Article Text

Abstract
Objectives Low back pain (LBP), from degenerative lumbar spine disease, represents a significant burden on healthcare resources. Studies worldwide report trends attributable to their country's specific demographics and healthcare system. Considering England's specific medico-socioeconomic conditions, we investigate recent trends in hospital admissions and procedures for LBP, and discuss the implications for the allocation of healthcare resources.
Design Retrospective cohort study using Hospital Episode Statistics data relating to degenerative lumbar spine disease in England, between 1999 and 2013. Regression models were used to analyse trends.
Outcome measures Trends in the number of admissions and procedures for LBP, mean patient age, gender and length of stay.
Results Hospital admissions and procedures have increased significantly over the study period, from 127.09 to 216.16 and from 24.5 to 48.83 per 100 000, respectively, (p<0.001). The increase was most marked in the oldest age groups with a 1.9 and 2.33-fold increase in admissions for patients aged 60–74 and ≥75 years, respectively, and a 2.8-fold increase in procedures for those aged ≥60 years. Trends in hospital admissions were characterised by a widening gender gap, increasing mean patient age, and decreasing mean hospital stay (p<0.001). Trends in procedures were characterised by a narrowing gender gap, increasing mean patient age (p=0.014) and decreasing mean hospital stay (p<0.001). Linear regression models estimate that each hospital admission translates to 0.27 procedures, per 100 000 (95% CI 0.25 to 0.30, r 0.99, p<0.001; r, Pearson's correlation coefficient). Hospital admissions are increasing at 3.5 times the rate of surgical procedures (regression gradient 7.63 vs 2.18 per 100 000/year).
Conclusions LBP represents a significant and increasing workload for hospitals in England. These trends demonstrate an increasing demand for specialists involved in the surgical and non-surgical management of this disease, and highlight the need for services capable of dealing with the increased comorbidity burden associated with an ageing patient group.
- NEUROSURGERY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The use of routinely collected national administrative data allowed for the analysis of trends in admissions and surgical procedures for low back pain (LBP) throughout England, for a prolonged time period.
As Hospital Episode Statistics is collected independently of this study, it is not subject to study-related bias or affected by factors that may have influenced hospital trends in LBP.
This study provides important England-specific population-level data about longitudinal trends, associations and patterns of care for LBP.
Limitations inherent to using aggregate administrative data include coding errors relating to inaccurate representation of admissions and procedures, data duplication and interhospital variability.
Introduction
Low back pain (LBP), from degenerative lumbar spine disease, is one of the most prevalent non-fatal conditions worldwide, and a significant cause of long-term disability.1 ,2 In England, it is one of the leading causes of physician attendances, hospitalisation and utilisation of social care services.3 It confers a significant economic burden in terms of funding of health resources, disability benefits and effect on industry from sick leave.3
Several studies in other countries, using national and medical insurance databases, have identified interesting trends in hospitalisation for degenerative lumbar spine disease. These trends have been attributed to the country’s specific healthcare system, demographics, medical technological advances, and profitability of treatment modalities.4–9 There is sparse data on trends in hospitalisation for this disease in England.
The aim of this study is to investigate the longitudinal trends in hospital admissions and surgical procedures for degenerative lumbar spine disease in England, between 1999 and 2013. Considering England’s specific medico-socioeconomic conditions, which include the existence of a health service free at the point of delivery, we evaluate whether it follows trends seen in other countries, and discuss the implications for allocation of healthcare resources.
Methods
Annual aggregate data for all hospital admissions and procedures in England, from 1999 to 2013, were retrieved from Hospital Episode Statistics (HES), available from the Health and Social Care Information Centre.
In this study, the term LBP refers to degenerative disease resulting in LBP with or without radicular or neurogenic claudicant symptoms. This encompasses a variety of underlying processes including herniated disc disease, isthmic/degenerative spondylolisthesis, spinal stenosis and non-specific LBP (back pain not attributable to spinal instability or associated with radicular symptoms). Surgical procedures refer to surgery for degenerative lumbar spine disease, and do not include surgery for non-degenerative pathology such as trauma or malignancy.
The HES data set groups primary diagnoses according to the World Health Organization’s 10th revision of the International Classification of Diseases. The codes relevant to our study were M54.1, M54.3, M54.4 and M54.5, referring to admissions with the primary diagnosis of radiculopathy, sciatica, lumbago with sciatica and LBP, respectively. Finished consultant episodes, representative of hospital admissions, were analysed with respect to gender and four different age groups (0–15, 16–59, 60–74 and ≥75 years).
Primary procedures, defined as the most resource intensive procedure performed during the hospital episode, were identified using to the fourth version of the Office of Population Censuses and Surveys Classification of Interventions and Procedures. Codes representing surgical procedures relevant to degenerative lumbar spine disease (see online supplementary appendix) were aggregated and analysed to produce admission trends stratified by age and gender. The data for 1999 were excluded from our analysis of surgical interventions as only the less detailed three-character procedure codes were available, deemed insufficient for this study.
Mid-year estimates of English population denominators grouped by age and gender were obtained from the Office of National Statistics. Annual hospital admissions and surgical interventions are reported per 100 000 of the population, and further stratified by broad age groups and gender.
Time trends were investigated using linear regression models with the gradient expressed as β values with 95% confidence intervals, per 100 000 of the population. Correlation is represented by Pearson’s correlation coefficient (r). Continuous variables were compared using the independent samples t test. A p value of <0.05 was chosen to imply statistical significance. Statistical Package for the Social Sciences was used to perform data analysis.
This study is exempt from UK National Ethics Committee approval as it analyses freely available anonymised aggregate data used for administrative purposes.
Results
Trends in hospital admissions for LBP
Overall hospital admissions
Over the 15-year period from 1999 to 2013, there was a significant rise in the overall hospital admissions for LBP, increasing from 127.09 in 1999 to 216.26 in 2013, per 100 000 population (figure 1). This represents a 1.7-fold increase or an annual increase of 7.63/100 000 (β 7.63 (CI 6.75 to 8.50), r=0.98, p<0.001).

Hospital admissions for low back pain in England, 1999–2013. Solid line—admissions per 100 000 population, dashed line—linear regression model.
Gender
Hospital admissions for men and women increased over the 15-year period (β 4.97 (CI 4.33 to 5.61) and 10.22 (CI 9.1 to 11.35) respectively, r=0.98 for both, p<0.001), with admissions being significantly greater in women than in men (p<0.001) (figure 2). Hospital admission rates for women increased at approximately twice the rate of men’s, resulting in a widening gender gap over the 15-year period (p<0.001).

Male and female hospital admissions for low back pain, 1999–2013. Solid lines—admissions per 100 000 population, dashed lines—linear regression model.
Mean age of patients at admission
Age at admission increased from 52.5 years in 1999 to 56.5 years in 2013, representing an estimated 0.28 year increase in the average patient age per annum, over the 15 years (β 0.28 (CI 0.21 to 0.34), r=0.93, p<0.001).
Age categories
The data demonstrates a significant increase in hospital admissions for each of the four age groups over the study period (p<0.001) (figure 3). The greatest increase is seen in those aged 60–74 and ≥75 years, evident by a 1.9 and 2.33-fold increases, respectively, (from 199.43 to 379.34, and from 209.96 to 488.60, per 100 000, respectively). Hospital admissions for those aged 0–14 years increased from 3.99 to 6.39 per 100 000, representing a 1.6-fold increase in a paediatric population, and from 140.11 to 200.8 per 100 000 for patients aged 15–59 years, over the 15 years. The older the age group the greater was the observed annual rate of increase in hospital admissions (p<0.001) (figure 4).

Hospital admissions for low back pain in England by age groups, 1999–2013.
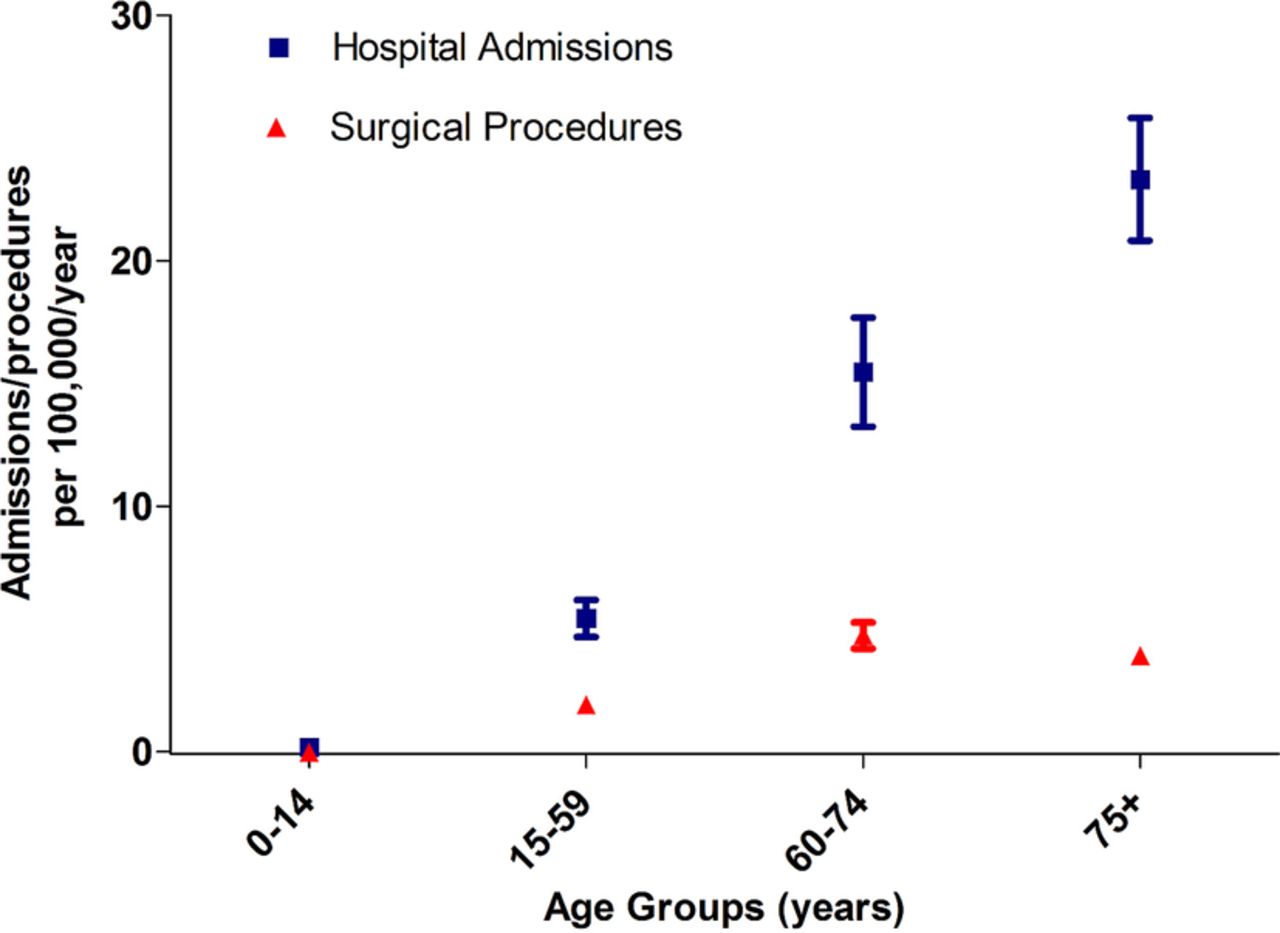
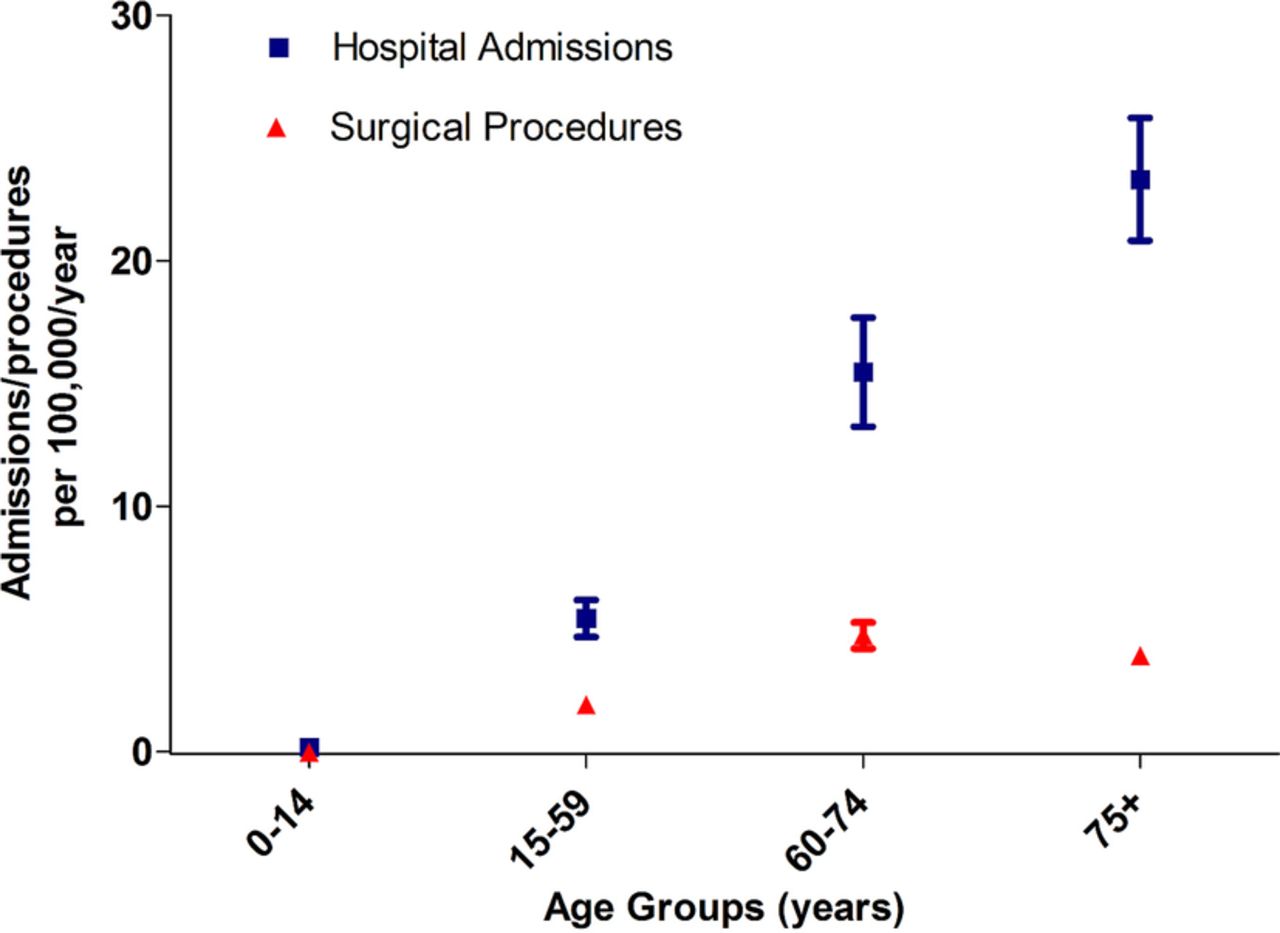
Age specific annual rate of increase in hospital admissions and procedures, 1999–2013. Values correspond to each age group’s β coefficient with their respective 95% CIs represented as error bars.
Mean hospital stay
The average length of hospital stay decreased from 5.7 days in 1999 to 2.7 days in 2014, representing a 52% decrease or a fall of 0.25 years per study year (β 0.25 (CI −0.21 to −0.29), r=0.96, p<0.001).
Trends in surgical procedures for degenerative lumbar spine disease
Overall surgical procedures
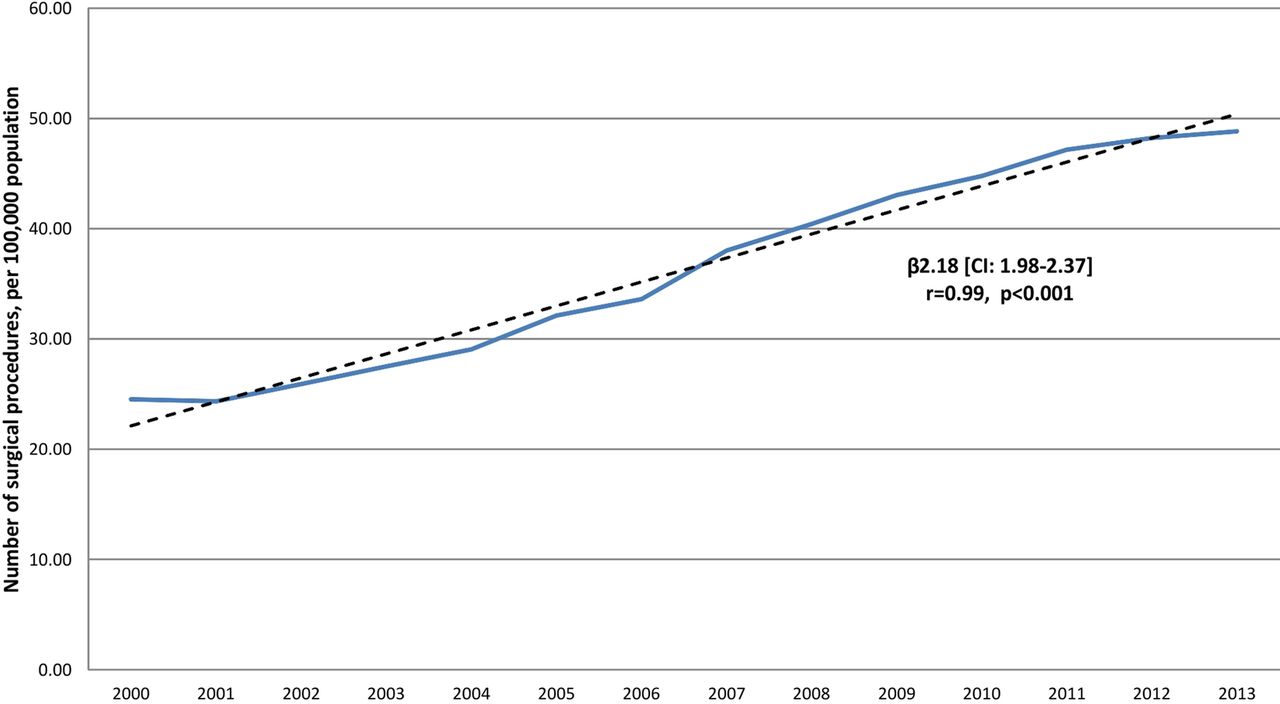
Over the study period, there was a significant increase in the overall number of surgical procedures performed for degenerative lumbar spine disease (figure 5). Recorded procedures almost doubled from 24.5 to 48.83 per 100 000, with an estimated 2.18/100 000 increase each year (β 2.18 (CI 1.98 to 2.37), r=0.99, p<0.001).

The number of surgical procedures performed for degenerative lumbar spine disease, 2000–2013. Solid line—number of procedures per 100 000 population. Dashed line—linear regression model.
Association between hospital admissions and the number of surgical procedures
There was a strong positive linear correlation between hospital admissions and procedures, with every incremental admission translating to an estimated 0.27/100 000 increase in surgical interventions (β 0.27 (CI 0.25 to 0.30), r=0.99, p<0.001).
Gender
There was a significant increase in surgical procedures for both genders over the study period (p<0.001). There was a statistically significant difference between genders for the early years only (2000–2003, p=0.01), but not for the latter years (2011–2013, p=0.73), suggesting a narrowing of any early gender gap.
Mean patient age
This increased from 49.4 in 2000 to 52.3 years in 2013 (p=0.014), with an estimated increase in mean patient age of 0.2 years per annum, over the study period (β 0.20 (CI 0.14 to 0.27), r=0.8, p<0.001).
Age categories
With the exception of patients aged 0–14 years, there was a significant increase in the uptake of surgery for all age groups (15–59, 60–74 and ≥75 years, p<0.001) (figure 6). The most significant increases were seen in the oldest age groups, with a 2.8-fold increase in those aged 60–74 and ≥75 years over the study period (from 32.54 to 89.95 and from 24.89 to 70, per 100 000, respectively). In contrast, those aged 15–59 years demonstrated a 1.7-fold increase (30.21 to 50.22 per 100 000). There was a fall in the number of surgical procedures recorded for those aged 0–14 years, from 0.67 in 2000 to 0.29 in 2014 per 100 000 (p=0.007).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of surgical procedures for degenerative lumbar spine disease by age groups, 2000–2013.
The rate of increase was greatest for patients aged ≥60 years, with patients aged 0–14 years demonstrating a slowly falling trend (0–14 years: β −0.02 (CI −0.01 to −0.04), r=−0.68; 15–59 years: β 1.9 (CI 1.65 to 2.15), r=0.98; 60–74 years: β 4.73 (CI 4.19 to 5.27), r=0.98; ≥75 years: β 3.9 (CI 3.57 to 4.23), r=0.99; p<0.01 for all groups) (figure 4).
Mean hospital stay
The mean hospital stay for those undergoing surgery decreased from 8.26 to 3.58 days over the study period, representing a 57% decrease or a fall of 0.39 days per study year (β −0.39 (−0.36 to −0.42), r=−0.99, p<0.001).
Discussion
This study identified significant increases in hospital admissions and procedures for degenerative lumbar spine disease in England, between 1999 and 2013. The findings are, in general, concordant with studies from other countries.4–9 The results reveal a widening gender gap, with women accounting for an increasingly greater proportion of hospital admissions. Interestingly, this has not translated to a similar trend in surgical procedures, where any gender gap in the early years is decreasing, in direct contrast to studies from other countries.5
This suggests that although more women are admitted for LBP, they appear to be managed non-surgically. It is also possible that the gender gap may be related to gender-specific coding inconsistencies: for example, gynaecological flank pain incorrectly coded as lumbago or LBP. Considering that this data mirrors trends identified in other countries, this is less likely. Further investigation into trends in specific surgical procedures may identify procedure-specific gender gaps not revealed when analysing aggregate surgical procedures.
As with other surgical trends in England, in the context of an ageing population, there has been a shift in the burden of this disease to the oldest population groups (60–74 and ≥75 years), resulting in an increase in the mean patient age for hospital admissions and surgical interventions.10–12 Unexpectedly, over the same period, the average hospital stay has halved. Although the data do not allow us to address the underlying reasons for this, it may be attributable to improved perioperative care (such as high risk anaesthetic clinics optimising patients prior to surgery), and improved postoperative therapy and social care, allowing for earlier patient mobilisation and discharge; or possibly, the result of the recent paradigm shift towards moving care into the community with better community services for chronic conditions.
Our observation of an ageing patient group and falling mean hospital stay is well established in the international literature.5 ,9 ,13 There is, however, a well described increase in the burden of comorbidities associated with increased rates of postoperative complications and mortality in older patients.5 ,14 ,15 Further analysis of trends in age-specific mortality and morbidity for lumbar spine surgery in England may better reflect the true burden of this disease on hospital resources, as the significantly shorter stay by younger patients may have skewed the data. An advancing mean patient age has important implications for provision of critical care resources, and demand for medical specialties involved in managing the increased comorbidity burden.
The data identify an under-appreciated trend in increasing hospital admissions for patients aged 0–14 years. Although the data cannot identify the underlying reasons, it may be attributable to the rising obesity levels in children.16 LBP is less well recognised in this age group, and consequently, health resources are relatively suboptimal.17 The data suggest growing demand and indicate the need for provision of paediatric services to manage the underlying causes in an effort to attenuate current trends.
This study estimates that for every 100 patients being admitted with LBP, approximately 27 undergo surgical intervention (β 0.27 (CI 0.25 to 0.30), r=0.99, p<0.001). Regression models looking at hospital admissions and surgical procedures separately (figures 1 and 5), illustrate that admissions are increasing at 3.5 times the rate of surgical interventions (β values of 7.63 vs 2.18, respectively). This highlights a disproportionate growth in demand for those involved in the non-surgical management of LBP, such as therapists and pain specialists, and indicates that more funding might be needed in the future for these services. A proportion of this difference may be attributable to a lack of surgical capacity to deal with the increasing workload. Further analysis of waiting lists and mean waiting times may elucidate the factors accounting for this observation.
Current guidelines regarding non-surgical management recommend considering structured supervised exercise programmes, manual therapies and acupuncture in patients with non-specific LBP.18 The medical literature regarding their effectiveness is complicated by the heterogeneous nature of these treatment modalities and the patient population, with pooled analyses and systematic reviews demonstrating, at best, a modest benefit.19 ,20 Considering the trends identified in this study, it would be prudent to increase funding into high level research (with sufficient long-term follow-up) aimed at identifying the relative effectiveness of non-surgical treatment modalities in different patient groups, so that resources may be optimally allocated to match the increasing future demand for these services, and reduce hospital burden.
Limitations inherent to using aggregate administrative data include coding errors relating to inaccurate representation of admissions and procedures (eg, lumbar fixation for trauma being incorrectly counted in the codes selected for this study), interhospital variability, data duplication, and discrepancy between finished consultant episodes and admissions. Considering the size of the data set and duration of this study, any systematic error is likely to have evened out, especially when investigating trends rather than absolute values. Furthermore, systematic reviews have demonstrated a good correlation between reported and actual validated data, reporting coding accuracies between 83 and 92%, which is sufficient for use in this study.21 ,22 Finally, the trends identified in this study not only reflect those found in other countries, but also mirror patterns seen in other surgical pathologies in England that have been subject to similar changing demographics, surgical innovation and changes in health guidelines.4–6 ,8–12
Although this data do not directly address the underlying reasons for the observed trends, over the past 15 years, there have been numerous factors that may have influenced hospital trends for degenerative lumbar spine disease in England. These include demographic changes such as an ageing population, rise in obesity, sedentary lifestyles, public health factors such as changes in health guidelines, and surgical factors such as advancements in diagnostic imaging and proliferation of spinal instrumentation and implant systems.7 ,23
Conclusion
LBP, from degenerative lumbar spine disease, represents a significant and increasing workload for hospitals in England. The strong trends and associations identified in this study demonstrate an increasing demand for specialists involved in the surgical and non-surgical management of this condition. It highlights the need for the provision of services capable of dealing with the increased comorbidity burden associated with an ageing patient group. An under-appreciated trend in increasing admissions for patients aged 0–14 years is identified, prompting the need for research into underlying causes, and the provision of appropriate paediatric services to attenuate this adverse finding.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors VS conceived and designed the study, analysed and interpreted the data, drafted the article, made appropriate revisions and approved the final version of the manuscript. HCP provided statistical analysis, and critically reviewed and revised the original draft, and approved the final version. BAO assisted in the interpretation of the data, critically reviewed and revised the manuscript, and approved the final version. MCP is the guarantor and assisted in the conception of the study, critically reviewed the manuscript, and approved the final version. All authors agree to be accountable for the study.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval This study is exempt from UK National Ethics Committee approval as it analyses freely available anonymised aggregate data used for administrative purposes.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.