Article Text

Abstract
Objectives To explore perceptions of the current practice and future potential of advanced practitioners (APs) from the perspectives of different professional groups in Wales UK.
Design A qualitative study consisting of nine focus group interviews.
Methods Initially verbatim transcriptions of each focus group interviews were analysed thematically before themes were merged to represent perceptions for the whole data set.
Participants Data were gathered from a total of 67 stakeholders—including APs from a variety of professional groups (eg, nursing, physiotherapy, paramedics) as well as managers, workforce developers, educators and medical staff who have a role developing and supporting APs in practice.
Results The results are presented in four themes: (1) demand, policy context and future priorities, (2) role clarity and standardisation, (3) agreement and understanding of the role and (4) interprofessional working. The context within which current and future AP roles were considered was influenced by inexorable demands for healthcare and the requirements to meet health policy priorities. Developing AP roles were hampered currently by a lack of shared understanding and ‘joined-up’ working between different groups such as medical practitioners, managers, commissioners and educators.
Conclusions For the AP role to flourish more ‘joined-up’ thinking, support and development opportunities are required between APs, managers, senior clinicians, commissioners and educators. Working together to plan and deliver education, innovation and service delivery is of prime importance to meeting ever increasing complex health needs. This will ensure that future APs are adequately prepared and supported to reach their full potential and help deliver necessary innovations in current models of care delivery.
- QUALITATIVE RESEARCH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
A major strength of our study was the inclusion of perspectives from a range of healthcare professionals such as physiotherapists, nurses and medical practitioners as well as managers, educators and workforce planners.
Another strength was that nine focus groups, each lasting 45–60 min were undertaken with 67 participants, ensuring that the topic area was discussed in breadth and depth.
Although participants were recruited from across Wales the study was undertaken in a relatively small area of the UK. As a result it is not possible to draw wide generalisations from this study, although the breadth and depth of the perceptions obtained may aid in the transferability of findings.
Introduction
Health systems globally face a future of myriad complex issues including ageing populations, growing incidence of chronic conditions, rising public expectations and the challenge of cost containment. Such challenges require different approaches to the organisation and delivery of future healthcare, including an interprofessional workforce supported by new skills and expertise.1
The challenge of future-proofing healthcare systems will largely fall to the existing workforce to implement as, for example, the majority of staff who will be working in the UK National Health Service (NHS) in 2025 are already in post.2 ,3 However, many were trained to work in a model of care that is increasingly different from that currently in existence or that required in the future.4
One response internationally to this impetus for changes to healthcare delivery has been the promotion and development of advanced practice roles.5 The UK NHS has been particularly active in the development of APs, for example as a means of providing medical substitution to overcome recruitment difficulties and in leading the development of new, particularly community-based, healthcare services.6 Indeed, the Institute for Employment Studies reported that the single most common reason cited for introducing AP posts in the UK was to cover recent reductions in junior doctors’ working hours.7
The AP role
The volume of peer-reviewed literature relating to AP is vast but focuses mostly on nursing.8 The scale of this body of work confirms the significance of AP role to contemporary healthcare and its potential influence on improving patient outcomes across a wide range of professional groups.9 A theme resonating throughout the international literature is that the concept of the AP role promises much, but remains ambiguous and lacks universal understanding, with variability in role definition and scope.10 ,11 However, there is national and international agreement that the academic level of education required to prepare APs should be at Masters level, although clinical competency at AP level is currently variable, often locally determined, and is not underpinned by professional standards for most of the disciplines involved in such roles.12
For the purposes of this paper we have adopted the International Council for Nurses definition of AP,13 who is a registered practitioner thatHas acquired the expert knowledge base, complex decision-making skills and clinical competencies for expanded practice, the characteristics of which are shaped by the context and/or country in which s/he is credentialed to practice. A Master's degree is recommended for entry level.
The lack of clarity in literature and policy is mirrored in practice by the proliferation of AP roles and titles which appear to have emerged as a result of addressing local need to fill gaps in the workforce, rather than as a result of centralised planning or regulation by national bodies.5 Indeed UK regulators have clearly signalled they have no intention of regulating advanced practice, stating that ‘much of what is often called AP across many of the health professions does not make additional statutory regulation necessary’(ref. 14, p.1) a position that has since remained unchanged.15 This is in stark contrast to the USA where, for example, titles related to advanced nursing practice are legislatively protected and require specific academic courses to be completed prior to nurses using such titles.16 As well as leading to conceptual confusion the international inconsistency in terminology related to AP has resulted in practical consequences in terms of recruitment and workforce planning given the increased global mobility of the healthcare workforce.17
The potential for confusion over terminology, competencies and roles related to AP16 in the UK has led to national healthcare bodies intervening with best practice guidelines.18–20 However, it remains to be seen whether the belated introduction of such advice will be able to influence a more standardised and coherent approach in developing and managing AP roles. Against this backdrop this paper reports findings from a qualitative study of interprofessional perceptions and current practices of AP roles in one area (Wales) of the UK.
The Welsh context
AP roles in Wales have been influenced by a number of policy directives21–23 which cite AP as a route for career progression and service innovation in healthcare practice. In Wales, as elsewhere, it has also been recognised that delays in providing AP job title protection and standardisation had led to an unstructured development and proliferation of such roles and titles.5 In response the Framework for Advanced Nursing, Midwifery and Allied Health Professional Practice in Wales20 emphasises the need to standardise and support current and future advanced role development and implementation in nursing, midwifery and the allied health professions.
The aim of this paper is to report on a study to better understand the current situation regarding AP roles in Wales, and associated issues such as the relevance of educational programmes, employment practices and support for APs in the workplace. Given that AP roles are being implemented internationally in response to a common set of challenges the findings from this study are likely to be of interest to a broad readership of healthcare practitioners, workforce planners, commissioners, educators and managers. Specific research questions that guided the study were:
What is the current situation regarding the commissioning and employment of APs in Wales?
What are the priority areas for future investment in AP roles?
What educational preparation and workplace support do APs experience and require to ensure that they are able to deliver effective practice that is responsive to health needs?
Methods
A qualitative research design was adopted consisting of thematic analysis of transcribed focus group discussions. Research ethics approval was gained from Cardiff University School of Healthcare Sciences (April 2013). Data collection and analysis was conducted with due regard to the principles of informed consent and respect for confidentiality of participants. Information letters were sent to participants a week before focus groups were held, while written consent forms were obtained from each participant on the day of the focus groups.
Purposive sampling and data collection took place April 2013 to December 2013. Data were collected from all those who agreed to participate. Invitations to participate in the study were delivered via Welsh Government's Workforce, Education and Development Service email lists, providing the research team with access to individuals with direct experience of AP either by being employed as APs in the NHS, working in NHS workforce planning, education or in an area of healthcare directly linked to advanced practice. Academic staff members delivering AP education programmes were recruited via the email lists of Higher Education Institutions (HEIs) in Wales.
Focus groups
The decision to utilise focus groups as the method for generating data was taken for the following reasons. First, they provide a relatively quick and convenient way to collect data from several people simultaneously. More importantly, in view of the project aims, the method is also particularly useful for exploring experiences and can be used to examine what and how people think, but also why they think that way. Our focus groups saw participants ask questions of each other, exchange anecdotes and comment on each other’s experiences, all of which are considered key attributes of the focus group method.24
Nine focus group interviews of 45–60 min duration were conducted with participants (n=67) from various professional groups including practising APs, medical practitioners, educators from HEIs, education commissioners from Welsh Government and development representatives from NHS Wales. This purposive sample allowed the team to recruit ‘information rich’ cases, namely those whose healthcare roles made them likely to contribute data that were relevant to the research aim. The decision on sample size was informed by practical considerations regarding available time for recruitment, organising data collection and completing the project within the timescale agreed with the funders. We were also satisfied that a total sample of 67 professionally diverse individuals would provide the substantive topic expertise, detail and depth of experiences that is needed to build a convincing analytical narrative.25
All focus groups were held in a ‘neutral’ venue (a local conference centre, thus neither NHS nor University property), audio recorded and transcribed verbatim by a university approved commercial company experienced in transcribing focus group data. A member of the research team checked each transcribed interview for accuracy against the relevant audio file; no issues of accuracy were found.
Focus groups consisting of either seven or eight participants were arranged to ensure they were not too difficult to control, nor too large to limit each person's opportunity to share insights and observations (box 1). They were conducted by two researchers, one delivering questions via a semistructured topic guide focusing on a range of issues derived from prior readings that were relevant to the aims of the study, while the other observed interaction, took notes and ensured the proper functioning of recording equipment.
Breakdown of focus groups participants
Five focus groups with National Health Service (NHS) staff and Higher Education Institutions (HEI) staff for example, those involved in workforce planning or organisational development directly linked to advanced practitioners (AP) development or those delivering AP educational programmes (n=36).
Three focus groups with APs working in the NHS (n=24)
One focus group with Medical Practitioners directly linked to AP development (n=7)
Data analysis
Thematic data analysis was informed by the original aims of the research but initially progressed in an inductive fashion, starting with identifying themes and categories of the participants themselves. An iterative process of analysis initially consisted of the authors individually analysing data from focus groups allocated to them, before the research team agreed emerging themes across data sources. This method of analysis enabled the progressive understanding of the interview data to interact with the research team’s own emergent thoughts and the research aim. The inductive process of analysis and theme generation was aided by NVivo software.
No attempt was made to analyse the interactional dynamics within the focus group; instead the analysis focused on what was said rather than how things were said. The aim was not for analysts to arrive at the exact same themes but for similar themes to merge, meaning the data were carefully analysed to provide a reduced, yet accurate representation of the participants’ views. This process corresponds with approaches to establish rigour in qualitative research, in particular establishing credibility which represents means of conferring value and believability to qualitative findings.26 Finally, the findings were informed by existing literature, such as prior international research on advanced practice.
Results
Inexorable and unprecedented demand on health services directly linked to policy changes emerged as the overarching context within which AP roles and responsibilities were being commissioned and undertaken. Themes relating to perceptions of AP included: differences between the realities of the role as experienced by practising APs and the perceptions of other professional groups of AP roles. Further themes included differences in perceptions about the educational preparation and on-going support of APs and view of interprofessional working. These themes are summarised in figure 1 and discussed in more depth in the following sections. Selected extracts illustrative of each theme are presented as indicative of participants’ views. The Consolidated Criteria for reporting qualitative research (COREQ) has guided preparation of this paper.27
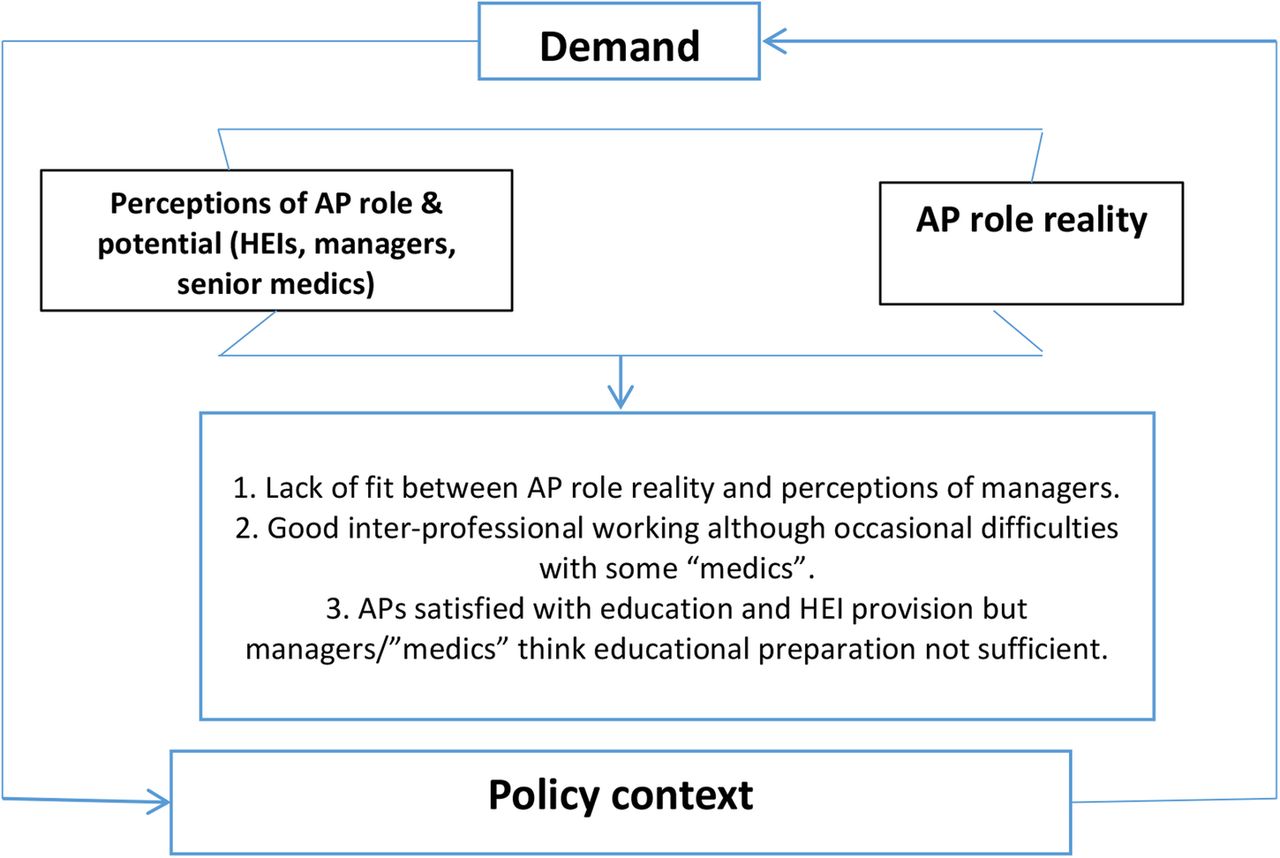
Schematic of themes emerging from the data. AP, advanced practitioners; HEI, Higher Education Institutions.
Demand, policy context and future priorities
The context within which AP roles were commissioned and practised was dominated by the increasing demand for healthcare services due to an ageing population and associated growth in numbers of comorbid conditions. As the following extract demonstrates a related need was to develop different ways of working in order to fulfil Welsh Government policy targets:The biggest pressure is the increasing amount of referrals year on year, and I think that's tied into the ageing population, we see a lot of people who are elderly and also with co-morbidities and against that pressure we've got the national driver so for example with stroke, the government targets so there's always pressures within that area as well. (Speech and Language Therapist 3)
More and more patients and more and more policy guidelines are continually challenging us to tweek our services and the type of practitioners we have. It does feel relentless at times trying to keep up with all those demands and we don't have much time to take stock. (Workforce Development Manager 3)
However, there was little consensus around the priority areas for the development of AP roles. This reflected the unprecedented demand already referred to as well as the actual and potential broad scope of AP roles. Key clinical priority areas for AP roles discussed during the focus groups included (among others): unscheduled care, mental health, dementia, emergency care, neonatology, primary care and paramedic roles. One unifying theme to emerge from the data was that current and future AP roles had a crucial part to play in hospital avoidance and more timely discharge of hospital patients into the community.If we used advanced practice roles more in elderly care, in medicine pathway, in preventing the chronic bronchitic who regularly comes to hospital, getting admitted because they've got access to somebody who can manage their respiratory needs in a different way outside of hospital, then we stop thirty beds being blocked. (AP Nurse 5)
Hospitals are failing to discharge people effectively and if you look at the evidence you have to say that the speed of discharge and people were assisted by those advanced practitioners is far greater than when you don't have advanced practitioners. So I think we must focus on community-based advanced practice to improve discharge. (Paramedic AP 4).
AP role clarity and standardisation
APs often drew attention to the lack of clarity with AP titles and subsequent understanding of AP roles. For example, many current AP roles have their origins in specialist nursing roles, resulting in the ‘advanced’ component of their role not being entirely clear, either at the point of taking up an AP job title or subsequently.My title is specialist nurse practitioner although my colleagues who have recently come into the same post have got the title of advanced practitioner so I would like to maybe clarify today whether I am an advanced nurse practitioner or an advanced practitioner or not [laughs]. (AP Nurse 1)
This confusion can be further compounded with the emergence of APs from different clinical professions including physiotherapy, paramedics, dietetics and radiography. However, AP roles in professions other than nursing have evolved more recently and seem to be shaped by Welsh Government guidelines. For example, one health region in Wales undertook a radical intervention to standardise the roles of non-nursing AP titles in response to government guidelines:As a result of the guidelines some of our advanced practitioners actually had the title taken off of them, not in nursing but in other professions and they couldn't have that rescinded until they'd done a portfolio which was interesting. (Nurse Manager 4)
Increased standardisation, in addition to clearer government guidance regarding the ‘buy-in’ of managers to policy guidance was also supported by practitioners who noted the current lack of parity in terms of work related terms and conditions for APs:I think there should be a clear all Wales policy direction on what AP is. Although the AP framework is there, managers need to sign up to that completely so that if you are an AP in various parts of Wales you are all working to the same level playing field. (Paramedic AP 2).
Lack of agreed understanding
Representatives from HEIs were keen to ensure that AP educational programmes were not seen as existing to teach specialist or advanced clinical skills only. The perceptions of many educators was that focusing only on skills could limit the potential of AP and lead to more entrenched professional groups:The truth is that we could just end up teaching skills but advanced practice is much more than this. The problem is there are different skills needed across professions and AP courses shouldn't just reinforce professional silos based on skills. (Educator 5)
I realise the need for skilled advanced practitioners but these skills need to be about management and research too not just whether someone can undertake clinical assessment. (Educator 8)
However, participants from the NHS were keen that educational programmes prepared APs to undertake a set of specific, advanced skills, which were underpinned by the appropriate evidence. The need for skills reflected the ‘reality’ of the ever-changing demands of practising at an advanced level; the view of some was that HEI provision struggled to keep up with such demands.We need education to reflect the reality of our jobs at advanced level. We verify death, we take ABGs (arterial blood gases), we cannulate, we reassess patients clinically and obviously move forward and make independent decisions. The pressures on us are phone calls, emergencies, numerous sort of tasks that need to be done now. (AP Nurse 3)
Sometimes I think HEIs are out of touch with reality and what they provide. (Paramedic AP 3)
Those managing and commissioning AP roles similarly demonstrated a lack of confidence in the educational preparation of APs. The first extract is taken from a medical consultant who had commissioned an AP nurse role. Despite the AP having the MSc AP qualification a further 18 months of practical training was arranged to ensure “she was proficient in doing the practical procedure”.We employed the individual as she was already a Band 7 sister but we employed her as a Band 7 advanced nurse practitioner, working day time with me for 18 months to make sure she could be trained and that she was proficient in doing the practical procedure that she needed to. (Medical Consultant 2)
Similarly, a nurse manager provided justification for insisting that advanced practitioners had achieved a Masters level course and undertake further trainingMy view in terms of education as a manager is that I don't know what the curriculum is, what the curriculum is spitting out, what standards are actually worked out. The comment you made to me about “these practitioners do their Master's level course and then you're going to put them on a service training course” and yeah I'm going to do that because I'm not assured in terms of governance arrangement what it is they've been taught. So I want to be 100% sure so yeah I do make them jump through these additional hoops. (Nurse Manager 1)
The above data extract reveals some interesting things; first that the manager had little faith in educational provision and second, that the managers’ lack of faith was predicated on a lack of knowledge and understanding of the AP curriculum and academic standards therein. The following extracts convey how practitioners often considered their managers as being out of touch with the realities of AP roles and tasks:Managers don't know what you do, there's lack of education and understanding of what the roles can actually put into the organisation. (Speech and Language Therapist 1)
I think there's a lot of skills that advanced practitioners have that a lot of people who organise services within the organisation don't know that they have, so almost like marketing, you know we can insert cannulas we can prevent a diabetic being admitted we can, you know, get somebody out of A&E with a toilet raise or whatever. (AP Nurse 5)
My bosses don't think about the workforce planning they need to fit in and around my post, it feels like somebody's happy because you've met a service need but actually they don't get the totality of what it is we do. (Paramedic AP 3)
These extracts suggest there is a distinct possibility that some workforce decisions regarding the educational and developmental needs of APs in Wales are made from a position of relative ignorance of the realities of clinical practice and the fit that exists with educational programmes used to prepare APs. In addition, some practitioners also described how AP roles could be commissioned and introduced without managers fully appreciating the on-going support and development needed by those being employed; as well as those managing APs failing to keep up with evolving AP roles:They bring in the service but in my experience professional development often isn't planned for, it's not somebody thinking right we need a practitioner to do that and the managerial support then evolves to keep up with the demands and professional development that's happened. Managerial support just doesn't adapt with us. (Physiotherapist AP4)
Regarding a nurse AP her manager whipped her off to London to do a course. She's come back and she's doing the job of a junior doctor on the ground without a consultant there. As a practitioner she hasn't got a job description that matches it. She's got no clinical supervision. She isn't doing any audit, which is scary. So basically some manager thought that's a good idea, our service needs that and I will just sort of do it. (AP Nurse 6).
Interprofessional working: benefits and challenges
In terms of role preparation another feature that was highlighted was that, although a focus on skills-based learning was preferred by many AP role holders, having a good understanding of other health professional groups was also seen as a priority, typified in the following extract.I think inter-professional working is absolutely key and I can see clear benefits of advance practitioners working across boundaries and understanding others’ development. (Physiotherapist AP2)
There was also evidence that AP courses were preparing practitioners who worked inter-professionally to a high standard.I've got a few medical colleagues, two teams and each of them have got a qualified AP attached to their ward team providing ward care and they would rather give up their foundation doctors than their AP I promise you’. (Medical Practitioner 1)
However, interprofessional working, especially between medics and APs from a variety of professional backgrounds, was not always harmonious.Interviewer: Have you had support from medical practitioners?
Paramedic: Yes, with a gun held to their heads until they give in.
Paediatric Nurse: I agree to a point but things changed, when the medics finally realised that we were an asset and we were a resource then the atmosphere changed and now if they want somebody to review patients with them, they don't pop along to the SHO or the House Officer, they will take one of the APs because they know that we'll know the history of the child, we'll know the current treatment plan and we'll give a better picture.
Similarly, in physiotherapy substantial barriers to advancing practice had to be overcome with the result that innovation in service provision was being stifledI came into post about 8 years or so ago and it's been a very long and arduous and frustrating journey because we never had that support from medics. Just to give an example it took me nearly 7 years to get an injection policy through to allow physiotherapists to inject. (Physiotherapist AP1)
Working with medical staff has historically proved to be very frustrating for APs from all professional groups, as they often had to endure several months of negativity and limited collegiality which would only be alleviated once certain unspecified but significant ‘rites of passage’ and ‘personal tests’ had been successfully negotiated by APs. Fortunately there are some signs of this improving, with abundant support and professional development offered more readily as the AP role proves its worth.
Thus, interprofessional working was perceived as a balancing act between those who traditionally had the power and carried out certain tasks—usually medics—being willing to co-operate and trust APs to carry out these tasks and functions safely. This process of monitoring was presented as unofficial, negotiated and context-specific.
Discussion
There is little doubt that APs are, and will continue to be, an important part of the healthcare workforce, both across diverse professions such as nursing, physiotherapy and paramedicine and in diverse areas of healthcare practice such as accident and emergency, mental health and primary care. For example, increased training and recruitment of APs in areas such as nursing and pharmacy has been identified as one of the solutions to the severe current and future shortfall of general practitioners in the UK.28 Our study is therefore very timely, especially as it provides insights from groups that have an important part to play if AP roles are to flourish. We have not located another study in the field of AP that has sought and combined the views of clinicians, educators and managers.
Our results suggest that significant barriers exist that may undermine the successful development and integration of APs into the healthcare workforce. One such barrier is the variable level of managerial and medical support and coordination of AP roles in Wales. Consequently, APs who participated in our study reported developing innovative practices often despite, rather than because of, the support and involvement of managers and medical staff. This finding evokes existing research that describes AP roles in the UK and internationally as having often developed in an ad-hoc manner, with little organisational coordination and attention given to sustainable funding for the role itself, on-going support and training and succession planning.29 ,30
A related barrier is the apparent lack of agreement between APs, educators, managers and senior medical staff about the preparation and training required to undertake the AP role. For example, participants from the latter two groups expressed concerns about the educational preparation of APs to practice competently, views which seemed to be based on a lack of understanding of the Masters level courses that APs had already undertaken. As a result of this, we propose that those who commission and manage APs should urgently familiarise themselves with the educational programmes on offer locally and nationally in order to fully determine whether the additional training being imposed on some APs is actually needed. The current lack of understanding may impede the development of AP roles and the fulfilment of their widely regarded potential as significant contributors to workforce/service development and innovation.31
Additionally, we urge those key decision makers to consider making full use of the NHS Wales Advanced Practice Framework.20 The framework provides the opportunity to enhance the governance of AP roles in Wales by providing a shared means of introducing role standardisation, transparency and assurance regarding the scope and competence of APs. The framework can also help to guide decisions about further educational curriculum developments and educational commissioning, all of which have been identified as issues related to the development of AP roles that require addressing on an international level.16
Encouragingly, there was consensus across all the professional groups who participated in this study about the actual and potential value of the AP role in delivering effective services that are responsive to the current and future demands facing the NHS. All professional groups were also in agreement about the factors (figure 2) that could help to enhance the success of the role.

{kind=link}
{kind=link}
Factors identified by all professional groups that would enhance the success of advanced practice roles. AP, advanced practitioners.
These included the need for agreement and standardisation regarding APs educational preparation, clear role definition and for the nature and demands of AP to be fully understood and supported by key professional and managerial stakeholders (such as medical consultants and line managers). While there was a clear call for more standardisation in various aspects of advanced practice, there was also a sense that unique practices that were profession or role specific also needed to be valued and developed. For example, enhanced support for continuing professional development was identified as a factor critical to the future success of APs, in terms of maintaining existing competencies and in supporting the development of new professional roles as services continuously evolve.
The ideal advanced practitioner of the future, as envisaged by study participants, would therefore consist of a balanced blend of interprofessional worker who undertook specialist professional roles and clinical skills that were responsive to the ever-changing demands of healthcare. All APs would be employed to standardised terms and conditions of employment across all professional groups and be prepared according to standardised, interprofessional educational programmes that have been agreed with senior clinicians, employers and educators.
Conclusion
Radical changes to the way in which future healthcare services are delivered are highly likely and such changes will inevitably lead to increased future demand in AP numbers and extended scope of the role. It became clear during this study that many practitioners in Wales are currently working at an advanced level, although it was equally clear that all the groups participating in the study felt that AP roles in Wales are yet to be fully optimised. Delivering more ‘joined-up’ support and development opportunities, where APs, managers, senior clinicians and the education sector work more closely, must therefore be prioritised to ensure that future APs are recruited, retained and developed appropriately. Suitable support and development opportunities would ensure that APs function to their full potential and help deliver much needed innovations to current models of care delivery.
Some of the lack of shared understanding between key stakeholders about APs suggests the need to create a forum that facilitates ‘joined-up’ thinking between employers, clinicians, educators and the commissioners of education programmes. Such a forum could help ensure that educational programmes and professional development opportunities reflects the needs of all stakeholders while supporting APs to deliver safe, innovative practices that meets the needs of rapidly evolving health systems. We suggest that AP roles will assume even greater importance in healthcare in the future and believe that there is an urgent need to consider their potential in a more systematic and creative manner.
Acknowledgments
The authors would like to thank the following for their assistance during data collection: Dinah Gould, Julie Rasmussen, Sarah Fry and Neil Thomas.
Footnotes
Twitter Follow Aled Jones at @aledjonze
Contributors All authors were involved in study design, data collection and analysis. AJ and TP drafted the paper and all authors contributed to subsequent re-writing and revising the paper. All authors approved the final version of the paper.
Funding The study was funded by NHS Wales Workforce and Education Development Service.
Competing interests None declared.
Ethics approval Cardiff University, School of Healthcare Sciences Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.