Article Text

Abstract
Objective The abdominal drawing-in manoeuvre (ADIM) is a common clinical tool for manually assessing whether a preferential activation of the deep abdominal muscles in patients with low back pain (LBP) is ‘correct’ or not. The validity and reliability of manual assessment of the ADIM are, however, as yet unknown. This study evaluated the concurrent and discriminative validity and reliability of the manually assessed ADIM.
Design Single-blinded cross-sectional study.
Settings General population in Stockholm County, Sweden.
Participants The study sample comprised 38 participants seeking care for LBP, and 15 healthy subjects.
Measures The manual ADIM was assessed as correct or not following a standard procedure. Ultrasound imaging (USI) was used as the concurrent reference (gold standard) for the manually assessed ADIM by calculating a ratio of the change in muscle thickness between the resting and the contracted states: the correlation between manual test and USI was calculated. Discriminative validity was analysed by calculating sensitivity and specificity. A sample of 24 participants was analysed with κ coefficients for interobserver reliability between two raters.
Results The concurrent validity between the manual ADIM and the ADIM–USI ratios showed poor correlations (r=0.13–0.40). The discriminative validity of the manually assessed ADIM to predict LBP showed a sensitivity/specificity of 0.30/0.73, while the ADIM–USI ratio to predict LBP showed 0.19/0.87. The interobserver reliability for the manually assessed ADIM revealed substantial agreement: K=0.71, CI (95%) 0.41 to 1.00.
Conclusions Although the interobserver reliability of the manually assessed ADIM was high, the concurrent and discriminative validity were both low for examining the preferential activity of the deep abdominal muscles. Neither the manually assessed ADIM nor the ultrasound testing discriminated between participants with LBP and healthy subjects regarding preferential activity of the transversus muscle as this ability/inability was also present in healthy subjects.
- REHABILITATION MEDICINE
- ULTRASONOGRAPHY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The abdominal drawing-in manoeuvre was analysed for both concurrent and discriminative validity and that the investigators were blinded to the health status of all the participants.
The study used a gold-standard tool (ultrasound) to measure the quantity of muscle activity for comparison with the manual estimation.
Our study design resulted in a disproportionate sample between healthy subjects and those with low back pain.
In addition, the patients estimated their low back pain only as low-to-moderate.
Introduction
The lumbar spine depends on complex interactions between passive and active structures such as contracting muscles, ligaments and fascia, to maintain optimal spinal control during bodily movement and loading.1–3 Contraction of the lateral abdominal muscles, and especially the anticipatory activity of the transversus abdominus muscle (TrA), has been suggested to be a key motor-control element for transferring spinal loads to the pelvis and upper trunk, thus avoiding injury to spinal tissue or pain following subfailure loading.2–5
Studies have reported delayed anticipatory activity of TrA in low back pain (LBP) sufferers in comparison to healthy subjects,5–7 although such differences in temporal activity have also been questioned.8 Specific exercises have been proposed for re-training motor control of the abdominal muscles; a popular and common treatment for people with recurrent and chronic LBP.9 ,10 Following such interventions, recent systematic reviews have reported improvement of symptoms such as pain and functional deficits compared to other exercises or treatment.11 ,12
To assess the activity of the deep abdominal muscles, a specific clinical test is available: the abdominal drawing-in manoeuvre (ADIM).13 Through manual palpation and visual inspection, the ADIM is used to assess the success or not in performing a voluntary and preferential contraction of the deep abdominal muscles, especially the TrA,13 ,14 in order to target interventions with specific exercises and follow-up progression.
In addition, ultrasound imaging (USI) has for several years been used in clinical settings to quantify the activity of the deep abdominal muscles. Specifically, it has also been used in research to quantify change in muscle thickness or muscle onset of TrA before and after interventions using motor control exercises.15 The USI has been validated for measuring change in muscle thickness against electromyography (EMG)16 and MRI,17 and demonstrates high interobserver reliability in healthy people and in patients with LBP.14 ,18–21 However, not all clinicians have access to USI and the manually assessed ADIM therefore remains the most common clinical tool for addressing and examining a preferential contraction of the deep abdominal muscles.
A clinically convenient test should show both good reliability and high validity. Specifically, it should be able to demonstrate concurrent validity against a reliable gold-standard assessment (eg, USI verifying TrA activity); proved to measure what it purports to measure.22 If the clinical test is to reflect impairment, and not merely normal variation in healthy subjects, it should also exhibit empirical, discriminative validity to justify its use among patients.23 For the present purpose, discriminative validity was defined as the extent to which manually assessed and USI-assessed ADIM differentiated between participants with LBP and those without.24
To date, the concurrent and discriminative validity of the manually assessed ADIM is unknown, and only one study addresses interobserver reliability.25 The present aims were therefore to assess the concurrent validity of the manually assessed ADIM in relation to the USI during guided abdominal contractions, to assess its discriminative ability and to determine the interobserver reliability.
Methods
Study design
A cross-sectional, single-blinded design was used to evaluate the concurrent validity, discriminating validity and interobserver reliability of the ADIM in patients with LBP, and in healthy subjects. A sample size of 50 participants was considered adequate to power the study, to obtain proper correlation data as used in concurrent analysis,26 while a sample of 27 participants was calculated for κ agreement data (CI 0.3; expected percentage agreement (PA) 0.8 and chance agreement 0.5) used in reliability statistics.27 Planned enrolment was undertaken to meet these criteria. The regional ethical review board approved the study (Dnr 2011/1859-31).
Study sample
Patients with LBP were recruited through information about the study distributed by email and telephone to six private physiotherapy settings in Stockholm, Sweden. Healthy subjects were found through written and verbal information distributed at two large companies in Stockholm, each with approximately 700 employees. Fifty-three participants, 38 with LBP and 15 healthy participants aged between 18 and 65 years, were included (table 1). Patients seeking care for a primary symptom of LBP were considered eligible, and were included if their LBP had lasted for at least 2 weeks and if they estimated their pain level to be >20 on a visual analogue scale (VAS 0–100).23 ,28 They were excluded if pain was severe and thought likely to prevent the planned test procedure; if they were pregnant; if they had undergone back or abdominal surgery within the last 6 months; or if they had a neurological disease, neurological signs of nerve root compression, inflammatory autoimmune disease, or a malignancy. Patients with spondylosis, or spondylolisthesis, were included if no signs of nerve root compression existed. Healthy subjects were excluded if they reported any pain on the VAS or had undergone back rehabilitation within the previous 5 years. Patients with LBP and healthy subjects both signed written informed consent forms. Participants were enrolled in the study between 2012–02–10 and 2012–06–27.
Demographic and self-assessment questionnaire data for all included participants (n=52)
Investigators
The manual investigators (n=3) were physiotherapists specialised in manual therapy for 13–32 years and with several years of experience assessing ADIM in patients with LBP. Another investigator skilled in musculoskeletal USI performed all the USI assessments. A same day intra-rater reliability was performed and calculated from the obtained USI measurements on 35 participants and considered very good (Intraclass correlation coefficient (ICC)2.1=0.84.).
The manual and the USI investigator were both blinded to the participant’s health status at the time of testing. At inclusion, prior to the clinical intervention, all participants completed demographic and medical history, and self-assessment questionnaires on pain and function.
Manual assessment of ADIM
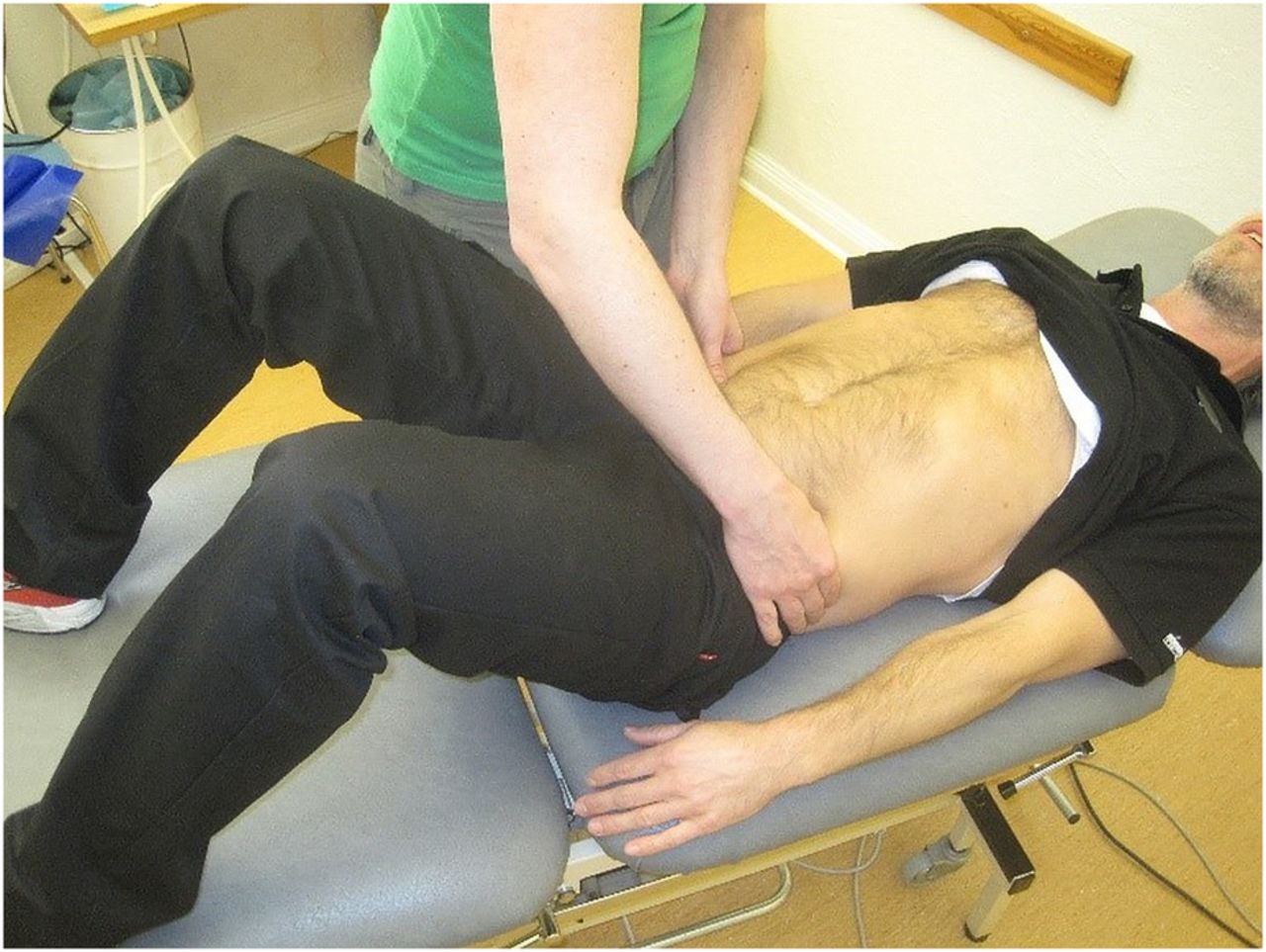
The ADIM was explained, performed and assessed, as a slow and gentle ‘abdominal hollowing’, as originally described by Richardson et al.13 The participants were in a supine hook, lying with hips at 40–60° and knees flexed between 90° and 100°, and arms placed along the torso (figure 1). They were instructed to gently draw the navel in towards the spine, to hold the contraction and breathe normally. The manual investigator palpated for muscle contraction medially to the spina iliaca anterior superior (SIAS). The success of a correctly performed contraction of the TrA was considered to be a slowly developed, deep tension in the abdominal wall continuously for up to 10 seconds (s).13 Compensatory patterns were observed during the test, such as: holding the breath; backward movement of the pelvis; visual or palpable contraction of the obliquus externus (OE) muscle; pressing the heels towards the floor. If any of these patterns appeared, the ADIM was assessed as incorrect.13 ,29–31 Before the investigation, the manual investigators underwent a training session to reach a consensus on how to judge whether the manually assessed ADIM was correct.

Test position for abdominal-drawing-in manoeuvre (ADIM).
Ultrasonography assessment of the ADIM and data processing
Ultrasound images were recorded with a Prosonix 600 DCPD Swissmed (HP Medical GMBH, Wollerau, Switzerland), and motions were registered using a linear-array transducer (5–10 MHz). Using B (brightness) mode ultrasound, the transducer was positioned across the abdominal wall at a point between the inferior angle of the rib cage and the iliac crest, approximately 100 mm from the umbilicus.32 ,33 On-screen callipers measured the distance between the inner edge of the fascial lines of the TrA, the obliquus internus (OI) and the OE muscles. The patient could not see the computer screen. Three pictures during rest and ADIM were recorded for each body side. The images of muscles at rest were collected at the end of exhalation, and images during the ADIM were collected when the patient had reached the expected peak of activity (figure 2).

{kind=link}
{kind=link}
Ultrasound image of abdominal muscles, Left= rest Right=activity during abdominal-draw-in manoeuvre (ADIM). Distance 1 represents musculus transversus abdominis (TrA), distance 2 musculus obliquus internus (OI) and distance 3 musculus obliquus externus (OE). Note the increase in TrA and OI and the decrease in OE during the ADIM, picture B.
Mean values of the measurements from the ADIM and resting position were calculated for TrA, OI and OE (table 2). From these values, three ratios were calculated: (1) the TrA contraction ratio (TrA-CR)=TrA thickness contracted/TrA thickness at rest, (2) the TrA preferential activation ratio=relative change in proportion of TrA relative to total lateral abdominal muscle thickness=(TrA contracted/ TrA+OE+OI contracted)–(TrA at rest/TrA+OE+OI at rest) and (3) OI+OE contraction ratio=OE+OI thickness contracted/OE+OI thickness at rest.14
Data from the USI measurements of muscle thickness (mm) at rest and during ADIM, presented with mean and SD (n=52)
The contraction ratio represents the relative change in muscle thickness as a result of muscle contraction; and the preferential activation ratio, the change in the proportion of the TrA relative to the total lateral abdominal muscle thickness.14
The mean ratio value −1 SD was selected as the cut-off to define the preferential activation of TrA.34 In assessing whether the ADIM, that is, the preferential activation of TrA, was correctly performed, all individual ratios had to exceed this defined cut-off to be accepted as passed (table 3).34 ,35
Calculated ratios from ultrasound imaging of lateral abdominal muscles during preferential activation of TrA
Experimental setup
All included participants were assigned by lot to start with either the manual or the USI assessment of the ADIM. They were briefed by the first investigator (either manual or USI) about the purpose of the ADIM and were instructed how to perform a correct ADIM. Following this, each participant was asked to perform an ADIM lasting up to 10 s without feedback; this was repeated three times. The manual investigator filled out a paper chart with yes or no; yes indicating a correctly performed ADIM.
If two of the three performed ADIMs were assessed as a correct contraction, the test was noted and filled out as correct. The subject rested for 10 min between the manual assessments and the USI assessment. To investigate the interobserver reliability of the manually assessed ADIM, a second investigator (M2) observed and assessed the ADIM 10 min following the first assessment (M1). Both investigators were blinded to each other's results.
Statistical analysis
For the concurrent validity analyses, Spearman's rank correlation coefficient (r) was used to calculate associations between the results of the manual test and the USI investigation of the preferential activation of the TrA. The coefficient (r) was defined as follows: 0.00–0.25=little or no correlation; 0.26–0.49=low correlation; 0.50–0.69=moderate correlation; 0.70–0.89=high correlation and 0.9–1.0=very high correlation.22 ,36
Discriminative validity was analysed by calculating sensitivity and specificity, with a 95% CI for patients with LBP and for healthy subjects. We considered at least 70% sensitivity and 50% specificity to be valid.36 A correctly or incorrectly performed ADIM was scored as ‘yes’ or ‘no’ for patients with LBP as well as for healthy subjects.
The interobserver reliability of the manual test was calculated using κ, and was presented with 95% CI, PA and SE. We defined the strength of the κ coefficient according to Landis and Koch: 0=poor, 0.01–0.2=slight, 0.21–0.40=fair, 0.41–0.60=moderate, 0.61–0.80 substantial and 0.81–1=almost perfect.37
Results
Fifty-three participants were allocated to the study. Their characteristics are presented in table 1. All the participants invited to participate agreed and were enrolled. One patient with LBP was excluded owing to un-interpretable images. Fifty-two participants (LBP n=37, healthy participants n=15) were thus included in the analyses. The patients with LBP had moderate pain (visual analogue scale; median 34, range 21–50) and low-to-moderate disability (Roland Morris Disability Score; median 7, range 3–14). There was no difference between patients with LBP and healthy subjects regarding age, height and body mass index. Sixty-eight per cent of the total sample were women.
Concurrent validity
Table 4 presents the associations between the manually assessed ADIM, and the USI-measured TrA contraction ratio (TrA-CR) and the TrA preferential ratio (TrA-Pref Ratio). None of the values for association were significant.
Associations between manually assessed ADIM and USI assessed, expressed in TrA-CR and TrA Pref Ratio in all participant (n=52) and in participants by investigator
The associations between the manually assessed ADIM and the USI-measured TrA-CR varied, and were overall low (r=−0.38–0.1), as were the results for the manually assessed ADIM and the TrA preferential activation ratio (TrA-Pref Ratio) (r=−0.19–0.53).
A subgroup analysis of the participants presenting with LBP (n=37) was also performed. Here, the agreement between the manually assessed ADIM, and the USI-measured TrA-CR and TrA-Pref ratio, also varied (r=0.09–0.17).
Discriminative validity
The discriminative validity of the manually assessed ADIM—that is, the ability of the test to discriminate between patients with LBP and healthy ones—showed a sensitivity of 0.30 and a specificity of 0.73. Regarding USI measurement of the ADIM, the discriminative validity for TrA-CR showed a sensitivity of 0.35 and a specificity of 0.80, while the TrA preferential ratio showed a sensitivity of 0.41 and a specificity of 0.8 (table 5).
Sensitivity and specificity for the USI-measured TrA contractions ratio (TrA-CR) and TrA preferential ratios (TrA-Pref Ratio) and manually assessed ADIM; presented with 95% CI
Reliability
The interobserver reliability of the ADIM manually assessed by two of the assessors (M1 and M2), revealed substantial agreement of 87.5%, (κ=0.71, CI (95%) 0.41 to 1.00) while the SE was 0.15.
Discussion
The present aim was to establish the concurrent and discriminative validity, and the interobserver reliability, of the manually assessed ADIM. The ADIM is a clinical tool for assessing preferential activity of the deep abdominal muscles in patients with LBP.
Our results showed poor concurrent validity, meaning weak associations between the manually assessed ADIM and the two calculated ratios of muscle thickness from the USI measurements. In addition to the low agreement, the results varied widely (TrA-CR r=−0.38–0.1; TrA-Pref Ratio r=−0.19–0.53). Further, no concurrent correlation between the manually assessed test and the USI measurements emerged when computed only for the group of patients with LBP. The validity of the manually assessed ADIM to discriminate those with LBP from healthy participants only reached low sensitivity regarding both contraction ratio and preferential ratio. The interobserver reliability of the manual assessment of ADIM in the present study was, however, substantial (κ=0.71).
Clearly, the manually assessed ADIM failed to agree with the USI measurements, both against TrA-CR and against the TrA preferential activation ratio. Reasons for the poor concurrent correlation may be the complexity involved in determining an isolated preferential contraction of a specific muscle when the activity seemingly appears in several muscles. Urquhart et al30 suggested that there is often a co-activation between TrA and OI, as both muscles have to stabilise the lumbar segments. This is also supported by that the fact that the OI has both a deeper and a superficial layer.30–32 Further, the anatomical position where the lateral abdominal muscles overlie one another contributes to the difficulty in palpating for an isolated TrA contraction.34 ,35 This raises the question of what this test actually adds, or what it actually measures, since the interobserver reliability was substantial.
Our results revealed good specificity to detect individuals presenting with a correct test among all participants. However, the results showed lower sensitivity, that is, the preferential activation, assessed both manually and with USI, did not meet the fundamental criterion of discriminating between patients with LBP and healthy subjects. Again, the question arises of whether there is a clinical use for the manually assessed ADIM to detect impaired preferential activation of TrA in patients with LBP. This must be taken into consideration if the test is to be used to identify functional impairments in patients under consideration for rehabilitation. Our results are supported by Pulkovski et al,34 who reported inconsistent outcomes in USI-measured preferential TrA activity in LBP and healthy subjects, concluding that the test was unable to differentiate between the two groups. The same results have been presented by other authors,34 ,37 ,38 who also concluded that the values of associations between healthy participants and patients with LBP measured with USI are highly variable and no association can be reached between groups during ADIM-USI. In contrast to these results, Teyhen et al38 showed significant differences in activity of the deep abdominal muscles assessed with USI in persons with LBP compared to healthy subjects, when performing an active straight leg raise test (ASLR). It should, however, be noted that their study design differed from ours, as no instruction of ADIM was given to the patients prior to performing the ASLR.
Even so, manual assessment of the ADIM is still commonly used in the clinic to differentiate between patients for guiding specific exercises to re-train motor control. On the present results, this can be questioned since the ability to perform seems simply to be a normal variation independent of LBP.
Ferreira et al39 reported improved TrA muscle activity measured with ultrasound following an intervention with specific motor control exercises to activate the deeper abdominals in people with a poorer ability to preferentially contract TrA. However, only low associations between improved functional level and the activity of the deep abdominals were reported. Moreover, recent studies report inconsistent relationships between alleviation of pain and disability, and changes in activity or muscle thickness in TrA as measured with USI B or M mode. Here, the participants were people with LBP following interventions with specific motor control exercises.15 ,39
The values obtained from the muscles measured with USI itself were consistent with previous findings.14 ,39 ,41 Small differences in mean values for anatomical distances appeared at rest and during measured muscle contraction.18 ,33 ,35 ,42 Our ratio values were similar to or slightly higher than those previously reported, a phenomenon that probably relates to basic data, especially the proportionally smaller value from the TrA at rest.14
Strengths and limitations
The strength of the present study is the aim to investigate both concurrent and discriminative validity, and also the reliability, of a clinical tool commonly used in the rehabilitation of patients with LBP, when prescribing specific exercises. A further strength is the study design, with investigators blinded to the health status of all the participants. Pulkovski et al34 studied the concurrent validity of the ADIM using ultrasound and a blinded design. They did not, however, investigate the manually assessed ADIM. To the best of our knowledge, no other study has performed a single blinded study of this manoeuvre.
While the use of USI as the criterion was believed to strengthen the results on validity, the gold-standard method itself showed low discriminative validity. Indeed, a possible limitation is that USI B mode was used instead of M mode in the assessment, suggesting the possibility that the peak of TrA activity during the ADIM was missed. Hodges et al18 proposed that a change in muscle dimension does not always correlate to increased muscle activity, depending on muscle length, muscle extensibility, pennate pattern and competing forces from adjacent muscles. The use of M mode with tissue Doppler imaging (TDI) may therefore be more advantageous than the use of B mode, as the images are sampled over time.34 This was, however, not feasible in the present study but should be tried in a future one.
Whittaker and collegues40 suggest that USI B mode may be used solely as a source of evaluation of muscle activity, and for understanding changes in muscle thickness and neuromuscular control. However USI B mode still plays an important role in detecting altered abdominal muscle function in subjects with LBP and affords helpful biofeedback for abdominal muscle function when evaluating treatment programmes.
For the selected cut-off value of the ultrasound measurements of TrA contraction and preferential ratio used in the calculations of concurrent validity, we used cut-offs previously defined for investigating the ability of the TrA-CR to discriminate between patients with chronic LBP and healthy participants.14 ,34 We are aware that a cut-off value will affect the outcome, and different cut-offs for these ratios may therefore be discussed and further investigated.
For strengthening internal validity, we presented the USI investigators’ intra-rater reliability (ICC 0.84), which is consistent with previously reported results of intra-rater reliability when measuring TrA muscle thickness with USI (ICC=0.92–0.99).16 The present interobserver reliability of the manual assessment of ADIM was substantial (κ=0.71), a finding that aligns with a previous study (κ=0.52).25
Our main aim was to investigate whether the manually assessed ADIM is a valid method for assessing a preferential activation of the deep abdominal muscles. We did this by comparing the manually assessed test (ADIM) results to the USI findings for the same action. Through blinding of the investigators by including both healthy subjects and patients with LBP, we aimed to minimise bias and thus strengthen the results. However, this led to a disproportionately large sample of patients with LBP, and this may be considered a limitation to the study.
It is imperative that clinical tests are studied for both validity and reliability. Therefore, the manually assessed ADIM should be further studied in order to afford clinicians better directions as to whether this clinical tool really is valid for detecting correct preferential activity of TrA in persons presenting with LBP.
Conclusion
Our study is the first to consider the concurrent and discriminative validity of the manually assessed ADIM, a commonly used clinical tool. Although it’s interobserver reliability was high, the concurrent validity and discriminative validity were both low for examining preferential activity of the deep abdominal muscles. Neither the manually assessed ADIM nor the ultrasound testing discriminated between patients with LBP and healthy subjects regarding preferential activity of the transversus muscle. This was because this ability was also noted in the healthy subjects. From the present results, it thus appears that the ‘preferential’ activity cannot be linked to patients with LBP, and this leads us to question the test's utility, in the clinic, for addressing impaired activation of the deep abdominals.
Acknowledgments
Financial support from the Swedish Confederation of Physiotherapists-Memorial Fund is gratefully acknowledged.
References
Footnotes
Contributors All the authors participated in the conception and design of the study, and all made substantial contributions to the acquisition of data. BOÄ and ERB performed the statistical analysis. All the authors participated in the interpretation of data. KK drafted the manuscript, and BOÄ and ERB critically revised it for important intellectual content. All the authors read and approved the final manuscript.
Funding No funding was recieved for the study.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The regional ethics review board in Stockholm, Sweden, approved the study (Dnr 2011/1859–31).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.