Article Text

Abstract
Introduction Neurodegeneration is a widely accepted contributor to the development of long-term disability in multiple sclerosis (MS). While current therapies in MS predominantly target inflammation and reduce relapse rate they have been less effective at preventing long-term disability. The identification and evaluation of effective neuroprotective therapies within a trial paradigm are key unmet needs. Emerging evidence supports amiloride, a licenced diuretic, as a neuroprotective agent in MS through acid sensing ion channel blockade. Optic neuritis (ON) is a common manifestation of MS with correlates of inflammation and neurodegeneration measurable within the visual pathways. Amiloride Clinical Trial In Optic Neuritis (ACTION) will utilise a multimodal approach to assess the neuroprotective efficacy of amiloride in acute ON.
Methods and analysis 46 patients will be recruited within 28 days from onset of ON visual symptoms and randomised on a 1:1 basis to placebo or amiloride 10 mg daily. Double-blinded treatment groups will be balanced for age, sex and visual loss severity by a random-deterministic minimisation algorithm. The primary objective is to demonstrate that amiloride is neuroprotective in ON as assessed by scanning laser polarimetry of the peripapillary retinal nerve fibre layer (RNFL) thickness at 6 months in the affected eye compared to the unaffected eye at baseline. RNFL in combination with further retinal measures will also be assessed by optical coherence tomography. Secondary outcome measures on brain MRI will include cortical volume, diffusion-weighted imaging, resting state functional MRI, MR spectroscopy and magnetisation transfer ratio. In addition, high and low contrast visual acuity, visual fields, colour vision and electrophysiology will be assessed alongside quality of life measures.
Ethics and dissemination Ethical approval was given by the south central Oxford B research ethics committee (REC reference: 13/SC/0022). The findings from ACTION will be disseminated through peer-reviewed publications and at scientific conferences.
Trial registration number EudraCT2012-004980-39, ClinicalTrials.gov Identifier: NCT01802489.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study examines optic neuritis as a discrete central nervous system inflammatory event with measurable structural and clinical outcomes allowing the time-efficient (6 month) assessment of neuroprotective therapies.
The repurposing of amiloride, a licenced diuretic with excellent safety record, as a neuroprotective therapy is supported by a strong basic and clinical science with potential to translate to multiple sclerosis (MS).
A multimodal approach including retinal scans and brain MRI will examine the effect of the intervention from the retina to the brain allowing the evaluation of sensitive outcome markers and inform structural–functional correlates for future studies of optic neuritis.
Neuronal loss can occur early in acute inflammation, therefore recruitment up to 28 days may be outside the effective ‘therapeutic window’ for neuroprotection.
The primary outcome measure uses the unaffected eye as a powerful comparator, but this eye may be affected by MS-related changes or previous subclinical optic neuritis, thus confounding the results.
Background
Overview
Multiple Sclerosis (MS) is the most common cause of progressive disability in young adults in the western world. It is characterised by inflammatory demyelinating plaques with associated axonal and neuronal damage affecting the central nervous system (CNS). The accumulated impact of neurodegeneration is thought to be the major pathological substrate for disability in MS.1 One of the major unmet needs in MS is for safe, cost-effective therapeutic interventions that prevent neurodegeneration and thereby the development of disability. The natural history of MS is such that disability accrues slowly in the majority of patients and therefore studies examining neuroprotective therapies can be protracted and expensive. Clinical trial paradigms examining acute inflammatory optic neuritis (ON) may help overcome this barrier by demonstrating a ‘proof-of-concept’ neuroprotective benefit for repurposed or novel therapies.
Acute inflammatory ON is a common cause of reversible visual loss in young adults in the UK and western world. Patients typically present with painful visual loss that progresses for a maximum of 2 weeks and then recovers over the following 2–6 weeks, with further prolonged recovery of up to a year.2 ON is a common precursor to the development of MS with approximately 50% of patients developing MS within 10 years.3 In addition, 70% of patients with MS will show evidence of optic nerve involvement over time.4 The presence of inflammatory demyelination and associated axonal loss in ON parallels the pathophysiology observed in other white matter structures in MS5 enabling translational research in ON to be applicable to the wider patient group affected by MS.
The distinct anatomy and function of the optic nerve affords unique ways of studying both structural and functional changes in the CNS during the acute and recovery phases of ON. The retinal nerve fibre layer (RNFL) is a major site of axonal loss after ON.6 Recent advances in retinal imaging allow accurate in vivo estimates of RNFL thickness, with the use of scanning laser polarimetry (GDx) and optical coherence tomography (OCT). High-resolution spectral domain OCT (SD OCT) with segmentation allows precise measurement of specific retinal layers using computerised algorithms and quantitation of both peripapillary and macular RNFL as well as the ganglion cell (GCL) and other retinal layers. Both GDx and SD OCT have recently been employed in neuroprotective trial frameworks7 allowing neurodegeneration to be quantified in vivo both sensitively and longitudinally.8–10 Moreover, OCT measures of RNFL loss correlate with clinical outcome measures of visual acuity and disability as measured by the Expanded Disability Status Scale (EDSS). Surrogate markers of neurodegeneration such as MRI measures of cerebral brain atrophy also correlate with RNFL loss.11 Thus, ON affords the opportunity to assess the impact of neuroprotective strategies in inflammatory CNS disease.
Currently there are no therapeutic strategies that have been shown to improve the visual outcome in ON. Oral or intravenous methylprednisolone has been shown to hasten the visual recovery of ON but not to affect the final visual outcome.2 Thus, by assessing amiloride, this trial aims to meet the major unmet need for cost-effective, safe, neuroprotective strategies that reduce both axonal loss and disability in ON and by extension to MS.
Translating the basic science
Recent advances in molecular biology have shed new light on the mechanisms of axonal loss and on potential therapeutic targets in ON and MS.
While axonal loss in MS is likely to be multifactorial, a key end point is the influx of sodium (Na+) and calcium (Ca2+) ions through ion channels and exchangers.12 Recent evidence has implicated the Acid Sensing Ion Channel type 1 (ASIC1), capable of fluxing both Na+ and Ca2+, as a mediator of neuronal injury in stroke and more recently in CNS inflammation.13 ,14
Amiloride, a licenced diuretic with a proven safety record, acting through ASIC1 blockade was found to be significantly neuroprotective and myeloprotective in animal models of MS.13 Furthermore, a recent single arm, open label, longitudinal run-in trial of amiloride in primary progressive patients with MS showed a significant reduction in the rate of brain atrophy on the amiloride treatment phase, compared to the run in phase. In tandem with this, diffusion tensor imaging indices of tissue damage were significantly reduced during the treatment phase in clinically relevant white matter structures suggesting a neuroprotective benefit in patients with MS.15
This converging basic and clinical science strongly supports a role for further testing of amiloride as a novel neuroprotective drug in the treatment of ON and MS.
Methods
Objectives and outcome measures
The Amiloride Clinical Trial in ON (ACTION) incorporates multimodal techniques covering imaging modalities of GDx, OCT and MRI combining with clinical and functional outcomes.
Primary objective
To evaluate the potential neuroprotective efficacy of amiloride in ON through the surrogate measure of retinal nerve fibre layer (RNFL) measurement.
Outcome measure
GDx determined difference in peripapillary RNFL thickness between affected eye at 6 months and unaffected fellow eye at baseline.
In addition secondary outcome measures of the primary objective will be made by assessing GDx derived difference in the affected eye at 12 months compared to the baseline unaffected eye, and the same measurements of RNFL will be made using OCT. Further OCT secondary outcome measures will utilise retinal layer segmentation to determine macular RNFL thickness and volume as well as GCL measurements.
Secondary objectives
Secondary objective 1
To assess markers of neurodegeneration in ON and the neuroprotective effect of amiloride through MRI outcomes.
Outcome measures
MRI surrogate markers of white and grey matter injury and connectivity derived on 3 T MRI at baseline, 6 and 12 months, including:
Diffusion-weighted imaging (DWI) measures of fractional anisotropy (FA), mean diffusivity (MD), axial and radial diffusivity (RD) of the postchiasmal visual pathways;
High-resolution T1-weighted imaging of the cortical and subcortical grey matter volume;
MR spectroscopy (MRS) measures of N-acetylaspartate (NAA) in the visual cortex;
Resting state functional MRI (RS-fMRI) patterns of activity;
Magnetisation transfer imaging (MTI) derived magnetisation ratio (MTR) of the white and grey matter.
Secondary objective 2
To assess whether amiloride improves functional and visual outcome following ON.
Outcome measures
High and low contrast visual acuity at baseline, 6 and 12 months
Humphrey visual fields (HVF) at baseline, 6 and 12 months.
Fansworth Munsell 100-hue colour vision test (FM100) at baseline and 6 months
Latency and amplitude of waveforms in pattern visually evoked potential (PVEP) and pattern electroretinogram (PERG) at baseline and 6 months
Quality of life scores on the national eye institutes 25-point visual functioning questionnaire (NEI-VFQ-25) and the 10-point neuro-ophthalmic supplement (10-NOS).
Secondary objective 3
To confirm ON as a sensitive and efficient model for neuroprotection in a clinical trials framework.
Outcome measures
A combination of outcome measures of MRI, RNFL, electrophysiology and clinical outcome measures will individually determine the validity of these measures and correlations will also support this trial platform for further neuroprotective studies.
Study design
The ACTION trial is a phase II randomised, double blind, investigator led, parallel group placebo controlled trial to examine the neuroprotective efficacy of amiloride treatment following ON (figure 1). We will recruit 46 participants who have either a clinically isolated syndrome of ON, or ON in participants with MS previously unaffected by ON. Participants will be randomised on a 1:1 basis to amiloride or placebo for 5 months treatment. The primary outcome measure will be peripapillary RNFL thickness on GDx at 6 months compared to unaffected fellow eye at baseline. Secondary outcome measures will be visual outcomes (visual acuity, LCVA, visual field and colour vision), MRI and GDx/OCT measures at baseline, 6 and 12 months, PVEP and PERG at baseline and 6 months. The 12 month measurements will assess if the potential benefit from amiloride is sustained and whether or not a rebound neurodegeneration occurs when off active drug. Placebo treatment identical to amiloride and blinding of both the investigators and participants to treatment is being utilised to minimise bias. We propose to combine longitudinal measurements of RNFL thickness determined by both GDx and OCT to provide evidence of the neuroprotective efficacy of amiloride. This will be supplemented by clinical and electrophysiological outcomes and non-conventional MRI measures. In the treatment arm of the study we will use 10 mg of amiloride. This replicates the efficacious and well-tolerated dose used in our preliminary study in primary progressing multiple sclerosis participants, and is consistent with the licenced dose of amiloride.

Amiloride Clinical Trial In Optic Neuritis (ACTION) trial visit schedule. Aq-4, aqusporin-4; FBC, full-blood count; HVF, Humphrey visual field; LCVA, low contrast visual acuity; LFT, liver function test; GDx, scanning laser polarimetry; OCT, optical coherence tomography; PERG, pattern electroretinogram; PVEP, pattern visually evoked potential; QOL, quality of life; VA, visual acuity; VEP, visual evoked potential.
We aim to randomise and initiate treatment within a maximum of 28 days from onset of visual symptoms but it is expected that a median of 14 days will be achieved. This timeframe has been chosen because longitudinal studies have shown that RNFL loss is greatest within 3 months after onset of ON.10 Therefore, initiation of therapy as early as possible is likely to positively influence the primary outcome measure; showing that amiloride has a neuroprotective effect. Treatment will be for a 5-month period from randomisation; this will allow a therapeutic efficacy during the early period of the majority of RNFL loss. This allows for a 4 week ‘washout’ period prior to imaging, to ameliorate any potential influence on tissue volume from the diuretic effect of amiloride. Similarly, imaging outcomes incorporating volumetric analyses (MRI, OCT, GDx) will be acquired prior to randomisation to minimise any potential confounding effect of the drug. In addition, MRI prior to randomisation will mitigate potential inclusion of compressive optic neuropathies.
In current clinical practice some patients may be given a course of oral or intravenous methylprednisolone at the initial presentation of ON. Methylprednisolone has been shown to hasten the recovery of ON, but not change the visual outcome.2 Given the systemic side effects of high-dose steroids, this is usually restricted to a small group of patients in whom symptoms are severely restricting their activities of daily living. It has been shown that our primary outcome of RNFL thickness is not affected by administration of methylprednisolone in ON.16 The use of methylprednisolone is decided by the treating physician outside the study, and would be recorded in the case report form (CRF). However, because we do not expect it to affect our primary end point it will not affect study inclusion.
Outcome measures of neuroprotection in ON being used in the ACTION trial
Imaging outcome measures
GDX
The primary measure of efficacy will be whether participants treated in the acute stage of ON with amiloride show greater preservation of RNFL thickness at 6 months compared to a placebo control group. The RNFL is the only retinal structure that is birefringent to a polarised light, therefore a change in the retardance of a polarised light can be measured by GDx and used to reliably infer the thickness of RNFL. The difference in RNFL thickness, as measured by GDx (GDx, Carl Zeiss Meditech) between affected eye at 6 months and unaffected fellow eye at baseline will be compared between the amiloride and placebo groups. Quality control of the image capture of GDx will be consistent with previous studies.17 Given the heterogeneity in baseline RNFL measurements in control groups, comparison with fellow unaffected eyes has been shown to be more sensitive than comparing with measurements from control groups for detecting RNFL thinning in ON, though both methods show a significant RNFL thinning following ON.18
Optical coherence tomography
An additional measure of RNFL will be made using OCT (Spectralis OCT, Heidelberg Engineering). This uses near infra-red light to form a cross-sectional image of the retina. In addition to the RNFL around the optic nerve, OCT allows segmentation of the retinal layers at the macula, providing measurements of macular RNFL, GCL, inner nuclear layer and outer retinal layers. Quality control of the image capture will be in line with published consensus guidelines.19 There is increasing evidence that the GCL at the macula, as identified on this spectral domain OCT, is affected after ON8 and has been shown to be more closely correlated with visual function in MS cohorts20 than RNFL thickness, which is measured around the optic nerve. This retinal segmentation provides additional information on neurodegeneration in ON and comparison between the two arms of the study will provide further insight into the potential protective effect of amiloride.
MRI
Conventional MRI
To enhance the interpretation of the non-conventional MRI measures, T1 and T2-weighted MRI sequences will be acquired and used to assess brain volume and white matter lesions typically found in MS and ON. The presence of these lesions, which can be prognostic for MS, may be passed on to the patient if they wish to know this information.
Diffusion imaging
Diffusion-weighted imaging (DWI) has been used extensively to study grey and white matter regions of interest, and recently the white matter of the optic tracts in established MS cohorts.21 Previous studies using MRI have demonstrated changes and reduction in white matter connectivity one year after ON.22 DWI provides quantitative measures of tissue integrity; radial diffusivity (RD), fractional anisotropy (FA) and mean diffusivity (MD). The numerical values produced from these measurements allow statistical analysis and infer white matter connectivity and integrity.
Magnetic resonance spectroscopy
MR spectroscopy (MRS) measures of NAA will be undertaken. It has been consistently reported that levels of NAA on MRS are lower in patients with MS compared to healthy controls, and the level of NAA has also been linked to disability, particularly in the early stages of disease.23 In addition, in a cross-sectional study of patients presenting with ON and other clinically isolated syndromes, levels of NAA were low.24
Resting state functional MRI
Resting state MRI is a form of functional MRI (fMRI). FMRI measures the blood oxygen level-dependant (BOLD) MRI signal, which can identify areas of brain activation. It has increasingly been shown that at rest, fluctuations in the BOLD signal correspond to anatomical and functional networks in the brain, with one of the most readily identifiable being in the visual cortex.25 Recently a cross-sectional study has shown changes in the pattern of activity in RS-fMRI between normal controls, patients with MS with previous ON and those without previous ON.26
Magnetisation transfer imaging
MTI measures the magnetisation derived from hydrogen ions that are bound to large molecules.27 Myelin has an abundance of such hydrogen ions and there is pathological evidence that MTI is closely correlated with myelin content.28 Loss and repair of myelin are key areas of interest in the pathophysiology of MS, and experimental evidence suggests that amiloride is myeloprotective as well as neuroprotective.13
Clinical outcome measures
We will assess visual acuity using early treatment of diabetic retinopathy (ETDRS) letter contrast charts. These allow patient's vision to be scored numerically, which can enable statistical analysis. In addition, low contrast visual acuity (LCVA) using Sloan 1.25% contrast and 2.5% contrast charts has consistently been linked to RNFL thickness in previous studies of patients with ON and MS.11 Visual fields will be tested using the standardised SITA-STANDARD 30–2 protocol on the Humphrey visual field machine (HVF). This automated sequence matches the patient's results to a large control population and will derive deviation scores that can then be statistically analysed. In addition we will be assessing colour vision with the Farnsworth Munsell 100-Hue colour vision test (FM100). The total error score on the FM100 is strongly correlated with RNFL thickness.29
Electrophysiological outcome measures
Prolongation of the latency of the P100 deflection of the pattern visually evoked potential (PVEP) are characteristic in acute ON. This then improves but remains delayed in absolute terms after visual recovery,30 thus providing a useful diagnostic tool that is used in clinical practice, and as an outcome measure in therapeutic trials. Furthermore the pattern electroretinogram (PERG) aids the interpretation of the PVEP by providing an assessment of macular function. The amplitude of the PERG is partially derived from the GCL component of the RNFL,31 and reductions in it are readily identifiable in ON.32
Quality of Life
We aim to measure vision-related quality of life scores using the standardised national eye institute visual functioning questionnaire (NEI-VFQ-25) with a 10-item neuro-ophthalmic supplement (10-NOS). The NEI-VFQ-25 provides a standardised quality of life score for ophthalmic disease validated across ophthalmic epidemiological studies.33 Both NEI-VFQ-25 and 10-NOS have been significantly correlated with segmented retinal layers on spectral domain OCT in ON.34
Eligibility/participants
Diagnosing ON
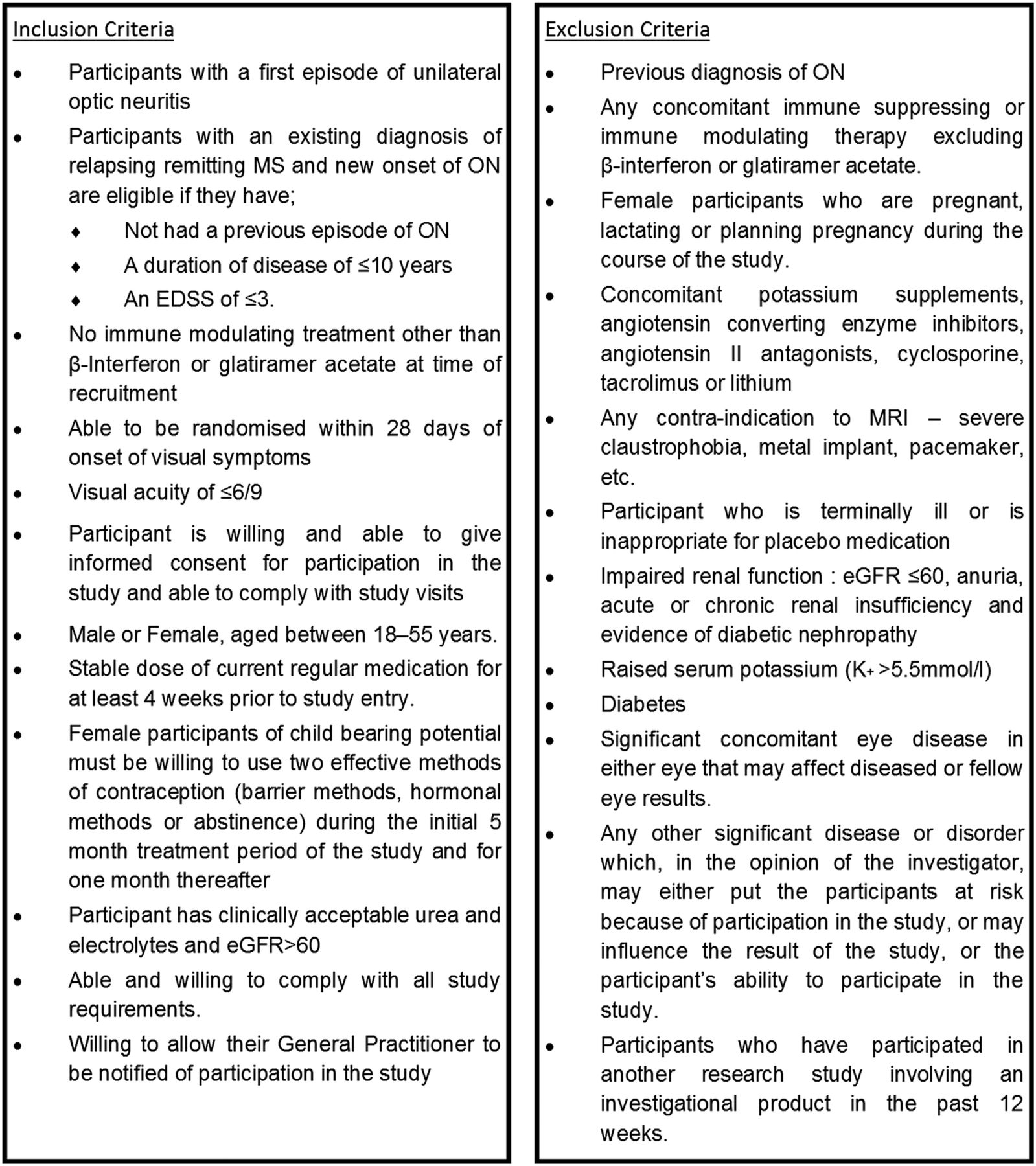
ON is a clinical diagnosis based on a combination of some or all of several key clinical features. These include pain on eye movement, subacute reduction in visual acuity over hours or days, presence of a central or paracentral visual field defect, presence of a relative afferent pupillary defect and either a swollen or normal appearing optic disc with an absence of pallor in the acute phase.35 Detailed inclusion and exclusion criteria are listed in figure 2.
{kind=link}
{kind=link}
Amiloride Clinical Trial In Optic Neuritis (ACTION) trial inclusion and exclusion criteria. EDSS, Expanded Disability Status Scale; eGFR, estimated-glomerular filtration rate; ON, optic neuritis.
Atypical ON
A proportion of patients diagnosed with ON will have a non-MS associated alternative diagnosis (atypical ON 36). This ranges in reports from 1.6% to 16%37–39 and the conditions involved are also inflammatory (eg, sarcoid ON, chronic relapsing idiopathic optic neuropathy, neuromyelitis optica). Given the ASIC pathway is a downstream mechanism of neurodegeneration in general CNS inflammation, we would not anticipate that amiloride would be detrimental to these groups.
The clinical course of an atypical ON is such that the diagnosis may not be discriminated from typical ON until after a poor recovery of vision in the initial weeks after ON. In addition, in the case of neuromyelitis optica, the diagnosis can be confirmed following positive antiaquaporin-4 antibody testing. However, this result will not be available until visit 3 (at 4 weeks). Once identified, these participants will be removed from the intention-to-treat (ITT) cohort and referred for appropriate care. Other differential diagnoses will remain in the ITT cohort and also be referred for appropriate clinical care. However, should these participants require immunosuppressive treatment they will be removed from the final analysis. We accounted for a 10% rate of atypical ON in our study powering, in addition to removing participants with neuromyelitis optica from the ITT cohort. We would aim to have a much smaller number of residual atypical ON than this, however, given the need for early recruitment necessary for neuroprotection, we recognise the potential for atypical ON to enter the cohort.
Ischaemic optic neuropathies
The age group eligibility criteria for this trial were selected to minimise the potential inclusion of patients with ischaemic optic neuropathies (anterior ischaemic optic neuropathy). While these can be confused with ON at initial diagnosis, they generally differ in their clinical presentation and natural history. Participants subsequently diagnosed with ischaemic optic neuropathy will be removed from the ITT analysis. Moreover, we do not anticipate any harm from amiloride in these groups as animal models of CNS ischaemia, have implicated ASIC1 as an important factor in neuronal injury with blockade providing neuroprotective benefit.40
Study procedures
Study procedures will all take place at the John Radcliffe hospital and the FMRIB centre at the John Radcliffe site.
Screening and eligibility assessment
Participants will be identified at the time of their presentation with ON, by the clinical care team at the trial site (Oxford) or patient identification centres (PIC) and given the participant information leaflet (PIL) at that point. With the patient's permission, which will be documented in the notes by the treating ophthalmologist or neurologist, they will be telephoned by the trial team and invited to come to the trial centre in Oxford.
Prescreening will take place in the form of discussion between the trial centre and the recruiting physician in order to ensure that the patient meets all the medical inclusion and exclusion criteria. Participants will have had an eye examination as part of their routine clinical care, this will only be repeated by the trial team at screening if the trial team deem it necessary to confirm the diagnosis of ON.
Informed consent
Written and verbal versions of the participant information and informed consent will be presented to the participants.
Written informed consent will then be obtained by means of participant dated signature and dated signature of the named trial investigator who discussed the trial and obtained the informed consent.
Randomisation
Subject numbers will be assigned sequentially as each subject enters the study. The subjects will be assigned a study drug through a centralised randomisation software hosted by the UKCRC registered Oxford Cognitive Health and Neuroscience Clinical Trials Unit. The randomisation will be performed by study investigators whose access to the software does not allow unblinding. If requested on clinical grounds the decision to unblind will be made by the chief investigator. The randomisation log and unblinding envelopes are held in the John Radcliffe Pharmacy with a 24 h on call service. A random-deterministic minimisation algorithm will be used to produce treatment groups balanced for important prognostic factors. The first 10% of participants will be allocated randomly without minimisation to avoid predictability. Subsequently the minimisation algorithm will be applied with an allocation ratio that is not fully deterministic: there will be an 80% bias in favour of allocations that minimise the imbalance.
The randomisation algorithm will minimise for the following three variables related to prognosis at baseline:
Sex (male or female)
Number of weeks since onset of symptoms (<2 weeks; ≥2 weeks)
Severity of visual acuity (between ≤6/9 and ≥6/18, ie, mildly affected; <6/18 and worse, ie, severely affected).
The study drug will be labelled with the study number and unique pack identification number. The two treatments amiloride and placebo will be indistinguishable.
Statistics
Sample size
It is estimated that the maximum total number of participants randomised will be 50 (25 per arm). Thirty six participants are required to detect a difference of 7.4 μm between groups on the primary outcome (difference in RNFL between affected and unaffected eye). This assumes a SD of 6.6, power of 90% and a 5% significance level. Allowing for a 10% drop out rate this increases to 40. However, as described previously, it is thought that approximately 10% of participants may have atypical ON. Therefore, to ensure that there is enough power to detect this difference in the typical ON subgroup we will need to randomise a total of 46 participants.
It is likely that patients found to have neuromyelitis optica (NMO) as described above will be given further medications that are potential confounding factors (listed in exclusion criteria) and they will not be included in the main ITT analysis. Therefore, randomisation will continue until a total of 46 participants have been randomised and reached the 4-week point without being diagnosed with NMO. It is thought that a maximum of 8% of participants randomised could have NMO, increasing the possible sample size to 50.
Quality control and quality assurance
There will be an independent data and safety monitoring committee (DMC) made up of an independent consultant neurologist, an independent consultant ophthalmologist, an independent statistician and the trial statistician. They will meet and perform interim analysis according to the DMC charter.
The trial investigators and the DMC will have access to the final trial data set.
Regular monitoring will be performed according to ICH GCP by Oxford Cognitive Health and Neuroscience Clinical Trials Unit. Data will be evaluated for compliance with the protocol and accuracy in relation to source documents.
Overall supervision of the trial will be co-ordinated through a trial steering committee consisting of an external consultant neurologist with experience in clinical trials in neuroprotection in ON and MS, the PI, the statistician, the coapplicants, a lay member and research nurses. The trial steering committee will meet every 6 months supplemented with teleconferencing as required by its members.
Confidentiality
Data will be stored within a firewall and password-protected computer system within a swipe-card secured building. Investigators will ensure that the participants’ anonymity is maintained. The participants will be identified only by initials and a participants ID number on the CRF and any electronic database. All documents will be stored securely and only accessible by trial staff and authorised personnel. The study will comply with the Data Protection Act which requires data to be anonymised as soon as it is practical to do so.
Analysis
Inclusion in analysis
The primary analysis will be carried out on a modified intention to treat cohort. This cohort will include all randomised participants (analysed in the group to which they were randomised) with the exception of those diagnosed with NMO in the first 4 weeks from randomisation.
A further sensitivity analysis will be carried out including all randomised participants with typical ON only. They will be analysed in the group to which they were randomised.
Analysis of primary outcome
The primary outcome will be presented using means and SDs and the difference between the two groups will be presented as the difference in means with 95% CI. The primary outcome will be analysed using an analysis of covariance to assess the treatment effect at 6 months, adjusting for baseline value and minimisation factors. We will formally assess the distribution of the data for evidence of departure from normality and, if necessary, transform the data or analyse using a non-parametric equivalent. A 5% level of significance will be used.
Analysis of secondary outcomes
Continuous secondary outcomes (OCT, letter score, electrophysiological data, colour vision data, visual field data and quality of life data) will be analysed in the same way as the primary outcome.
MRI analysis will be performed using FSL tools (http://www.fmrib.ox.ac.uk/fsl)41 and will include both a region of interest approach and measures of whole brain metrics to assess for differences between amiloride and placebo groups.
Discussion
Neuroprotective strategies and efficient means to test them within a clinical trial setting remain key unmet needs in ON and MS. ACTION is a phase II clinical trial aiming to provide proof of concept that amiloride is neuroprotective in acute inflammatory ON. The trial encompasses a multimodal approach combining structural and functional outcomes with clinical measures enabling the refinement of future trial designs.
However, the recruitment of acute patients with ON within a short time window to a clinical trial setting can be challenging and requires a high degree of cooperation between clinical and research staff in order to give potential participants the opportunity to take part. Despite this, within the spectrum of CNS structures affected by MS, one of the major values of using ON to assess neuroprotection is that the visual system provides unique opportunities to do so in a timely and efficient manner.
Ethics and dissemination
The findings from ACTION will be disseminated through peer-reviewed publications and at scientific conferences. Each participant will receive a summary of the overall results.
Acknowledgments
The authors would like to thank Abigail Koelewyn for her help in formatting of the manuscript and figures, and Dr Charles Cottrial for his help with the electrophysiological outcomes in the trial.
References
Footnotes
Contributors JBM and MJC designed the trial protocol, with scientific insight and contributions from CK, JE, JP, NE, LF and YK. JBM prepared the first draft of this manuscript and it was reviewed by MC, CK, JE, JP, NE, LF, SG and YK. Revisions were performed by JBM and MJC.
Funding This work is supported by the Multiple Sclerosis Society in the UK, grant reference 952/11.
Competing interests MJC received an unrestricted grant from Biogen for technical equipment used within the study. The remaining author's declare no competing interests.
Ethics approval South Central Oxford Rec B. ref: 13/SC/022.
Provenance and peer review Not commissioned; externally peer reviewed.