboembolic events.
The observed reduction in thromboembolic events was similar across clinical indications for anticoagulation: AHV (6 studies, RR 0.56, 95% CI 0.38 to 0.82), AF (2 studies, RR 0.33, 95% CI 0.01 to 8.09) and mixed indications (13 studies, RR 0.57, 95% CI 0.30 to 1.09) (test for subgroup differences: p=0.95). Similarly, there were no significant differences in observed reduction in thromboembolic events among studies which conducted standard care in anticoagulant clinics (10 studies, RR 0.65, 95% CI 0.30 to 1.42), physician/GP offices (6 studies RR 0.45, 95% CI 0.31 to 1.38) or mixed practices (5 studies, RR 0.66, 95% CI 0.31 to 1.38) (test for subgroup differences: p=0.55).
Mortality
Thirteen trials reported 422 deaths from any cause in a total of 6537 participants.39 ,42 ,43 ,46 ,47 ,49–52 ,54 ,56 ,57 ,60 There was no statistically significant difference in all-cause mortality between self-monitoring and standard clinical monitoring (RR 0.83, 95% CI 0.63 to 1.10, p=0.20) (figure 5). Trials of self-management found a reduction in mortality which was close to statistical significance (RR 0.68, 95% CI 0.46 to 1.01, p=0.06), and similar in size and direction to the observed reduction in thromboembolic events. Self-testing had no effect on mortality (RR 0.97 95% CI 0.78 to 1.19, p=0.74).

Forest plot of comparison: mortality.
There was an apparent significant reduction in mortality in trials which restricted entry to patients with AHV (4 trials, RR 0.54, 95% CI 0.32 to 0.92, p=0.02) and no reduction in mortality in trials with mixed clinical indications for anticoagulant therapy (RR 0.95, 95% CI 0.78 to 1.16, p=0.61). As none of the trials reporting mortality specifically excluded patients with AHVs, we could not conclude from the pooled data whether this difference by indication was clinically meaningful.
Deaths directly associated with anticoagulation therapy were reported in five trials.42 ,43 ,47 ,50 ,51 In total, six deaths related to anticoagulation therapy occurred among participants receiving usual monitoring care42 ,50 ,51 (1 valve thrombosis, 2 myocardial infarctions, 1 retroperitoneal haemorrhage, 1 cerebral haemorrhage, and 1 gastrointestinal bleeding) and seven deaths occurred among participants who self-managed their coagulation status (1 valve thrombosis, 1 pulmonary embolism, 1 massive ischaemic stroke, 2 myocardial infarctions, 1 cerebral haemorrhage, and 1 gastrointestinal bleeding).43 ,47
Anticoagulation control: target range
Table 4 summarises the results of anticoagulation control reported in the included studies. There was a great variation between trials in the measures used to assess INR time and the values in TTR. In general, INR time and INR values in TTR were reported to be higher among self-monitoring participants compared with those in standard care (table 4). Pooling of INR values in TTR across trials proved unfeasible. Eighteen trials38 ,39 ,42 ,43 ,47 ,48 ,50 ,51 ,53–57 ,59–64 provided data on INR time in TTR and pooling of results was possible for 10 trials that provided suitable data.42 ,43 ,47 ,53 ,54 ,56 ,57 ,59 ,60 ,62 No statistically significant differences were observed between self-management and standard care with regard to TTR (p=0.62) (table 3 and figure 6). Nevertheless, a modest but significantly higher proportion of TTR was found for participants who self-tested compared with those who received standard care (WMD 4.44, p=0.001) (table 3 and figure 6).
INR time and value in therapeutic range

Forest plot of comparison: time in therapeutic range.
The other intermediate outcomes were sparsely reported in the included studies. Two trials reported good patient compliance with self-monitoring (75% and 98%, respectively).58 ,59
Cost effectiveness
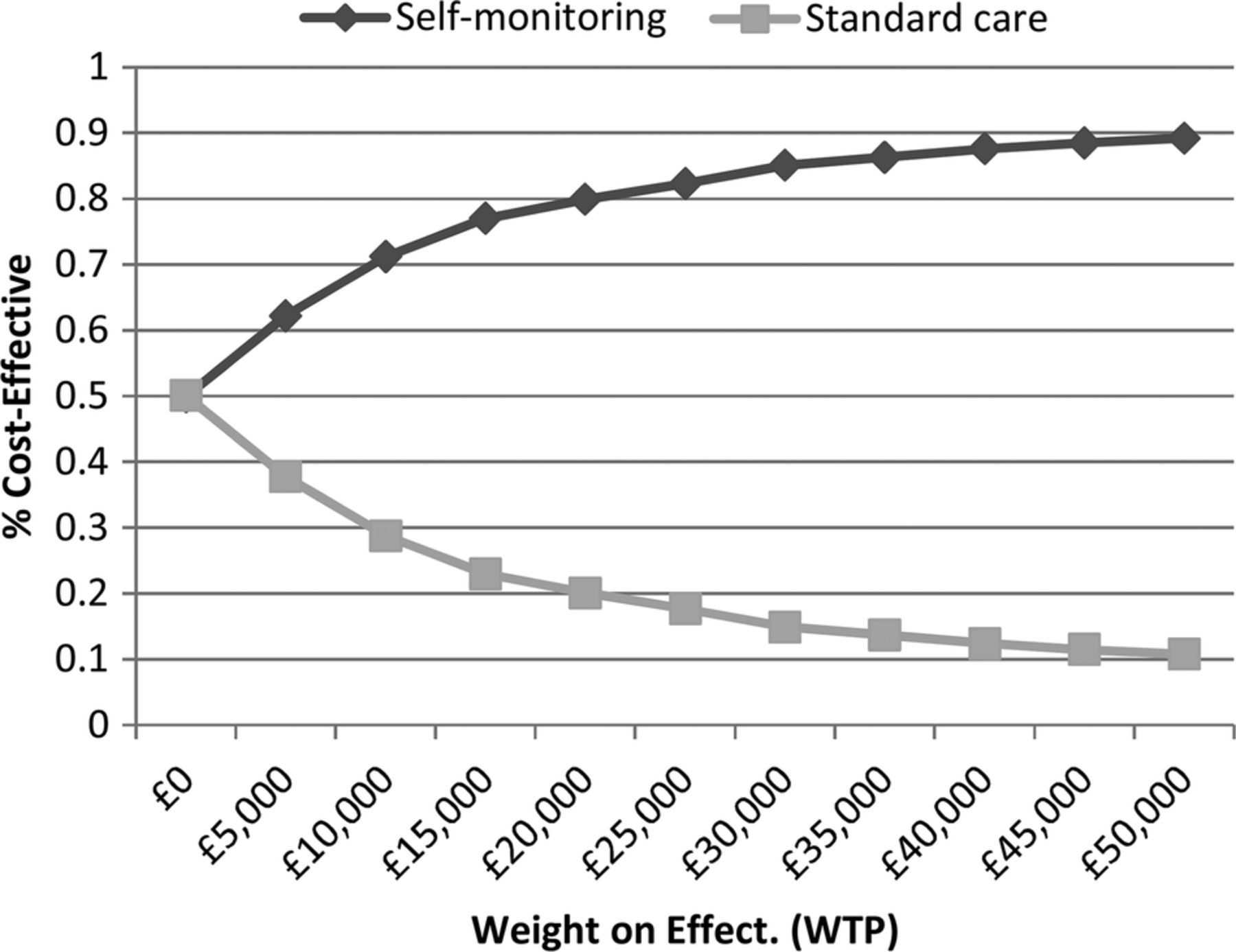
Applying the base case assumptions presented in table 1, the results of the cost-effectiveness analyses indicate that over a 10-year period, the introduction of self-monitoring would reduce the proportion of people suffering a thromboembolic event by 2.5%, while slightly increasing the proportion suffering a major haemorrhagic event by 1.2% (table 5). While the predicted monitoring costs are higher with self-monitoring, the total health and social care costs are similar: £7324 for standard care monitoring and £7326 for self-monitoring (table 5). The estimated QALY gain associated with self-monitoring was 0.028. Self-monitoring (50% self-testing, 50% self-management) appears to be cost-effective due to its positive impact on the incidence of thromboembolic events, even though, compared with mixed primary/secondary care, it is likely to increase the INR monitoring costs. Figure 7 shows that self-monitoring as a whole has an approximately 80% chance of being considered cost-effective at a willingness to pay ratio of £20 000 per QALY gained. However, the pooled relative effect estimate for self-testing on thromboembolic events (figure 4) is small and non-significant (RR 0.99), while the effect estimate for self-management is large (RR 0.51) and significant. Thus, within the base case model, self-management alone is highly cost-effective (ie, dominant), while self-testing is not (table 5).
Mean costs, outcomes and incremental cost-effectiveness over a 10-year time-horizon

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curves: self-monitoring versus standard care.
Further analysis of uncertainty
In an alternative specification of the model, the overall pooled effect estimates obtained from all self-testing and self-management trials were applied to the self-testing and self-management strategies. Under this scenario, self-monitoring as a whole was found to be cost-saving over standard care (see online supplementary appendix 5 table S3).
Two key parameters underpinning the cost-effectiveness findings are the baseline risk of thromboembolic events, and the relative effect of self-monitoring on these events. The model findings were robust to individual changes in these parameters through feasible ranges. However, when a lower baseline risk of thromboembolic events (1.15%) was combined with the upper 95% confidence limit for the RA associated self-management (RR 0.69), the incremental cost-effectiveness ratio (ICER) for self-monitoring as a whole rose above £30 000 per QALY. The same was found when the lower baseline risk of thromboembolic events was coupled with the upper confidence limit of the pooled RA for self-monitoring (RR 0.89). It should be noted, however, that self-management alone remained cost-saving under the former combined scenario. The cost-effectiveness of self-monitoring improved further when the modelled time horizon was extended to 20 and 30 years, dominating standard primary/secondary care based monitoring. The incremental cost per QALY gained for self-monitoring also remained below £20 000 when higher training failure and discontinuation rates were applied, and when higher self-monitoring testing frequencies were applied (with no change in effects).
Alternative scenarios assessed the potential for self-monitoring to be cost-saving if used to replace clinic-based testing without increasing the frequency of testing (see online supplementary appendix 5 table S4). Under these scenarios it was assumed that there would be no effect on the number of thromboembolic or bleeding events, and a cost-minimisation approach was adopted. This showed that, when holding all other base case parameters constant, self-testing and self-management were more costly than standard primary care monitoring (ie, physician offices and general practices), but less costly than standard secondary care monitoring (ie, specialised anticoagulation clinics).
Discussion
Our findings suggest that self-monitoring of anticoagulation at home is at least as safe and effective as standard clinic monitoring. Self-management of anticoagulation is associated with reductions in thromboembolic events and possibly, in all-cause mortality. INR time in TTR was reported to be higher in self-monitoring participants compared with standard clinical care. Self-monitoring, and in particular self-management, of anticoagulation status appeared cost-effective at a willingness to pay threshold of £20 000 per QALY gained when pooled estimates of clinical effectiveness were applied to the economic model. The modelled reduction in thromboembolic events was the key driver of cost-effectiveness.
The differences we observed between self-management and self-testing are difficult to explain. Paradoxically, those who self-tested, rather than self-managed, spent more time in TTR (and had more minor bleeding events), but those who self-managed experienced less thromboembolic events. It is possible that people who self-managed their coagulation status take a more active role in managing their therapy or that self-testing leads to more rapid or frequent dose changes. It is also worth noting that the meta-analyses results on self-testing were dominated by the results of the largest trial published so far, the Home International Normalised Ratio Study (THINRS),60 which enrolled 2922 people and assessed self-testing versus routine clinical care. This trial had a specialised routine coagulation control and the longest follow-up period (mean 3 years). The high quality of the routine care in the THINRS may exceed current monitoring care for anticoagulation control and could explain the lack of significant differences in major clinical adverse events between self-testing and routine care. When we excluded this trial from the statistical analyses, the risk ratio for thromboembolic events fell from 0.99 to 0.55 among self-testing participants, although the CIs widened (95% CI 0.13 to 2.31).
On the whole, our findings are broadly consistent with those of previously published systematic reviews on self-monitoring using point-of-care devices for the management of anticoagulation therapy, which found that self-monitoring was associated with a significant reduction in the occurrence of thromboembolic events and all-cause-mortality.14 ,16 ,20 ,27 ,29 ,66–69 Our economic model, in accordance with previous economic evaluations,29 ,34 indicates that self-monitoring is likely to be cost-effective. The findings of our economic model are also broadly in line with those of previous UK-based economic assessments, in that self-monitoring (under base assumptions) will increase the monitoring costs to the NHS. However, our base case differs from that of previous UK evaluations in that the pooled relative effects for self-management and self-testing, compared with standard care, were applied. We observed significant future cost savings and quality of life gains as a consequence of a significant reduction in the incidence of thromboembolic events. This, in turn, translated into more favourable estimates of cost-effectiveness. Further differences between the current analysis and the previous UK-based model include the application of higher standard secondary care monitoring costs, lower self-monitoring device costs (in line with current prices), and higher acute treatment costs for stroke and major bleeding events. Our analyses suggest that the cost-effectiveness of self-monitoring is robust to variations in these parameters when pooled clinical effect estimates are applied to the model.
In more general terms, home monitoring, and especially self-management, of anticoagulation therapy may have a substantial impact on the quality of life of patients and their families. It may reduce the anxiety associated with the fear of deviating from the therapeutic target range and boost confidence in the therapy, increase independence and psychological well-being, and allow for the more efficient organisation of time (eg, travelling, social interactions).
Limitations
This study has been conducted as per recommended methodological standards and is the most up-to-date evidence synthesis on this topic with the largest number of included RCTs.20 ,66 ,68
There are, however, potential limitations. The literature searches were performed in 2013 and were not subsequently updated. While the meta-analysis results demonstrated low statistical heterogeneity, which made it statistically reasonable to combine the studies, uncertainties remain that clinical heterogeneity could have contributed to over or underestimate the effects. The included trials varied in terms of clinical indications for anticoagulation therapy, type of control care, reporting structure for the time and/or values in TTR, the mode and structure of the preintervention training and education programme, length of follow-up, and methodological study quality. The majority of the trials included participants with mixed clinical indications for anticoagulation therapy, which made it challenging to extrapolate the results to specific clinical populations. In particular, only limited data were available for people with AF and consequently, no firm conclusions could be drawn in relation to this patient population is. Nevertheless, it likely that self-monitoring may produce similar clinical benefits in people with AF to those achieved in people with artificial heart valves. A great variation between trials was found in the way both INR time and INR values in TTR were measured, which hampered further analyses.
Assuming there is no interaction between the TTR and the relative treatment effect for self-management on thromboembolic events, our modelling suggests that it will remain cost-effective even where TTR is high and the thromboembolic event rate is low. However, it is possible that the quality of standard care may modify the effectiveness of self-monitoring, and in turn, influence its cost-effectiveness. Where patients are already achieving a very high level of INR control, this may limit the potential for self-monitoring to improve TRR and in turn, reduce thromboembolic event. With regard to the economic model, there is still a certain degree of uncertainty surrounding the pooled clinical effectiveness estimates, especially for self-testing. It is worth noting that the perspective of the cost-effectiveness analysis was that of the National Health Service (NHS) and personal social services. Therefore, our modelling fails to capture any wider benefits or cost-savings to patients and their families, such as a reduction in time spent travelling to and waiting in clinics.
Generally, adherence to self-monitoring was reported to be high in the included trials (more than 90%). However, all included trials enrolled highly selected samples of people requiring anticoagulation therapy, and so it was uncertain whether there was strong external validity. To be enrolled in the trials, participants needed to demonstrate adequate cognitive and physical abilities, as well as dexterity and confidence in using the point-of-care device. In some of the included trials42 ,43 ,47 ,62 a considerable proportion of eligible participants (up to 50%) ultimately were not considered suitable for inclusion. Despite the enrolment restrictions, results are valid for the patients groups included, which actually represent the population who would be considered for self-monitoring in clinical practices. Six of the trials were conducted in the UK and we could not find any evidence that the UK trial patient cohorts were fundamentally different from those of the rest of the included studies.
Whilst new non-vitamin K antagonist oral anticoagulants were beyond the scope of this assessment, these offer an alternative option for many people with AF who are currently on warfarin. However, these are not suitable for all people who need anticoagulation therapy. Furthermore, due to the potential risk of bleeding, it is unlikely that people receiving warfarin who have stable INR may switch to the NOACs. Therefore, there are still many people who receive warfarin rather than the NOACs for whom self-monitoring is still of clinical relevance.
Conclusions
Self-monitoring, and in particular self-management, is a safe and cost-effective option for people requiring long-term vitamin K antagonist therapy. Further research assessing the longer-term outcomes of self-management versus standard monitoring care as well as the comparative effectiveness of various point-of-care coagulometers would be useful. The technology related to these devices is constantly changing and future research needs to target larger cohorts of people with different clinical indications requiring long-term anticoagulation therapy. It is worth acknowledging that the modern point-of-care coagulometers are likely to have advanced both in their ease of use and cost, which, in theory, could modify the possible candidates for these devices as well as the magnitude of any economic evaluation.
Acknowledgments
The authors would like to thank the investigators who kindly provided additional trials details, the NICE Assessment Subgroup specialist members (Dianna Oxley, Dianne Kitchen, Niall O'Keeffe, Peter Birtles, Peter MacCallum, Rishabh Prasad, and Sue Rhodes) for their assistance with some queries related to the interventions and their use in clinical practice, Charles Boachie for statistical support, and Lara Kemp for secretarial support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors MB and CRR conceived the original idea for the study, interpreted results, edited the manuscript and took full responsibility for the integrity and accuracy of the work; PS contributed to literature evaluation and data collection, conducted statistical analyses, and drafted the first version of the manuscript; GS contributed to the design and development of the economic evaluation and edited the manuscript; MC contributed to literature evaluation and data collection, and edited the manuscript; ET contributed to the development of the economic model and edited the manuscript; CF conducted literature searches and edited the manuscript; CB and BC interpreted results and edited the manuscript. All authors have read and approved the final version of the manuscript. Thus, all authors fulfil the ICMJE criteria for authorship: (1) substantial contributions to conception and design, acquisition of data or analysis, and interpretation of data; (2) drafting the article or revising it critically for important intellectual content, and (3) final approval of the version to be published.
Funding This report was commissioned by the NIHR HTA Programme as project number 13/06/2001. The Health Services Research Unit, and Health Economics Research Unit, Institute of Applied Health Sciences, University of Aberdeen, are both core-funded by the Chief Scientist Office of the Scottish Government Health Directorates. The views expressed in this report are those of the authors and not necessarily those of the Chief Scientist Office of the Scottish Government Health Directorates, NIHR HTA Programme or the Department of Health. Any errors are the responsibility of the authors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendices are available from the corresponding author.