Article Text

Abstract
Introduction There is limited evidence demonstrating the benefits of community-based water, sanitation and hygiene (WASH) programmes on infections with soil-transmitted helminths (STH) and intestinal protozoa. Our study aims to contribute to that evidence base by investigating the effectiveness of combining two complementary approaches for control of STH: periodic mass administration of albendazole, and delivery of a community-based WASH programme.
Methods and analysis WASH for WORMS is a cluster-randomised controlled trial to test the hypothesis that a community-based WASH intervention integrated with periodic mass distribution of albendazole will be more effective in reducing infections with STH and protozoa than mass deworming alone. All 18 participating rural communities in Timor-Leste receive mass chemotherapy every 6 months. Half the communities also receive the community-based WASH programme. Primary outcomes are the cumulative incidence of infection with STH. Secondary outcomes include the prevalence of protozoa; intensity of infection with STH; as well as morbidity indicators (anaemia, stunting and wasting). Each of the trial outcomes will be compared between control and intervention communities. End points will be measured 2 years after the first albendazole distribution; and midpoints are measured at 6 months intervals (12 months for haemoglobin and anthropometric indexes). Mixed-methods research will also be conducted in order to identify barriers and enablers associated with the acceptability and uptake of the WASH programme.
Ethics and dissemination Ethics approval was obtained from the human ethics committees at the University of Queensland, Australian National University, Timorese Ministry of Health, and University of Melbourne. The results of the trial will be published in peer-reviewed journals presented at national and international conferences, and disseminated to relevant stakeholders in health and WASH programmes. This study is funded by a Partnership for Better Health—Project grant from the National Health and Research Council (NHMRC), Australia.
Trial registration number ACTRN12614000680662; Pre-results
- EPIDEMIOLOGY
- INFECTIOUS DISEASES
- PARASITOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first randomised controlled trial assessing the impact of an integrated community intervention comprised of water, sanitation and hygiene (WASH) and mass albendazole distribution on infections with soil-transmitted helminths (STH) and intestinal protozoa.
Results of this study will provide evidence on the benefits of intersectoral collaboration between the health and infrastructure sectors in order to achieve more effective and sustainable STH control.
The impact of the intervention will be conditioned by the level of adherence of the communities to the WASH intervention, particularly the construction and continued use of latrines.
Control communities may be exposed to interventions led by other organisations, or improve their WASH status due to economic and social development of the country or ‘contamination’ from the intervention clusters.
Given that viable helminth eggs (particularly Ascaris spp) can persist in the environment for several years, the follow-up time may not be long enough to detect changes in rates of reinfection.
Introduction
Soil-transmitted helminths (STH), which are among the most prevalent infections worldwide, include Necator americanus, Ancylostoma duodenale, Ancylostoma ceylanicum (hookworms), Ascaris lumbricoides (roundworm), Trichuris trichiura (whipworm) and Strongyloides stercoralis (threadworm). It has been estimated that globally, in 2010, there were 819 million people infected with A. lumbricoides, 465 million with T. trichiura, 439 million with hookworms and, in 2006, 30–100 million people infected with S. stercoralis.1 ,2 Chronic and intense STH infections contribute to malnutrition and iron-deficiency anaemia, and adversely affect physical and mental growth in childhood.3–5 The protozoon Giardia duodenalis causes diarrhoea, malnutrition and wasting in approximately 2.8 million people annually,6–8 while Entamoeba histolytica causes intestinal and extraintestinal amoebiasis, affecting approximately 50 million people, and resulting in approximately 100 000 deaths annually.9 Cryptosporidium spp are an important cause of diarrhoea, especially in immunocompromised hosts and children, being associated with malnutrition and deficient child growth.10
There has been a renewed global commitment over the last two decades to finance and implement control strategies to reduce parasitic disease burdens.11 STH control is possible because of the availability of cost-effective and logistically feasible intervention strategies: regular periodic mass (targeting entire communities) or targeted (focused on school-age children) chemotherapy, using the benzimidazole anthelmintic albendazole.12 In some studies, treatment has been shown to reverse negative health consequences of parasite infection, including anaemia and poor growth,13 and had a positive effect on improving cognitive function and school performance,14 and decreased school absenteeism.15
In 2001, the 54th World Health Assembly passed a resolution to provide regular deworming treatment to 75% of at-risk school-age children by 2010, defined as the figure required to eliminate STH as a public health problem in childhood.16 Despite great progress, only 200 million school-age children of the 610 million in need received treatment in 2010.17 ,18 Continued international interest in parasitic disease control, as embodied by the London Declaration on Neglected Tropical Diseases (NTD) in 2012, saw several pharmaceutical companies and global health institutions announce their commitment to meet the revised target of 75% deworming coverage of school-age children at risk by 2020, with significant donations of anthelminthic drugs promised.18
As adult worms, STH inhabit the host intestine where they are able to survive for several years and produce large numbers of eggs starting 5–11 weeks after infection.2 Once passed during defaecation, A. lumbricoides and T. trichiura eggs can remain viable in the soil for several months, and hatched hookworm larvae for several weeks.19 STH infections occur through accidental ingestion of A. lumbricoides and T. trichiura eggs and through oral ingestion or penetration of the skin by hookworm larvae.2 Transmission of protozoal parasites can be direct through person-to-person and animal-to-person contact, or via the ingestion of water or foods contaminated with faeces containing protozoal oocysts and cysts.20
Deworming treatment only has immediate impacts on killing the adult parasites within the human host and does not prevent rapid reinfection if the host contacts an environment contaminated with infective stages of the parasites.21 Therefore, in the absence of improved sanitation and personal hygiene, the prevalence of infection will return to pretreatment levels within 6–12 months of a single round of deworming.21–25 Chemotherapeutic interventions successfully act to reduce morbidity caused by STH infection in the short term, however, for longer term control, deworming interventions must be repeated periodically.17 ,24 Another concern associated with the scale-up of periodic deworming campaigns is the risk for drug resistance to occur, similarly to what has been reported in veterinary parasitology.26 For longer term and sustainable reduction in parasite-associated morbidity due to STH, additional control strategies, based on improved water access, sanitation and hygiene, are required.27 ,28
There is evidence for the benefits of water, sanitation and hygiene (WASH) interventions on several NTFs, including on STHs, and for the prevention of diarrhoea.29–34 In the case of STHs, a recent meta-analysis suggests that, in general, individual components of WASH access and habits are associated with at least a 33% reduction in the odds of infection with any STH.31 However, most large-scale community-based parasitic disease control programmes focus almost exclusively on mass or targeted chemotherapy without investing in WASH improvement; primarily because of the perceived high costs of providing infrastructure, but additionally, in some settings, due to the lack of coordination between the health and the infrastructure development sectors.28 ,35 On the other hand, there are limited studies rigorously quantifying the additional benefit of WASH on STH infections,36 ,37 with the vast majority of investigations being observational studies, limiting the ability to establish causal inferences of WASH on STH infections.31 A few experimental studies have looked at individual components of WASH and its impact on worms: both sanitation and hygiene promotion/education have been shown to be effective.36 ,38–40 On the contrary, two recent randomised controlled trials (RCTs) assessing the impact of the Indian Total Sanitation Campaign on diarrhoea, STH and malnutrition did not find benefits of the intervention, possibly due to an insufficient coverage and use of latrines.41 ,42 When considering the three components of WASH, the only sufficiently powered RCT, to date, reported on a school-based WASH intervention describing a 44% reduction in A. lumbricoides reinfection in the intervention arm (OR 0.56, 95% CI 0.31 to 1.00), but no effect on T. trichiura or hookworm.37 To the best of our knowledge, there is no reported RCT adequately powered to evaluate the impact of integrated community-based WASH and mass chemotherapy programmes on gastrointestinal parasitic infections, although there are two similar intervention studies under way in Kenya and Bangladesh.43
In order to address these key evidence gaps, the WASH for WORMS trial aims to test the hypothesis that a community-based WASH programme integrated with mass chemotherapy with the benzamidazole anthelmintic drug, albendazole, will reduce infections with gastrointestinal parasites above that achieved through mass deworming alone. The specific aims of this study are:
To determine the effectiveness of a community-based WASH programme integrated with mass albendazole chemotherapy in reducing the incidence (hookworm, roundworm and whipworm) or prevalence (threadworm and gastrointestinal protozoa) of parasitic infection, in rural communities of Timor-Leste.
To determine the reduction in intensity of infection and in parasitic disease-related morbidity in children, including anaemia, stunting and wasting, achieved by implementation of the integrated WASH and mass albendazole programmes.
To understand the planning and implementation of the sanitation component, as well as the barriers and enablers associated with the acceptability and uptake of the WASH programme.
In this report, we present the trial design and study protocols.
Methods and analysis
Study design
This is a two-arm cluster RCT (figure 1). Cluster units are small rural communities in Manufahi district, Timor-Leste. This design was deemed appropriate because in this study the WASH programmes are implemented at the community level. All participating communities receive mass chemotherapy with single dose of albendazole 400 mg every 6 months, in accordance with WHO guidelines. Half the communities also receive the community-based WASH programme. The follow-up period is 2 years following the first albendazole distribution, during which four additional (6-monthly) rounds of chemotherapy are delivered. The study was initiated in May 2012, and field work will end in April 2016. This study is registered with the Australian New Zealand Clinical Trials Registry (Registration number ACTRN12614000680662). This study was registered after the baseline surveys were conducted, due to logistical and human resources constraints, but did not impair the study quality, nor the ethical procedures described below. At the time of registration, only baseline data had been collected, and no study outcomes had been measured; furthermore, the study has been managed throughout according to protocols developed prior to data collection.
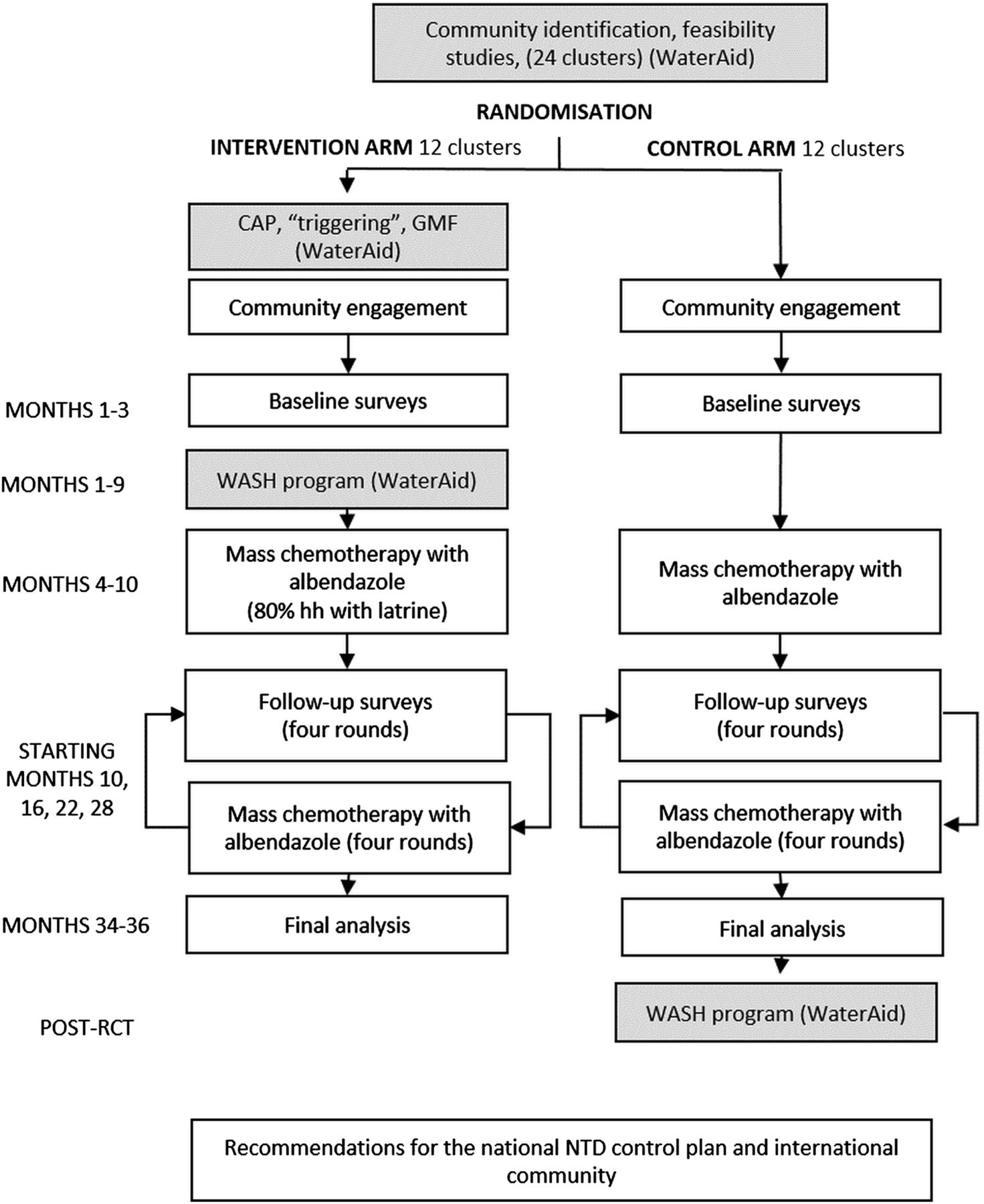
Flow diagram of the proposed cluster-randomised controlled trial. The study was initiated in May 2012 and field work will end in April 2016 (see figure 2 for details on the enrolment process) (CAP, Community Action Plan; GMF, Grupu Maneja Facilidade; WASH, water, sanitation and hygiene; RCT, randomised controlled trial; NTD, Neglected Tropical Diseases).
Setting
Timor-Leste is 1 of the 20 poorest countries in the world, and the poorest in South East Asia.44 According to the Global Health Observatory Repository Data of WHO in 2013, child mortality in under 5-year-olds was 55 deaths per 1000 live births, and infant mortality was 46 per 1000 live births above the 47 and 37 per 1000 live births average, respectively, in WHO's South East Asia region.45 ,46 Malnutrition and infectious diseases (including pneumonia, diarrhoea, malaria, dengue and tuberculosis) are major child health problems.47 A recent national STH survey, carried out in all 13 districts of the country in 2012, revealed a national infection prevalence of 29% in children aged between 7 and 16 years of age, with Manufahi being one of the six districts with the highest prevalence of STH infection.48 The high prevalence of STH infection in Timor-Leste strongly supports the need for an STH control programme. In 2005, the Ministry of Health (MoH) initiated a deworming programme, with support from WHO, known as ‘Lumbriga…Mak Lae Duni’ (Worms, no way!); the programme ceased in 2008 due to a shortage of funding. The MoH recently developed a National Integrated Plan for NTD control, which includes STH infections. Funds required for 2014 are estimated at US$1.3 million followed by US$1 million per year for subsequent years. Owing to limited available resources, the MoH plans to restart the implementation of the programme in 2015 in a limited number of districts.49
Integrated intervention
Community-based WASH programme
The non-governmental organisation (NGO), WaterAid Australia, has been working in Manufahi since 2012 on the improvement of the water and sanitation infrastructure, and is the implementer of the WASH intervention being evaluated in this trial in terms of impact on STH infection. The WASH intervention has three main elements:
Providing access to safe, adequate and convenient water supplies. WaterAid adopts a Community Management approach aimed at sustainable and optimal use of available water resources.50 WaterAid, through its local NGO partners, supports the community with the water supply system design and construction. During the Community Action Plan (CAP), a staged series of meetings that includes historical and gender analysis, WASH situation analysis, awareness raising and capacity building; there is the establishment of the Water User Group (also called the Grupu Maneja Facilidade (GMF) committee), consultations on the water supply system and technology options and, finally, planning of the construction of the water system. The majority of the water supply systems built are gravity-fed schemes whereby water is transmitted down to communities from higher water sources (eg, springs or small unpolluted streams). In areas where elevated water sources are not available, groundwater supply systems (eg, borehole with hand pump) are selected as one of the options. On gravity-fed schemes, the water is tapped, dammed and protected at its source before being piped to storage tanks near, or in, communities. Distribution pipes then feed protected tap stands, thus allowing water to be accessed by the community, with the maximum distance between each dwelling and collection point of 200 m (or less than 5 min round trip walking time). The construction process can take up to 10 months to complete, dependent on the community motivation and the water supply system size. During this process, the technical staff from the local NGO partner work together with the community on a daily basis with regular (at least once in a fortnight) support and mentoring from WaterAid technical staff.
Providing access to sanitation, particularly household latrines. This is achieved by increasing demand for improved sanitation, using a strategy inspired by the Community-Led Total Sanitation (CLTS) process. CLTS was pioneered by WaterAid and Village Education Resource Center in Bangladesh in 2000, and is now used in many countries as a technique for mobilising communities to eliminate open defaecation through social awakening rather than merely providing toilets.51 A key feature of the CLTS technique is the ‘triggering’ process which comprises several community activities, ideally culminating in the community deciding not to practise open defaecation, and to build their own latrines. In its original form, CLTS attempts to ‘trigger’ people's disgust and shame at open defaecation practices.52 WaterAid and local NGO facilitators convene the ‘triggering’ and engagement meeting, which usually lasts 1–2 days, prior to the CAP described above. The community activities comprise a transect walk through the community with the residents to identify open defaecation sites; creating a community map (usually on the ground with coloured chalk) of village boundaries, roads, residents’ houses, water points, open defaecation sites and any toilets; as well as presentations of various WASH-related health messages. After options for hygiene improvement are discussed, agreement with communities is reached to end open defaecation, and regarding the predicted schedule for household latrine construction. The most common types of latrine that are built are simple direct pit latrine, and the offset pit pour-flush latrine. The pits are generally at least 2 m deep, and completely above the water table. WaterAid and partners explain how to build a squat slab covering the pit, which should be strong and easy to clean, and with a lid to prevent flies coming into contact with faeces. These may be precast away from the pit and then placed over it, and can be used for direct and offset pit latrines. Slabs made from local timber and compacted earth are also often used. A shelter using local materials is then built to provide privacy and shelter. Care is taken to ensure that water resources are not compromised by sanitation activities through follow-up guidance to communities.
Improving hygiene behaviour, especially hand washing with soap at critical times. WaterAid and local partner NGOs use a combination of approaches to hygiene promotion, in addition to CLTS messaging, that target various target groups including households, children, women and community clusters, as well as the community in general, using various Information, Education and Communication materials (eg, flashcards, flipcharts, posters, snakes and ladders games, songs and video). The communities are also encouraged to use locally made models of hand washing stations, particularly the tippy-tap. All these activities are conducted within a period of 4–6 months usually once in every 2 weeks by the community hygiene promotion volunteer and partner NGO staff with regular support from WaterAid's staff.
While the WASH intervention is being implemented, there is monitoring of the construction of the household latrines and hand washing stations by local NGO staff and the community Water User Group leader. When all households have built latrines, there is verification of open defaecation-free status, during 1–3 days, by the district verification team, comprising representatives of the District Health Service, Department of Water Services, District Administrator Office and other stakeholders. Furthermore, WaterAid verifies the completion of the water supply system and carries out physical and microbiological water quality tests. Finally, every 6 months, for 2 years after the WASH intervention is completed, there are Post-Intervention Monitoring and Evaluation visits, where WaterAid, along with the Department of Water Services, assists the community Water User Group to conduct maintenance activities of the water supply system, and monitors the household latrine and hand washing station status.
Mass administration of albendazole
Albendazole is offered to all eligible members of the community regardless of whether they participate in the study. Children under 1 year of age, and pregnant women in the first trimester, are excluded. Administration of a single oral dose of 400 mg albendazole (Albenza, GlaxoSmithKline, Research Triangle Park, North Carolina, USA) is observed by the study team for each participating individual. Children under 2 years of age take half the dose.
In the intervention communities, the first round of mass distribution of albendazole was triggered by a sanitation intervention threshold, that is, 80% of households having a latrine. This information was provided by WaterAid based on routine visits to the intervention communities by their local NGO partners. In the control communities, albendazole administration was timed such that the lag between the baseline surveys and mass chemotherapy was as close as possible to that of the intervention communities. Thus, the first round of mass chemotherapy involved a second visit to each community that happened between 2 and 6 months after the baseline surveys. For the four follow-up surveys, albendazole is administered directly after collection of faecal specimens, meaning, that each community is visited once per round.
Study outcomes
The primary outcomes are 6-month cumulative incidence of infection with Ascaris spp, T. trichiura, N. americanus and Ancylostoma spp (undifferentiated), measured at each of the four follow-ups (table 1). Note, for Ascaris infections, albendazole is highly efficacious and infections diagnosed at follow-up are likely to be incident infections; however, for T. trichiura and hookworm infections, albendazole is less than 100% efficacious, and cases diagnosed at follow-up will include incident infections and prevalent infections not cured by previous rounds of albendazole.53 For simplicity's sake, we use the term ‘cumulative incidence.’ Secondary outcomes are the prevalence of S. stercoralis, G. duodenalis, E. histolytica and Cryptosporidium spp. For protozoa and for S. stercoralis, given the low efficacy of a single dose of albendazole, we will be measuring prevalence instead of cumulative incidence. Additional secondary outcomes are: the ratio of numbers of people infected with the hookworms A. duodenale, N. americanus and A. ceylanicum; the mean intensity of infection (calculated as the average number of eggs per gram of faeces, derived from the Ct values obtained in the PCR) of each of the most frequent STH, measured at 6-monthly intervals; and the mean haemoglobin (Hb) concentration and the anthropometric indices weight-for-age, weight-for-height and height-for-age Z-scores (to identify underweight, wasting and stunting) measured at 12-monthly intervals (rounds 3 and 5). Each of the trial outcomes, measured at each 6-monthly midpoint and at the 2-year end point, will be compared between control and intervention communities.
Trial outcomes to be compared between control and intervention communities
Sample size
Sample size calculations were for the primary outcome. Original sample size calculations indicated that we needed to include 12 communities in each of the intervention and control arms, assuming 120 participants per cluster, and a 10% loss to follow-up. We therefore aimed to enrol 2880 people, located in 24 clusters, randomised 1:1 between the intervention and control arms.
As explained below, three control and two intervention clusters were excluded after allocation (figure 2). At baseline, there were 2646 residents in the 19 remaining clusters that were randomly allocated, of which 2444 were present at the time of the visit. Of the 2371 residents who were over 1 year of age (ie, eligible) and present at baseline, 23 (0.97%) refused to answer questionnaires, 41 (1.73%) refused to give a stool sample, 2242 provided individual questionnaires (94.56%), and 1865 (78.66%) provided stool samples. During the first albendazole distribution visit, 2285 residents were present. Of the 2218 participants who were present and eligible, 2215 (99.86%) took albendazole.

{kind=link}
{kind=link}
Flow diagram of the enrolment process, putting in evidence the randomisation, allocation and enrolment process and replacement of clusters (WASH, water, sanitation and hygiene).
Given that original sample size calculations indicated the need for 12 clusters in each arm, we redid those calculations using the sample that we were effectively able to recruit at baseline. For N. americanus, the most prevalent STH in the study communities, given an observed intraclass correlation coefficient (ICC) of 0.13 and a baseline prevalence of 62.8%, and assuming a reduction in cumulative incidence at the 6-month follow-up of 25% in the control group (albendazole chemotherapy only), based on the reported impact of MDA campaigns in neighbouring countries,54–56 we estimated a control-group cumulative incidence of 47.25%. Our baseline data indicated an average cluster size of 125 people, of whom 120 would participate but only 100 provide stool samples, and we estimated a subsequent 10% loss to follow-up. To determine whether the WASH programme results in a 50% reduction of the follow-up cumulative incidence compared with the control group (ie, to 23.63%), with a power of 80% and α=0.05, based on the baseline data, we would need 8 clusters in each arm rather than 12. We therefore expect to have sufficient power (>80%) to achieve the study aims with regard to N. americanus. This is largely because the baseline prevalence was higher than expected, and the ICC was lower than expected.
Note that sample size calculations were based on impact, not at the 2-year end point but at the first midpoint, since there were no data available that allowed for an estimation of the effect of the interventions over a 2-year period. Furthermore, our choice of estimate of impact had the following rationale: (1) it would not be logistically feasible in our setting to run a trial capable of detecting smaller intervention effects (eg, it would require a number of clusters that exceeds implementation capacity of WaterAid) and (2) we believe that the scale-up of WASH interventions as tools for STH control is not likely to occur if there is not a sufficiently large benefit compared to the MDA only.
Selection of communities and randomisation
WaterAid works from the Timor-Leste government's district water infrastructure plan, which includes all villages that require assistance with water facilities, and prioritises them according to need. Each year, WaterAid holds a workshop with government ministries and the local district and subdistrict officials, to agree on a priority list of communities to be supported by WaterAid in the forthcoming year.
This annual meeting established the sampling frame using the following criteria.
Inclusion criteria
Rural communities in Manufahi district that were suitable to receive water infrastructure development (ie, having a water source such as a spring from which clean water can be distributed to the community).
Manufahi district communities identified as ‘priority communities’ for receiving the hygiene and sanitation programme (ie, having poor access to clean water and sanitation, and demonstrating local commitment to hygiene and sanitation improvement).
Exclusion criteria
Communities that had been previous recipients of the WaterAid programme.
Communities that had been recipients of deworming programmes (school or community based) in the previous 10 years.
Communities that had more than 50% coverage with household latrines.
To meet the needs of the participant communities, all of which have been identified as priority communities for receipt of the intervention, all clusters included in the control arm will receive the WASH programme at the end of the study. Thus, we have used a delayed intervention design for this study.
Feasibility assessments
WaterAid conducts 1–2 days visits to the communities of the priority list agreed with the district officials to perform feasibility studies, that is, to assess, in loco, the eligibility of each community. The visits include meetings with local leaders (village or subvillage chief), and inspection of the area to determine the community size, the population, the water source location, type and size and sanitation status.
Three rounds of feasibility assessments were made by WaterAid and partner local NGOs: one in early 2012 for identification of the first eight communities; a second in early 2013 for identification of the remaining 16 clusters; and a third round of feasibility studies had to be done in August 2013 to identify four additional replacement communities to complete the enrolment of the last group of clusters, as explained below (figure 2).
Allocation and enrolment
Each year, the clusters in the list of 8 and 16 that were provided by WaterAid, were randomised by the trial investigators to the intervention and control arm using an electronic random number generator, and they were enrolled in the following three batches/time periods: the first eight clusters were enrolled between May and October 2012; the second group of eight clusters were enrolled between April and July of 2013, and the final eight were enrolled between August and October of 2013 (figure 2). Unfortunately, five (2 interventions, 3 controls) of the selected communities were excluded during the enrolment process, due to not meeting the necessary criteria namely: one intervention community had an unsuitable water source; one control due to high risk of contamination was given proximity to two intervention clusters; one control was not willing to comply with the 2-year waiting period to receive the WASH intervention; one control due to its small size; and one intervention was not willing to voluntarily cooperate with WaterAid and the implementation partners in building the water system. Additionally, two intervention and two control clusters were replaced given that the originally selected clusters did not meet the inclusion criteria: one intervention and one control cluster were deemed too close, thus posing high risk of contamination; another control had high latrine coverage, and the other intervention community was targeted by the government to receive a water intervention. The replacement clusters were randomly allocated to the intervention and control arms from a replacement list of four communities assessed by WaterAid.
During the follow-up period, one of the intervention communities withdrew due to the fact that the previously identified water sources were deemed to have an insufficient water debit for WaterAid to implement the planned water intervention. Furthermore, one intervention cluster was reduced in size given that at the time of the implementation of the water intervention, the water source no longer had capacity to provide water to the entire community, but was enough to provide water to one of the four hamlets that comprised that initial cluster.
Engagement and recruitment
The WASH for WORMS research team accompanied WaterAid and their local partners during the ‘triggering’ event. Once at the community, the trial was initially discussed with community leaders: the objectives and design of the study were explained to them, and their support and commitment was sought. At the end of the ‘triggering’ meeting, where community members are assembled at a central location (a school, health centre or house of the community leader), the WASH for WORMS trial was explained to the assembly, facilitated by the trial staff, assisted by community leaders and WaterAid staff. The GMF committee elected in each cluster by the community, as per WaterAid suggestion, was recruited to also work as the Community Advisory Committee (CAC) for the research study. In control communities, a similar approach was implemented by the trial field team (initial meeting with the community chief, followed by community assembly and election of CAC).
Baseline parasitological surveys were then conducted in each community. The timing of these surveys depended on the villagers’ availability, and did not exceed 3–4 weeks after the ‘triggering’ event, so that it happened before residents started building latrines. When possible, the survey happened the week immediately after the ‘triggering’ and CAP events took place. This was staggered over an 18-month period in 2012 and 2013, due to WaterAid implementation capacity, and, to avoid temporal confounding due to seasonal variation in transmission of gastrointestinal parasites, surveys conducted in intervention communities were alternated with surveys conducted in control communities. All members of the selected communities (over 1 year of age) were eligible for inclusion in the trial at baseline, provided that they, or a parent or guardian, were able to provide informed consent. During the follow-up visits, new residents or babies who turned 1 year, were invited to participate. The name and date of birth of each resident was recorded for each household on standardised registration forms, and this information was used to identify participants at each of the follow-up surveys.
Data collection
Specimen collection and processing
During the house-to-house visit, each participant is given a plastic container and asked to return the following morning with a sample of their faeces from that morning. Ideally, this is timed such that faecal samples are provided to the survey team within 4 h of collection. Instructions are given to parents on how to obtain faecal samples from their young children. The process is identical for intervention and control arms, and is being repeated at each of the four follow-up surveys.
Each faecal sample is separated into 2–3 mL aliquots (equating to approximately 2–3 g), and preserved in 15 mL centrifuge tubes, previously filled with 8 mL of 10% formalin or 6 mL of 5% potassium dichromate for microscopy or molecular analysis, respectively.54–57 The samples are transported to the National Laboratory, Dili, Timor-Leste and to the Queensland Institute for Biomedical Research, Brisbane, Australia, for diagnostic processing for microscopy and PCR. Identification and quantification of STHs and oocysts of protozoan parasites by microscopy were carried out using a flotation technique, and was done for the first eight clusters only.58 In addition to this, all faecal samples are subjected to detection and genetic identification using PCR. DNA extractions are carried out using the PowerSoil DNA extraction kit (Mo Bio), with modifications.59 Each sample is subjected to two real-time multiplex PCRs modified from a previously described technique, to detect and quantify the STH (Ascaris spp, N. americanus, Ancylostoma spp and T. trichiura), and detect S. stercoralis and protozoa (E. histolytica, G. duodenalis and Cryptosporidium spp).60 ,61 Those samples positive for Ancylostoma spp will be further subjected to a Sequenom MassARRAY SNP Genotyping platform (Sequenom, Inc) assay to differentiate species of Ancylostoma (A. duodenale, A. ceylanicum and A. caninum) (Llewelyns, personal communication, 2013).
Anaemia assessment
At baseline and each annual follow-up, blood samples are obtained from each participant by the fingerprick method, and Hb concentration is assessed using a portable analyser (Hb 201+, HemoCue, Angelholm, Sweden). Anaemia will be defined as per WHO classification for each age group.62 Hb levels will be adjusted for altitude for the surveyed communities situated above 1000 m.63
Anthropometrics
The height and weight of children aged <18 years are also measured by the WASH for WORMS field team, that includes one nurse. Each child is measured for height or length to the nearest 0.1 cm, using a Portable Height Rod (Wedderburn, WSHRP) for children aged 2 years or older and able to stand, or a measuring mat (Wedderburn, SE210) for children under 2 years of age. Weight is measured to the nearest 0.1 kg, using a digital scale (CAMRY, ED-301); in the case of children under 2 years of age or unable to stand, tared weighing is used. These measurements, taken as single measurements (along with age), will be used to calculate anthropometric indices used as proxies for malnutrition in children: weight-for-age (also known as underweight), height-for-age (also known as stunting), weight-for-height (also known as wasting) and body mass index (BMI)-for-age (also known as thinness).64 Results for all anthropometric indices will be computed as Z-scores (number of SDs in relation to the mean of the standard population); the value of −2 Z-scores was used as the critical point below which to define malnutrition, while values below −3 Z-scores were defined as severe malnutrition.64 Z-scores will be constructed using the 2006 WHO (Geneva, Switzerland) database for child growth standards. Weight-for-age Z-scores will be calculated for individuals 1–10 years of age; height-for-age and BMI-to-age Z-scores will be calculated for individuals 1–18 years of age, while weight-for-height Z-scores will be calculated for individuals 1–5 years of age. Z-scores will also be stratified by age, considering the following age groups: 1–2 years of age, above 2 to under 5 years of age (preschool-age children), 5–10 years of age, 10 to under 15 years of age, and 15 to under 18 years of age as applicable, to reflect critical periods of growth.65
Assessment of potential risk factors for STH infection and confounders
WASH for WORMS field workers were trained to interview participants using questionnaires asking about defaecation practices (including observation of the household latrine if it exists); disposal of faeces practices; availability of water, soap and latrines; household assets; education; occupation; treatments with antiparasitic drugs; and history of diarrhoea. These variables will be included in the regression models. Questions relating to water, sanitation and hygiene will be used as measures of the intervention uptake and compliance, and taken into account when interpreting the results of the trial. Questionnaires are administered at community (interview with the community chief), household (interview with the female head preferentially) and individual level. When participants were younger than 12 years of age, the caregiver answered the questionnaire in the presence of the child.
Analysis of the trial data
Study outcomes will be calculated and compared across both arms of the trial, with the study end points measured after 2 years of follow-up, and midpoints assessed at 6-monthly intervals or, for specific secondary outcomes, 12-monthly intervals.
Analyses will be initially based on generalised linear mixed models to account for within and between cluster variability. If there is the need to adjust for confounding or differences in the baseline characteristics of the intervention and control groups, variables measured in the study questionnaires by the WASH for WORMS team will be incorporated as covariates, allowing an adjusted effect estimate to be calculated for the intervention as follows: for cumulative incidence, Bernoulli logistic regression models will be developed with the infection status of the individual as the outcome, age and sex entered as covariates, and the household and community as random effects; adjustment for baseline prevalence and malnutrition status will involve entering baseline prevalence and z-scores as fixed effects in the models, and the intervention will be entered as a binary fixed effect to estimate differences in cumulative incidence, and OR of infection, between the two arms at each follow-up survey. Given an expected high cumulative incidence, OR may be biased away from the null, and therefore, calculations will be complemented by estimating the cumulative incidence ratio (CIR) using either a log-binomial model or a modified Poisson model. Calculating both parameters will contribute to advancing evidence on the legitimacy of using OR or CIR as estimates of relative risk.66 ,67 Intensity of infection of the STH (Ascaris spp, Ancylostoma spp, N. americanus and T. trichiura) will be determined by a formula based on the log-transformation of individual Ct values, and will be expressed as eggs per gram of faeces, and will be modelled with random and fixed effects as described for the cumulative incidence analysis. Anthropometric Z-scores and mean Hb concentration, measured as continuous outcomes, will be modelled using mixed-effects linear regression. All analyses will be conducted using Stata software68 and will not be blinded. Analysis of the trial outcomes will be based on the 18 communities (10 interventions and 8 controls) that were randomly allocated and remained in the study.
Understanding the planning and implementation of the sanitation component, as well as the barriers and enablers associated with the acceptability and uptake of the WASH programme
We will examine the planning and implementation of the sanitation component of the intervention, as well as the factors acting at individual and community levels that influence acceptability and uptake of the community-based WASH programme, using a mix of qualitative and quantitative methods.
Interpretations of Community-Led Total Sanitation in Manufahi, Timor-Leste: The objective of this qualitative investigation is to compare the theoretical basis of CLTS, as described by its founders, with descriptions of CLTS and how it is implemented in Timor-Leste. Data was collected through interviews with 19 key informants, representative of the different groups involved in planning and implementing WASH interventions in Manufahi: members of the relevant government ministries in Timor-Leste, WaterAid staff, facilitators of the triggering events, and residents of two communities in Manufahi which have undergone the WaterAid WASH programme. The interview questions relate to how the participants define the critical aspects of CLTS, as well as how they think the CLTS-inspired sanitation interventions should be and are currently being implemented in Timor-Leste. Interviews will be transcribed and data will be coded around the main topics of the interview guide. Key themes will be drawn out and analysed thematically.
Changes in Knowledge, Attitudes and Practices (KAP) among household representatives participating in the WASH programme: Using quantitative methods, we aim to identify the changes in community members’ KAPs regarding sanitation since undergoing the WASH programme. Data were collected through a KAP survey of household representatives in three participating clusters, at three points in time, aiming to have 60 participants complete the three surveys, which will allow to detect percentage changes of 30% or more. Changes will be identified in relation to the triggering process, specifically: up to 1 month prior; up to 1 week after; and 9–11 months after the triggering process. The primary analysis will assess changes in the proportion of households with each item of KAP at each time point. The results for each community will also be processed separately using principal component analysis, a procedure which compresses potentially correlated variables (in this case, changes in KAPs across time) in order to identify patterns in the overall data.
Barriers and enablers associated with the acceptability and uptake of the sanitation intervention: The objective of this qualitative substudy is to identify the salient influences on household WASH decisions and behaviour, in particular, whether households construct a toilet, and/or become open defaecation free, following participation by their community in the WaterAid WASH programme. Data was collected through interviews with the community leader from two communities which have participated in the WASH programme for at least 1 year; household representatives from the same cluster (up to 10 in each community); a field staff member from WaterAid and WASH for WORMS (one each) who work in the two clusters. The households were selected purposively from lists provided by the WASH for WORMS team and WaterAid, and included households which have built a toilet and are open defaecation free; have built a toilet but are not open defaecation free; and, have neither built a toilet nor become open defaecation free. Where possible, diversity of household vulnerability was sought within these categories, where vulnerability will be limited to (1) female-headed households and (2) households which include a person living with a disability. The participants were asked open-ended questions pertaining to the series of events which took place in relation to the WaterAid and WASH for WORMS activities in the community; the decisions and behavioural change that occurred within households as a result of these events; and the reasons offered for these decisions and behavioural change. Interviews will be transcribed, and data will be coded around the main topics of the interview guide. Key themes will be drawn out and analysed thematically.
Ethics and dissemination
Written consent for participation in the study was obtained from each participant aged ≥18 years and from the parents/guardians of children aged <18 years, during house-to-house visits to each household. In addition, written assent was sought from individuals aged 12–17 years inclusive. For illiterate participants, an ink thumb-print was used in lieu of a signature.
The results of the study will be published in peer-reviewed journals, presented at national and international conferences, and discussed with the Timorese Ministry of Health. The results of this research will provide evidence on the benefits of intersectoral collaboration between the health and the WASH sectors, in order to achieve more effective and sustainable disease control, and therefore, will be disseminated to relevant stakeholders in disease control and WASH programmes, including WHO and international NGOs. Tools used for the implementation of this study (ie, questionnaires and protocols), as well as data collected and the analysis scripts, will be made available to the scientific community on request, after the publication of the trial results.
Acknowledgments
The authors would like to acknowledge the Ministry of Health of Timor-Leste for the albendazole distributed in the trial; the WASH for WORMS’, WaterAid's and their partner's field staff for carrying out work in the field; Darren White for his contribution to improving field procedures, and the communities for participating in the trial.
References
Footnotes
Contributors SVN was responsible for revising and implementing the study protocol, and drafted the manuscript. JSM, RT, RMA, JB, DG, AV, MM and GW participated in designing the study. AC codrafted the manuscript. EW is responsible for the implementation of the WASH intervention protocol. J-AA drafted study protocols. SC and NC are major contributors to the development of questionnaires for aims 1/2 and 3, respectively. All the authors contributed to editing and revising the manuscript.
Funding This study is funded by a Partnership for Better Health—Project grant from the Australian National Health and Research Council (NHMRC) (APP1013713). DG holds a NHMRC Career Development Fellowship (APP1090221); AC holds a NHMRC Senior Research Fellowship (APP1058878).
Ethics approval Ethics approval was obtained from the University of Queensland Human Research Ethics Committee (project number 2011000734); the Australian National University Human Ethics Committee (protocol: 2014/311); the Timorese Ministry of Health Research and Ethics Committee (reference 2011/51); and the University of Melbourne Human Research Ethics Committee (reference 1339348).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.