Article Text

Abstract
Objectives There is a scarcity of literature reporting hospital costs for treating out of hospital cardiac arrest (OOHCA) survivors, especially within the UK. This is essential for assessment of cost-effectiveness of interventions necessary to allow just allocation of resources within the National Health Service. We set out primarily to calculate costs stratified against hospital survival and neurological outcomes. Secondarily, we estimated cost effectiveness based on estimates of survival and utility from previous studies to calculate costs per quality adjusted life year (QALY).
Setting We performed a single centre (London) retrospective review of in-hospital costs of patients admitted to the intensive care unit (ICU) following return of spontaneous circulation (ROSC) after OOHCA over 18 months from January 2011 (following widespread introduction of targeted temperature management and primary percutaneous intervention).
Participants Of 69 successive patients admitted over an 18-month period, survival and cerebral performance category (CPC) outcomes were obtained from review of databases and clinical notes. The Trust finance department supplied ICU and hospital costs using the Payment by Results UK system.
Results Of those patients with ROSC admitted to ICU, survival to hospital discharge (any CPC) was 33/69 (48%) with 26/33 survivors in CPC 1–2 at hospital discharge. Cost per survivor to hospital discharge (including total cost of survivors and non-survivors) was £50 000, cost per CPC 1–2 survivor was £65 000. Cost and length of stay of CPC 1–2 patients was considerably lower than CPC 3–4 patients. The majority of the costs (69%) related to intensive care. Estimated cost per CPC 1–2 survivor per QALY was £16 000.
Conclusions The costs of in-hospital patient care for ICU admissions following ROSC after OOHCA are considerable but within a reasonable threshold when assessed from a QALY perspective.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
First study looking at outcome related costs in this population.
Single centre study though population in study representative of typical patients presenting to any Heart Attack Centre in the UK.
Tariff based re-imbursement system used to eliminate interhospital variability in accounting methods.
Methodology unique to UK tariff-based system though all cost analyses susceptible to country of origin healthcare funding system bias.
Figures quoted current and applicable to current commissioning and therefore of interest to wider readership.
Background
Out of hospital cardiac arrest (OOHCA) causes 60 000 deaths in the UK and 300 000 deaths in the USA each year.1–3 Only 7–10% of patients who suffer an OOHCA in the developed world will survive to hospital discharge and obvious cognitive impairment will occur in 10% of these survivors.1–3 Studies have demonstrated improved high-quality survival (Cerebral Performance Category (CPC) 1–2) using targeted temperature management (TTM) and primary percutaneous intervention (PPCI);4–9 guidelines now incorporate these interventions.10 In these selected trial populations approximately 50% of patients with return of spontaneous circulation (ROSC) admitted to intensive care unit (ICU) are discharged from hospital with a good neurological outcome.4–7 This compares to 20–30% prior to the introduction of TTM and universal PPCI.9 ,11
Outcome analysis of interventions used in cardiac arrest management has a number of unique challenges. The overall outcomes are frequently poor—as represented by death or survival with poor neurological outcome and disability. Furthermore, it is often impossible to determine prognosis for several days after admission to hospital as patients are kept sedated for temperature management. Primary coronary interventions and prolonged periods of intensive care (with associated investigations) are delivered before any assessment of neurological damage or prognosis is possible. The inevitable consequence of this is that expensive treatment is delivered to people whose outcome remains uncertain. There is accordingly much interest in identifying robust early predictors of poor prognosis following OOHCA.12 ,13 In order to make a useful assessment of cost-effectiveness, the unit hospital costs of treatment leading to the discharge of a high-quality survivor must include costs associated with unsuccessful treatment, that is, death or severe disability in others. Interventions delivered early in the patient pathway may clearly have a major impact on accumulated costs—especially if there is a possibility of delaying inevitable death in the intensive in-hospital phase.
Literature review reveals a scarcity of published data regarding economic costs of OOHCA, particularly within the UK.14–18 The primary purpose of this study was to provide an up-to-date UK estimate of the in-hospital cost per high-quality OOHCA survivor, based on CPC scoring, within a tertiary referral centre following the introduction of PPCI and TTM in accordance with guidelines.10 Secondarily, using follow-up outcome data from similar studies, an exploratory estimation was made to determine likely cost-effectiveness based on cost per QALY gained.
Methods
This study was a service evaluation under current National Research Ethics Service definitions and used retrospective data collected for clinical and administrative purposes.19
Data collection
We performed a single centre retrospective review of all patients admitted to our ICU following successful resuscitation from OOHCA over an 18-month period starting 1 January 2011. In keeping with prevailing guidelines, patients were assessed for PPCI suitability and targeted temperature management was initiated unless contraindicated.
A good outcome was defined by a Pittsburgh Cerebral Performance Category (CPC) Score of 1–2 (independence, mild impairment). A poor outcome was defined as death or CPC 3–4 (moderate to severe impairment, coma).20 CPC score breakdown is shown in table 1.
Cerebral Performance Category Scale20
Patients were identified from London Ambulance Service (LAS) records and from a specific coding parameter on the ICU electronic patient administration database (AcuBase Critical IV, AcuBase Ltd, UK). LAS records also provided details of the cardiac arrest. Demographic data, diagnostic data, cardiac interventions, organ support data, outcome and length of stay data were extracted from paper and electronic patient records. Electronic radiology databases (Centricity, GE Systems) supplied data on diagnostic radiological interventions. Data were entered onto a new database for analysis (Excel, Microsoft). CPC scoring was determined from routine clinical, physiotherapy and occupational therapy assessments recorded in the clinical notes for each patient. These were assessed by two of the authors. Where disagreement occurred, the best score was accepted. In practice, this rarely occurred and did not occur between CPC 2 and 3.
Cost analysis
‘Costs’ were defined as the sum of money apportioned to episodes of care as generated using the UK payment by results (PbR) system, as outlined in figure 1.21 These costs were provided at an individual patient level by the Trust Finance Department.

Payment by Results System Cost Calculation.21
After discharge, clinical coders translate clinical records into diagnostic and procedure codes using the ‘International Statistical Classification of Diseases and Related Health Problems’ (ICD-10) and the ‘Office for Population Census and Surveys Classification of Interventions and Procedures’ (OPCS-4) systems, respectively.22 These codes are submitted to the Secondary Users Service (SUS); the SUS is a nationally determined computerised algorithm which generates a Health Resource Group (HRG) descriptor based on the submitted codes. Health Resource Groups typically reflect diagnoses and interventions that commonly occur together. Each HRG corresponds to a nationally set tariff, which is adjusted annually. Such adjustments are derived from benchmarking data submitted by National Health Service (NHS) Trusts across the UK. There is currently no HRG for OOHCA. HRGs commonly assigned to these patients include those associated with PPCI, or implantable cardioverter defibrillator (ICD) implantation (see table 2 eg, HRG codes and online supplementary appendix for worked patient examples). Each HRG tariff is adjusted according to whether the in-patient stay was elective or non-elective and will include a standard set number of days for inpatient care up to a point known as the ‘trimpoint’. Days in excess of this trimpoint are charged on a daily rate. Since costs vary according to geography (eg, inner city vs rural), a local Market Forces Factor (MFF) is included as a multiplier. In our Trust an MFF of 1.2417 is applied to reflect higher local costs.
Examples of coronary intervention PbR tariffs for year 2011–2012
Some aspects of inpatient care are not included within the HRG—Critical Care is such an example. The adult Critical Care Minimum Dataset (CCMDS) is a subset of data relating to the patient's Critical Care stay that generates a separate Critical Care HRG. The Critical Care HRG is based on the peak number of organs supported at any time during that Critical Care episode; PbR tariffs at our trust for 2011–2012 are shown in table 3. Each admission to Critical Care will generate a separate Critical Care HRG that would be expected to reflect:
Hotel services
Nursing and other clinical staff
Therapies
Medical staff
Ward consumables
Drugs
Blood and blood products
Diagnostics undertaken while the patient is in critical care, for example, pathology, plain film X-rays, MRIs
Medical and surgical equipment (include the costs of specialist equipment, eg, CPAP and NIPPY machines, and ensure that the costs of devices excluded from the national tariff are also reported in the reconciliation statement workbook).23
Imperial College Healthcare NHS Trust ICU PbR tariffs for year 2011–2012 shown against NHS reference costs for that year
Certain medical devices and expensive treatments, including ICDs are also charged separately to the HRG. In our Trust the cost of each unit is calculated as an average of all such devices implanted over the previous year, thus eliminating the complexities of charging for individual devices according to manufacturer; the average ICD cost was £18 285 per unit in 2011–2012.
Data analysis
Data were assessed for normality using the d'Agostino-Pearson omnibus test; all cost and length-of-stay data were non-parametric and are presented as median (IQR) values, rounded to the nearest £1000 and whole day, respectively. Non-parametric data were analysed using a Mann-Whitney U test. Correlation was assessed using a Pearson's R Correlation test. Data were analysed and presented using Microsoft Excel and Prism (V.5, GraphPad Software, San Diego, California, USA).
Quality adjusted life years extrapolation
As a secondary analysis we extrapolated cost per quality adjusted life years (QALY) for our data. QALYs are calculated by multiplying the number of additional years gained by the ‘utility’ (an assessment of the quality of those years).24 In the absence of long-term follow-up data for our 2011–2012 patient population we extrapolated QALY data using survival and utility from previous follow-up studies. Historically studies have been consistent in their reported long-term mean survival post-OOHCA (6.13 years (Norwegian 1971–1992 data)14 and 6.2 years (Scottish 1991–1998 data)15). Studies have also reported consistent utility following survival after OOHCA, 0.72 in a 2004 American study,25 0.7 in a Dutch study26 and 0.77 in a recent German study.16 In order to avoid underestimating cost/QALY we used conservative estimates extrapolated from these studies of 6 years mean survival and 0.7 utility.
Results
The flow of OOHCA patients through our hospital in the 18-month period from 1 January 2011 is shown in figure 2. One hundred and fifty-seven patients presented directly to our hospital following OOHCA. Of these patients, 56 required ICU admission. One hundred and one patients were not admitted to ICU; of these, 37 survived to hospital discharge, having required ward care only and 64 either died soon after admission to hospital or were deemed to have such a poor prognosis that critical care was not indicated. None of these 101 patients were included in this study.
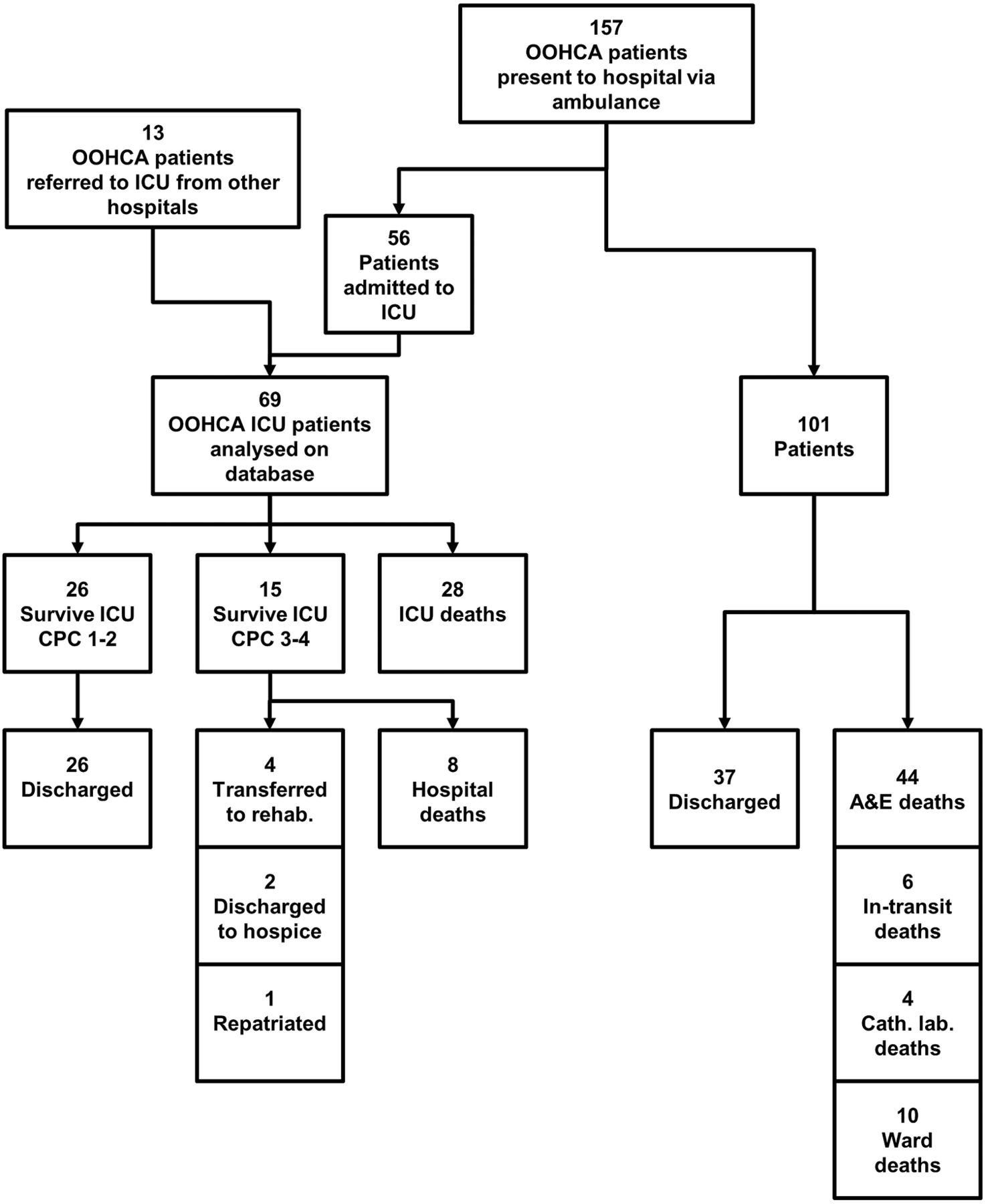
Presentation of OOHCA patients to our regional centre. Flow of patients presenting with OOHCA to our hospital. A total of 157 patients were brought by ambulance to our institution. Fifty-six of these were admitted to intensive care unit (ICU) and 101 were not admitted to ICU. A further 13 patients were admitted to our ICU following OOHCA presenting to another hospital (total 69 patients). Of the ICU patients 33 survived to hospital discharge, 28 died (21 on ICU, 7 on the ward subsequently). Of the 101 OOHCA not admitted to ICU at our institution 37 were discharged from hospital alive, 64 died. Of these 44 died in A&E, 6 died in the theatre/recovery area (prior to transfer to definitive ICU bed), 4 died in the catheter laboratory and 10 died on the wards.
On account of our position as a regional referral centre for cardiac intervention, 13 additional patients were transferred from other hospitals thus making at total of 69 patients admitted to our ICU following successful resuscitation from OOHCA in the 18 months. During this time period our ICU admitted 666 patients; OOHCA patients thus represented 10% of all ICU admissions. Baseline characteristics, cardiac interventions, causes of cardiac arrest and critical care support of the 69 patients is summarised in table 4. Over the course of their admission, these patients underwent a total of 598 chest radiographs, 87 CT scans (all sites but mostly brain) and 9 MRI scans (brain and cardiac). Six patients had an automatic ICD (AICD) inserted prior to discharge.
Patient characteristics, causes, cardiac and ICU interventions
Outcomes
The outcomes of the 69 ICU patients are shown in table 5. Of 69 ICU patients, 26 survived to hospital discharge with a CPC 1–2; 7 survived to hospital discharge with a CPC 3–4; the overall hospital survival rate was 47.8%. All patients discharged from ICU with a CPC 1–2 survived to hospital discharge and returned to their own homes (2 via inpatient rehabilitation). Two returned overseas and were lost to follow-up. Five of the 26 patients (19%) are known to have died in the first year after discharge.
ICU and hospital survival and discharge destination stratified by outcome
Although 15 patients in total left ICU with a CPC 3–4, eight died in hospital and thus only seven patients left hospital alive. None had improved their CPC score by hospital discharge and none returned directly to their own homes. Four patients went to long-term rehabilitation institutes, two to hospices and one was repatriated to a hospital outside our region. Four of these patients died within the year and thus 3 of 15 remained alive at 1 year.
Cost analysis
Total costs
The total ICU cost for the 68 UK patients (1 overseas patient was excluded) was £1 166 000. The total number of ICU days was 696. Thus cost per ICU day was £1700 (£1 166 000/696). The total hospital cost of the 68 UK patients was £1 699 000, with total number of hospital days of 1653 and cost per undifferentiated hospital day £1000 (£1 698 000/1653). The total non-ICU costs were £533 000, with total number of non-ICU days 957 and the cost per non-ICU hospital day £557 (£533 000/957). Intensive care costs represented 69% of the total costs and for each patient was a mean of 66% of their individual cost.
Cost analysis and outcome
Costs and length of stay are shown stratifies by outcome in tables 6 and 7. The average (median) cost of a CPC 1–2 patient hospital (ICU+non-ICU) stay was significantly (p<0.005) lower at £29 000 than that of a CPC 3–4 patient (£53 000) as shown in figure 3. The length of stay was significantly longer in CPC 3–4 patients (p<0.005). There was also a significant correlation between length of stay and cost with much longer length of stay in ICU and hospital for the CPC 3–4 patients (0.9795 (p<0.0001) and 0.6193 (p<0.0001) respectively; see figure 4). While the average overall hospital cost per patient admitted to ICU was £20 000 (this includes non-survivors), the overall hospital cost per survivor of any CPC was £51 000 (£1 698 000/33). The total hospital cost per high-quality survivor (defined as CPC 1–2) was £65 000 (£1 698 000/26). Thus a major determinant of cost for the CPC 1–2 group was the burden of cost of the non-survivors and CPC 3–4 patient group. Taking into account the deaths of five patients in the year following hospital discharge the cost per CPC 1–2 1-year survivor was £81 000 (£1 698 000/21).
Costs (ICU and total) stratified by outcome
Length of stay (ICU and total) to nearest day, stratified by outcome

Graph demonstrating costs (median, 25th and 75th centiles and minimum and maximum values) both for ICU (light grey) and total (ICU and non-ICU) stay in hospital (dark grey) for different outcome groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph demonstrating length of stay (median, 25th and 75th centiles and minimum and maximum values) both for ICU (light grey) and total (ICU and non-ICU) stay in hospital (dark grey) for different outcome groups.
QALY analysis
QALY data were extrapolated using survival and utility from previous studies (see Methods). Using a conservative estimate for survival following OOHCA of 6 years, the life year cost per high-quality survivor is estimated to be £11 000 (£65 000/6) and using a conservative utility estimate of 0.7, cost per QALY of a high-quality survivor is £16 000 (£11 000/0.7).
Discussion
To our knowledge this is the first UK study using individual case costing to assess the economic burden of OOHCA in patients requiring intensive care. This may be reflective of the specific challenges of completing such a cost analysis within the UK. A fully ‘bottom-up’ approach summing individual pathology, radiology, staffing, drugs, cardiology and hotel services costs per patient is extremely challenging as these figures are embedded within the HRG costing. We have used the best of the data available to us—re-imbursements calculated by the hospital finance department based on tariffs per ICU day and the tariff cost of a typical HRG which in turn are based on costs collected from hospitals across the National Health Service. Sixty-nine per cent of our costs were ICU costs calculated on an individual patient basis as the product of ICU days and maximum organ support. We expect these to be an accurate representation of the true cost. Thirty-one per cent of our costs were outside of ICU costs and a combination of the cost of individual interventions such as ICD implantation and the HRG tariff. While the interventions are accurate on an individual basis, the HRG costs are more of an ‘average’ reflection of the type of admission.
Good quality survival (hospital discharge with CPC 1–2) occurred in 26/69 (38%) patients with an overall survival to hospital discharge of 33/69 (48%). This is a significant improvement from the UK average 28.6% overall survival to hospital discharge rate of ICU admissions with ROSC reported by Nolan in 2007;11 possibly representing both advances in management of these patients and the volume-outcome relationship. Targeted temperature management occurred in all but five patients and coronary angiography was performed in 48/69 (70%) of patients.
In contrast to other costing studies, our study provides fairly current data from the time period of 2011–2012, following the widespread introduction of TTM and PPCI. Unfortunately methodological differences make direct comparison with other costing studies challenging. Additionally, there are time dependant inflationary changes and variations in purchasing power between different regions. Nationally these are adjusted by MFF corrections embedded within the tariff-based system. Internationally however, comparisons are much more difficult. We used individual patient costing data from an 18-month period to provide our cost figures but have included only inhospital costs and we were unable to estimate prehospital or posthospital costs.
In a 2004 Norwegian study Naess et al14 used data from OOHCA patient identified via Emergency Medical System (EMS) registers in Oslo over a 20-year period (1972–1992) to identify all patients admitted to ICU with ROSC following OOHCA of presumed cardiac aetiology. They estimated costs per survivor of €40 642 (£33 761) and costs per life year gained of €6632 (£5509). Their cost per survivor included the cost of the non-survivors. It also included prehospital, inhospital and posthospital rehabilitation and nursing home costs but used average ambulance costs and the product of individual length of stay and average 24 h coronary care, ward costs and nursing home costs, respectively. In contrast to our study, their mean length of stay (survivors and non-survivors) in coronary care (3.4 days) and the general ward (mean 6.8 days) was very short. Their patients spent an additional mean 11.2 days in rehabilitation/nursing home care. This shorter mean stay may reflect a reduced survival percentage (26% of those with ROSC compared with 48% in our study) and different management protocols at the time of the study. UK data of ICU patients admitted with ROSC following OOHCA over a 10-year period 1995–2005 had similar survival (28.6%) to the Norwegian study, again preceding the widespread introduction of TTM and PPCI.11
In a 2004 Dutch study van Alem et al15 used data from OOHCA patients identified via EMS registers in Amsterdam over 2 years (2000–2002) and calculated the cost of a survivor to be €28 636 (£23 788) and a non-survivor to be €2383 (£1979). They also included prehospital, inhospital and posthospital care and used a more ‘bottom-up’ approach, however their cost per survivor did not include the cost of the non-survivors. Their 50% survival to hospital discharge of those with ROSC (72/144 patients) was slightly higher than our overall survival but their analysis included patients with rapid ROSC and return of consciousness who might bypass ICU direct to CCU in our study and were not included. Their lengths of critical care stay were considerably shorter with mean 2.85 ICU days, 4.93 CCU days and 28.3 hospital days total per survivor. Their much lower cost per non-survivor (£1979 compared with £14 192) may be a reflection of a majority of non-survivors who did not even survive to hospital or ICU admission.
In a 2008 German study Graf et al16 used 3-year data from ICU admissions with ROSC following cardiac arrest from a single hospital (1999–2001 inclusive). They completed an individually costed ‘bottom up’ approach, including prehospital, posthospital and inhospital costs to calculate their cost per survivor of €49 952 (£41 495), cost per life year gained of €10 107 (£8396) and estimated cost per QALY (5-year survivors only) of €13 126 (£10 904). Their study also included inhospital cardiac arrests (accounting for 31% of patients). Nevertheless their survival to hospital discharge was similar at 42% (compared with 48% in our study). Their mean overall (survivors and non-survivors) ICU stay was 9 days (compared with 10.2), with a mean hospital stay of 25 days (compared with 24.3). Mean daily ICU cost was €2693 (£2237) compared to £1675 and mean per patient ICU costs were slightly lower at €17 832 (£14 813) compared to £17 142. The results obtained via our method therefore correspond very well with the fully costed ‘bottom up’ approach used by Graf et al.16
The major determinant of our calculated inhospital cost was length of stay—in particular length of ICU stay. Our length of hospital and ICU stay is higher than previously reported in UK studies (although comparable to that reported by Graf et al).16 Nolan et al11 reported a median ICU length of stay of 2.9 days in ICU survivors of OOHCA (our median 10 days) with a median hospital length of stay of 18 days in hospital survivors of OOHCA (our median 27 days). However, survival to hospital discharge was 28.6% compared with 48% in our study. While the increased length of stay may reflect delays introduced by TTM to clinical course and delays in prognostication, it also may reflect improved survival in our population. It is also possible that in our institution we are relatively slow at arriving at a withdrawal of active-care consensus with patients’ families. This may reflect local experience and the nature, ethnic and religious background of the population of North West London. Variation in the practices of withdrawal both within the UK and Europe is well recognised.27 It is notable that the 2007 Nolan study median time to start withdrawal was 2.4 days which by current standards is early to attempt accurate prognostication especially in the era of TTM.12
Of our patients admitted to ICU with ROSC following OOHCA, the cost per survivor to hospital discharge was £51 000, the cost per CPC 1–2 survivor was £65 000, and the average cost per CPC 1–2 1-year survivor was £80 879. The NHS is economically stretched by limited resources, an increasingly ageing population and increasing availability of expensive drugs and treatments. Fairness (or ‘justice’) in resource allocation in such conditions requires an understanding of the economic cost-benefit ratio of interventions. Studies have shown that survival curves following cardiac arrest return to normal after 1–2 years28–31 and systematic review demonstrates that survivors have a good quality of life.32 Treatments can be usefully assessed using QALYs. The threshold value for cost effectiveness in the UK is £30 000.33 In our study the extrapolated cost per QALY of a high-quality survivor is £16 000, well within this threshold. This is using very conservative estimates for utility and survival and thus the true cost per QALY is likely to be lower than this.
This study was a retrospective review of prospectively collected data and had a number of limitations some of which have already been discussed above. It is important to highlight that our aim was to investigate the cost-effectiveness of ICU admission with ROSC following OOHCA and thus our population was patients admitted to ICU rather than all-comers with ROSC. Some of the best outcomes following OOHCA will be in patients not captured in this study (ie, those with rapid ROSC, consciousness and admission to CCU or normal ward level care). These patients will be less expensive.
Although the costing method used is a nationally imposed model, it is somewhat dependent on how individual clinical coders enter data, thus some caution is needed in applying our figures to other institutions. Also, the approach that is adopted in determining prognosis and managing end-of-life issues in our service may not be representative of wider practice. However, we do not feel that these issues undermine the general level of costs estimated. In addition we made no attempt to estimate prehospital or posthospital costs of patient care. Other limitations of this study include the retrospective nature of the study and the fact that CPC status was decided by review of the clinical notes. Finally in the absence of longer term follow-up data for our 2011–2012 population, our QALY data was an extrapolation using previously published values for survival and utility.
Conclusion
Patient survival to hospital discharge of 48% following ICU admission with ROSC after OOHCA in our institution is considerably higher than historically reported in UK studies, though comparable with recent clinical trials. The major determinant of hospital cost is ICU length of stay. The overall cost burden for high-quality survivors is inflated by high costs of treating those who die or survive with poor outcome and who necessarily experience long lengths of stay. However, the majority of patients discharged from hospital have a CPC of 1–2, and treatment including ICU is thus cost-effective by current standards with an estimated cost per QALY of £16 000.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
Contributors JP collected outcome data, calculated cerebral performance categories (CPC), managed database, performed statistical calculations and wrote most of the article. SE provided detailed information regarding hospital accounting, tariff calculations and provided permission to use re-imbursement data. VN provided financial details for each case in study group. CL helped collect outcome data and integrate CPC data. SJB suggested article concept, provided technical support, checked statistical methodology, assisted with proof-reading and guided submission strategy. RS created original database from ambulance and hospital records, integrated cost data with patient data, supported main author, assisted with proof-reading and coordinated submission process.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Ethics approval This study is regarded as ‘service evaluation’ by NRES guidance and therefore ethics approval was not sought.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.k78g1.