Article Text

Abstract
Introduction Ensuring that patients receive care that is consistent with their goals and values is a critical component of high-quality care. This article describes the protocol for a cluster randomised controlled trial of a multicomponent, structured communication intervention.
Methods and analysis Patients with advanced, incurable cancer and life expectancy of <12 months will participate together with their surrogate. Clinicians are enrolled and randomised either to usual care or the intervention. The Serious Illness Care Program is a multicomponent, structured communication intervention designed to identify patients, train clinicians to use a structured guide for advanced care planning discussion with patients, ‘trigger’ clinicians to have conversations, prepare patients and families for the conversation, and document outcomes of the discussion in a structured format in the electronic medical record. Clinician satisfaction with the intervention, confidence and attitudes will be assessed before and after the intervention. Self-report data will be collected from patients and surrogates approximately every 2 months up to 2 years or until the patient's death; patient medical records will be examined at the close of the study. Analyses will examine the impact of the intervention on the patient receipt of goal-concordant care, and peacefulness at the end of life. Secondary outcomes include patient anxiety, depression, quality of life, therapeutic alliance, quality of communication, and quality of dying and death. Key process measures include frequency, timing and quality of documented conversations.
Ethics and dissemination This study was approved by the Dana-Farber Cancer Institute Institutional Review Board. Results will be reported in peer-reviewed publications and conference presentations.
Trial registration number Protocol identifier NCT01786811; Pre-results.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Ensuring that patients receive care that is consistent with their goals and values is a critical component of high-quality care.1 Early conversations about advance care planning (ACP) with seriously ill patients have been associated with better outcomes for patients and families.2–4 However, multiple deficits in the timing and content of these discussions have been described. Discussions occur too late, when patients are in crisis or unable to make decisions for themselves, or clinicians who know the patient are not available.5–7 Even though most patients want to know about their prognosis, such information is often not shared,8 ,9 leading to poorly informed decisions. Furthermore, contrary to expert recommendations,1 physicians tend to focus these critical conversations on choices about procedures (eg, resuscitation or feeding tube insertion) rather than on the goals, values and wishes that form the basis of an informed patient's decisions. Clinicians are underprepared and undertrained to conduct high-quality end-of-life conversations,10 and tend to avoid them.11 Several studies of physicians in the UK,12 the USA,13 and in an international palliative care training programme14 ,15 demonstrate that communication skills instruction programmes are effective,16 with participants showing sustained improvement in patient-centered communication skills, including significant improvement in responses to patients’ emotional cues.12 Interactive, case-based learning sessions with communication skills practice are the most effective;17 however, most often, these training programmes have been intensive, multiday off-site retreats which are not always feasible for busy clinicians in practice.
One proposed solution to deficits in ACP and end-of-life discussions is for palliative care clinicians, who are trained to conduct such conversations, to see all seriously ill patients. Early palliative care intervention, the primary focus of which is communication,18 with ambulatory patients with non-small cell lung cancer has been demonstrated to improve quality of life, mood and survival, and to reduce aggressiveness of care and hospital length of stay.4 While palliative care physicians are an excellent resource for conducting/assisting with end-of-life conversations, there is already a shortage of approximately 11 000 palliative medicine physicians for hospices and hospital-based palliative care programmes;19 this workforce shortage is only expected to increase with future demographic changes. It is unlikely that this care model will be scalable.20 Thus, other approaches are needed, to engage non-palliative care physicians in integrating basic elements of palliative care, such as ACP, in the care of patients with serious illnesses.
We have developed, piloted and refined a multicomponent Serious Illness Care Program (SICP) to improve conversations about values and goals for patients with serious illnesses. The goals of this programme are to train and support oncology clinicians in integrating best practices in ACP in the care of their patients, to optimise the alignment between patient goals and the medical care they receive, and to enhance quality of life and peacefulness throughout the late stages of illness. We describe the steps taken in developing the programme, including review of the evidence about the effectiveness of ACP discussions,21 ,22 pilot work with oncologists to improve their ACP practices, engagement of a national advisory board, and development and pilot-testing of a structured approach to these conversations in the form of a seven-item Serious Illness Conversation Guide (SICG) for clinicians and patients. Then, we describe the research protocol: setting, recruitment, measurements, design of the intervention, timing of assessments, data analysis and collection, and planned analyses and dissemination.
Literature review
We conducted and published an extensive literature review of the evidence about early goals-of-care discussions.21 These discussions were found to be associated with better quality of life, reduced utilisation of non-beneficial medical care near death, enhanced goal-consistent care, positive family outcomes and reduced costs. Existing evidence does not support the commonly held belief that communication about end-of-life issues increases patient distress. The review also described best practices in conversations about serious illness care goals, and offered guidance to clinicians and healthcare systems on following a systematic approach to quality and timing of such communication to assure that each patient has a personalised serious illness care plan.
Pilot work
To begin understanding how the physicians in our institution actually conduct ACP discussions, we asked oncologists in the Gastrointestinal Oncology and Neuro-oncology centres at the Dana-Farber Cancer Institute (DFCI) to conduct values and goals discussions with their patients with pancreatic cancer or glioblastoma multiforme as part of an institutional quality improvement initiative. We evaluated clinical documentation before and after education where we introduced clinicians to an ACP module in the electronic medical record (EMR) intended to simplify tracking of patient values and goals. The proportion of patients whose physician documented their values and goals was low (<5%) before the intervention, and the norm (>90%) after the intervention. Following this pilot initiative, we solicited feedback from the clinicians with a structured interview about their experiences in conducting and documenting these discussions. This feedback later informed the development of our conversation guide and training programme.
Consultation with National Advisory Group
Early in the project, we gathered a national panel of experts for an Advisory Group for the SICP. Members included palliative care specialists, general internists, cardiologists, oncologists, paediatricians, surgeons and patients. Some members had extensive expertise in end-of-life communication skills and ACP; others were representative clinicians and patients who would be using the intervention. The purpose of the meeting was to discuss key elements of agreement and disagreement about best practices in serious illness communication, to elicit feedback about a proposed intervention, and to obtain input on our research design. Prior to the meeting, all members received an extensive background document, including a literature review.
Development of the SICP materials
Building on our literature review and pilot work, we developed a systematic approach to integrate best practices in outpatient care for patients with serious illnesses, and proposed a structured format to guide the discussions—the novel seven-item SICG (figure 1). This guide addresses eliciting illness understanding, eliciting decision-making preferences, sharing prognostic information according to preferences, understanding goals and fears, exploring views on trade-offs and impaired function, and wishes for family involvement. In addition to the SICG, designed for clinicians to use in outpatient encounters with their patients, we developed a letter to give patients before the visit to help them prepare for the discussion, and a family communication guide to send home with patients after the discussion to aid in discussing their values and goals with their family. The family guide follows the same general structure as the SICG, but in the patient's voice.
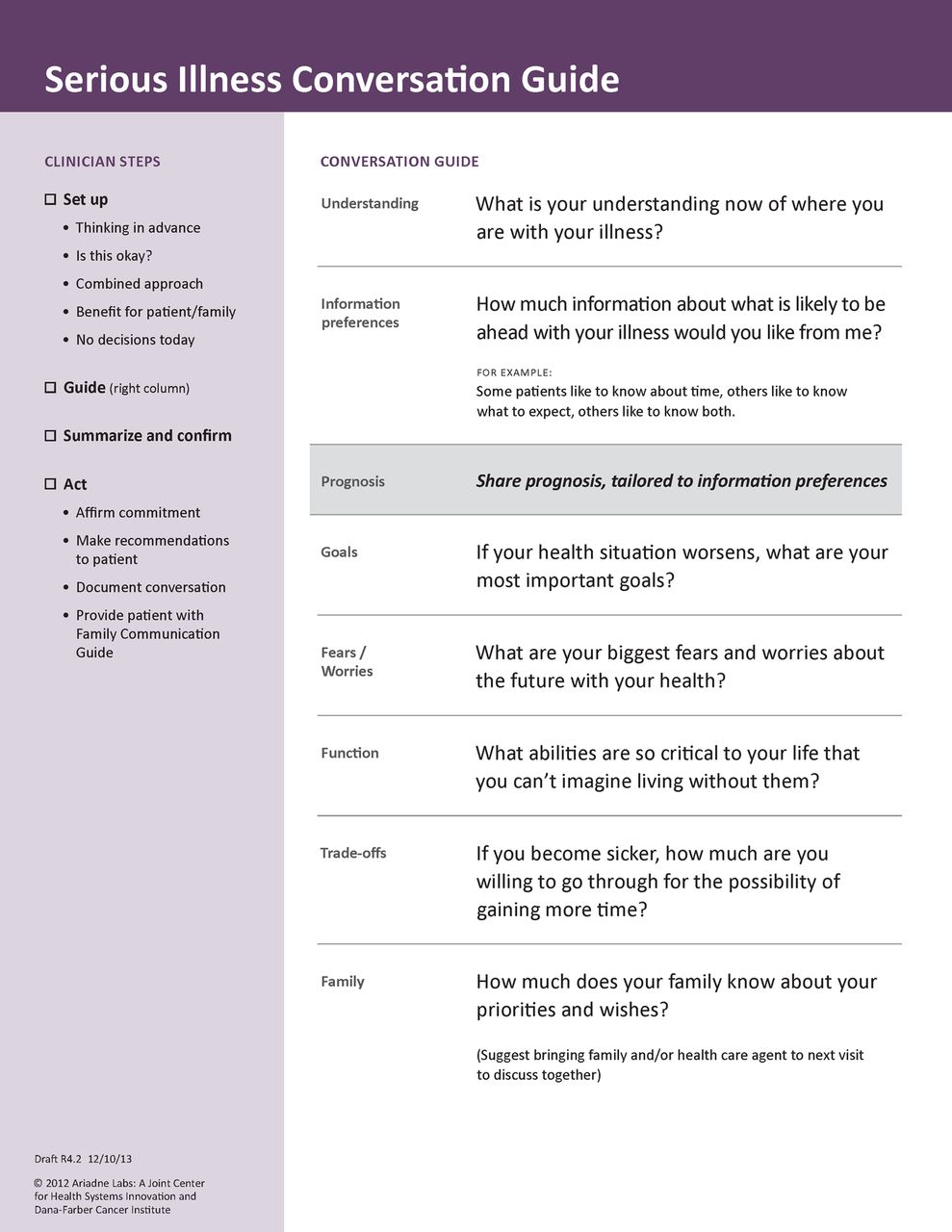
Serious Illness Conversation Guide.
Patient input
We sought feedback from the DFCI Patient and Family Advisory Council about our materials (SICG, family guide, pre-visit letter, etc) through a series of meetings. The Patient and Family Advisory Council consists of patients, family members, executive leaders and providers partnering to improve hospital programmes, policies and the overall quality of care of the DFCI. In addition, we worked with a marketing firm (Hill Holliday, http://www.hhcc.com) that conducted patient, family and clinician focus groups to determine acceptability of terminology, wording and format; we used these data to refine our materials.
Pilot testing the guide
We piloted the SICG with 26 practitioners—physicians from multiple specialties including internal medicine, oncology, nephrology, critical care, surgery and neurology, as well as nurse practitioners (NPs) and physician's assistants. Clinicians were given a brief overview of the project and were trained to use the conversation guide. They were then observed and audio-recorded as they conducted a discussion with a trained actor serving as a standardised patient. Clinicians first followed their usual approach to an end-of-life conversation, then were asked to use the guide's structured format. We then debriefed with the clinicians about the wording, order, structure and acceptability of the guide, as well as any other feedback. We made changes based on clinicians’ suggestions. We used the newly edited version of the SICG for the next round of interviews. We continued this cycle (approximately 3 clinicians per cycle) until our participants suggested no more significant changes to the guide (eight cycles).
Methods and analysis
Trial design
The study is a prospective, cluster-randomised controlled trial of a quality-improvement intervention. We enrol oncology physicians, NPs, physician assistants (PAs) and ambulatory patients with cancer and their identified surrogates. We are conducting the study at the DFCI, and at two affiliated satellite clinics (Dana-Farber at Milford Regional Medical Center, and Dana-Farber at South Shore Hospital). DFCI is a National Cancer Institute designated comprehensive cancer centre located in Boston, Massachusetts and part of the National Comprehensive Cancer Network. The DFCI is organised into ‘disease centres’, each of which focuses on a specific class of illnesses. Clinicians from these disease centres, except for those in gynecologic oncology department, where there is another ongoing trial that overlaps with the objectives of this one, were asked to volunteer for the study. Among the clinician volunteers (including physicians, NPs and PAs), half were randomised into the intervention group, and the other half into a control group. Physicians, NPs and PAs in the intervention group were trained in using the SICG and received ongoing coaching from the study team. The control group provides usual care. In addition, because we hypothesise that volunteer clinicians would be different from non-volunteer clinicians and would therefore have patients with different outcomes than the patients of their volunteer-colleagues, we are enrolling the patients of a third group of clinicians who did not volunteer for the study and who also provide usual care (see figure 2 for the study design).

Research design.
Participant recruitment
Clinicians
All medical oncologists who see patients at least one half day a week are eligible to participate. Study staff recruited and enrolled clinicians at disease centre meetings, by email and in person. Oncologists who declined participation received an email notifying them that their patients will be invited to participate. All volunteers received a $150 gift card.
NPs and PAs were also enrolled in the study. They were recruited and consented in the same fashion as the physicians, and also received a $150 gift card for enrolment. In order to minimise the possibility of contamination if a patient sees clinicians from both arms of the study, enrolled NPs and PAs were enrolled in the study arm of their collaborating physicians. If an NP or PA works with both intervention arm physicians and either control arm or non-enrolled physicians, they were excluded from the study.
Patients
Only patients receiving their ongoing primary oncology care at DFCI are eligible for participation in the study. Enrolment criteria include: age >18 years, English-speaking, able to consent and complete periodic surveys, and also to identify a friend or family member willing to answer surveys. Since the trial relies intensively on the clinician's communication skills about a culturally complex topic, we feel that relying on interpreters, who do not have experience with these conversations, and who have been shown to be unreliable translators of emotionally difficult material,23 ,24 might expose patients and their families to greater distress without separate testing to determine suitability. Therefore, all non-English-speaking patients were excluded from the study (see figure 3 for a visual representation of recruitment).

Patient/family recruitment and assessment.
Surrogates
Patients identify a surrogate—a friend or family member—who is able to participate in the study. The friend or family member can consent remotely and is not required to attend clinic appointments with the patient but is asked to answer surveys. The friend or family member is required to be over 18, speak English, and have the ability to provide consent. If the identified surrogate does not wish to participate, then the patient is asked to suggest another individual. If no surrogate is identified, then the patient is ineligible for the study (see figure 3 for a visual representation of recruitment).
Intervention
The intervention is a multicomponent, structured communication intervention designed to (1) identify patients at high risk of death in the next year; (2) train clinicians to use the SICG to structure advanced care planning discussion with patients; (3) ‘trigger’ the oncology clinicians to have conversations using the guide with enrolled patients; (4) prepare patients for the conversation by providing them with a letter encouraging them to think about some of the topics raised in the Guide; (5) guide clinicians in conducting values and goals conversations; (6) document outcomes of the discussion in a structured format in the EMR and (7) provide patients with a Family Communication Guide to help them continue the discussion at home with their loved ones.
Population identification
To identify eligible patients, we use a ‘No’ answer to the question, ‘Would you be surprised if this patient died in the next year?’, if the patient meets other study requirements. The ‘surprise question’ is a validated single-item method for identifying patients at high risk of dying within a year among advanced cancer and dialysis patients.25 ,26 A physician answering ‘No’ to the question ‘Would I be surprised if this patient died in the next year?’ confers an HR of death of 7.9 for patients with cancer.26 Every patient identified by a clinician with a ‘No’ response on the surprise question is invited to participate in the study by a letter with an opt-out card. If the opt-out card is not returned, a follow-up phone call is conducted to invite participation.
Recruitment in the neuro-oncology clinic is conducted using the surprise question and via review of ICD-9 codes to identify any patients with a diagnosis of a cancer that has a high mortality risk (eg, glioblastoma multiforme); those patients are deemed eligible to be approached for consent after their fourth clinic visit.
Training and coaching programme
In order to minimise time commitment for clinicians, we designed a 2.5 h training programme for intervention clinicians to develop their competencies in using the SICG21 (table 1). The training begins with a brief didactic session (<30 min) on the evidence base for ACP discussions. A demonstration and discussion of the use of the SICG (approximately 30 min) are followed by individualised practice by all participants, using role-plays with personalised feedback from attending palliative care physicians (more than 60 min). Training sessions include 6–10 participants per session. Trained actors serve as standardised patients for both the demonstration and role-play. Clinicians learn how to introduce the conversation, including: (1) orienting patients to the conversation, (2) asking for permission to discuss desires for future care, (3) reassuring patients about continued treatment, (4) stating support for the patient and family and (5) emphasising that no decisions have to be made during the initial discussion. At the end of their patient conversations, clinicians are instructed to summarise and confirm the content of the conversation, and provide patients with a Family Communication Guide (figure 4) that can encourage further discussion of issues with family members. All intervention clinicians receive the Clinician Reference Guide, which summarises information provided in the training and offers guidance on challenging scenarios. The training concludes with a tutorial for clinicians on how to access and complete the EMR documentation module. Finding the time to conduct a conversation was a significant issue discussed in the training session. Clinicians were given leeway as to how to fit the conversation into their workday. We allowed clinicians to split the conversation between several visits, that is, that one or two questions would be addressed at each visit. We advised clinicians that we would continue to remind them to conduct the conversation until all questions were complete in the EMR documentation module.
Goals of the Serious Illness Care Training Program

Family communication guide (front page only).
After each intervention clinician's first SICG conversation with a patient, a physician member of the SICP team reviews the conversation, elicits feedback from the clinician, and offers suggestions. Intervention clinicians can also contact the SICP team in person, by paging and telephone or by email to discuss their conversations. Group or individual coaching sessions on difficulties with these conversations are similarly available from the SICP physicians, both for routine and challenging cases. In these sessions, the coach asks clinicians to identify problem areas and then facilitates discussion of approaches to the challenges presented, including use of role-play.
Triggering
Trained clinicians are triggered by the research staff to have the SICG discussion with enrolled patients in an upcoming visit in two ways: (1) an email is sent the day before the visit notifying the clinician that the study patient is due for an SICG conversation and (2) on the day of the visit, a packet with the study materials (SICG, Family Guide, and a Post-Conversation form) is placed with the face sheet that is given to clinicians before each patient visit. We collect data on the number of triggers it takes to complete the intended SICG conversations.
Pre-visit letter
In order to activate patients and ensure they are prepared for the conversation, intervention patients receive a pre-visit letter (figure 5), which introduces the SICG topics to consider prior to their conversation with their clinician.

Pre-visit letter for patients.
Serious Illness Conversation Guide
The seven key elements that should be addressed with patients are shown in figure 1. These include: illness understanding, decision-making and information preferences, prognostic disclosure, patient goals and fears, views on acceptable function and trade-offs, and desires for family involvement.
Electronic medical record module documentation
We developed a structured format for documentation that aligns with the seven items of the SICG in the ACP module of our EMR (figure 6). The module is designed to remind clinicians of the key elements of the discussion, to ease the burden of documentation, and to allow other clinicians easy access to the information elicited from the conversation. Each SICG question is mirrored in the module with a free text box and checkboxes in which to record responses. This module offers a single location for all information related to patient values and preferences, and allows interdisciplinary team members to review, enter and track preferences over time. All entries automatically include identification of the date, time and author of the documentation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Electronic module of the Serious Illness Conversation Guide. (c) 2015 Epic Systems Corporation. Used with permission.
Family guide
After the conversation, the clinician gives patients a Family Guide that suggests an approach for discussing their illness and care preferences with their family.
Outcome data collection
The primary outcomes of the trial are patient receipt of goal-concordant care, and peacefulness at the end of life. Key process measures are acceptability of the SICG conversation to patients, acceptability of training to clinicians, number of triggers required to complete SICG, and frequency, timing, and quality of documentation of goals of care discussion. Secondary outcomes include: anxiety, depression, quality of life, therapeutic alliance, quality of communication, and quality of dying and death. We describe below how these outcomes will be measured. We plan to report outcomes in two phases: phase I will include key process measures and secondary outcomes and phase II will include the primary outcomes plus late secondary outcomes.
Timing of assessments
All study patients receive a baseline survey and then are surveyed every 2 months. For patients in the intervention arm, 1 week after the SICG conversation is complete, the patient is surveyed to assess their perception of the conversation, including its acceptability. Control patients are administered a parallel survey 2 months after enrolment, around the same time when patients in the intervention group would be likely to have an SICG conversation, based on pilot data prior to the randomised study. The control patients are asked about the number and content of their ACP or end-of-life discussions with their clinicians and families.
Patient measures
Table 2 lists the questionnaires and timing of administration for patients. Patients complete questionnaires by email, postal mail or phone. Demographic information includes age, gender, education, oncological disease, ethnicity and religion.
Patient measures and timing of administration
Surrogate measures
Table 3 lists the questionnaires and timing of administration for surrogates. We collect surrogate demographics including age, gender, education, ethnicity and religion. Friends/family members are surveyed every 2 months about the frequency and quality of communication with the patient about ACP and about their perception of the patient's life priorities using the Family Perception Scale. Six to 12 weeks after the patient's death, a social worker interviews the family member/friend on the phone using a modified form of the Quality of Dying and Death instrument (QODD).27–29 Additional questions from FAMCARE that address issues not covered in the QODD are included. The FAMCARE scale is a validated instrument to measure family satisfaction with advanced cancer care and can be administered to family members after the patient's death.30 We also collect the friend/family member's perceptions of the patient's achievement of self-identified goals using an adaptation of the Life Priorities measure. Prior to conducting the interview, which is audio-recorded, the social workers received a 1 h training from a bereavement specialist.
Surrogate measures and timing of administration
Clinician measures
Table 4 lists the questionnaires and timing of their administration for clinicians. At baseline, we record gender, profession (MD, NP or PA), disease centre, percentage clinical time, and years in practice, and administer questionnaires on clinician confidence in and attitudes about end-of-life conversations. The same questionnaire is administered following SICG training and will be administered at the conclusion of the study. Each time after a clinician is triggered to have a conversation, we ask them to complete a Post-Conversation Questionnaire. Clinicians provide information about prognostic communication, the length of the discussion, and whether they deviated from the SICG for any reason. For clinicians and patients who agree (a separate item on the consent form), a subset of conversations are audio-recorded. If the conversation did not take place, the same questionnaire asks clinicians to report their reasons for deferring the discussion. Clinician data also include how often we are emailed and paged for coaching by clinicians, as well as the number of one-on-one or group coaching sessions attended.
Clinician measures and timing of administration
Process measures
Table 5 describes the process measures tracked in the study. We conduct a chart review to assess frequency, timing, and quality of conversations on patients who die. We will count the number of intervention and control patients with goals-of-care conversations documented in the EMR, the extent and retrievability of documentation in the EMR (eg, is the information in the Advance Care Planning Section of the EMR, or included in a progress or other note). In addition, the timing of conversations for intervention and control patients will be reported relative to time of death. Finally, we will count the number of key elements of goals-of-care discussion (based on best practices) documented in the EMR.
Process measures: frequency, timing and quality of conversations
Evaluation of goal concordance
We could not identify a ‘gold standard’ for measurement of concordance between the patient's wishes and the care provided at the end of life; validated measures of this critical construct do not exist.31–36 Thus, we extensively reviewed existing literature on the topic, interviewed patients, and used this information to design a ‘Life Priorities’ survey for patients and a ‘Family Perceptions’ survey for identified surrogates. The Life Priorities survey evaluates patient priorities before death and the extent to which those priorities are subsequently achieved. The Family Perception survey assesses the extent to which the identified surrogate understands the patient's priorities while the patient is alive, and the extent to which those priorities were achieved in the last week and last 3 months of the patient's life, and also asks specific questions about the care received in the months, weeks and days before death. The last patient-reported Life Priorities survey before death will be used as the primary outcome. We have included two additional validated questions in the patient surveys, and we will compare these responses to those from our Life Priorities Scale to evaluate the validity of our measure.37
To determine the extent to which patients receive care that is consistent with their top life priorities in the last 3 months and last week of life, we will compare the patient's top three ranked life priorities to the patient's care experience at the end of life using family perception of patient's achievement of goals and medical record review. Using that information and the scoring system of 0, 1, 2 or 3 corresponding to the number of these top three goals that are met at the end of life, a team of independent, blinded physicians will determine the extent of goal concordance.
Peacefulness
The validated PEACE scale, or the ‘Peace, equanimity and acceptance in the cancer experience’ scale, will be used to measure patient peacefulness at the end of life. The PEACE instrument contains two subscales, ‘Peaceful acceptance of Illness’ and ‘Struggle with Illness’. The ‘Peaceful acceptance of Illness’ subscale will be used as the main outcome.38
Secondary outcomes
We examine patient anxiety using the validated Generalized Anxiety Disorder (GAD-7)39 ,40 and evaluate depression using the validated Patient Health Questionnaire (PHQ-9).41 We measure therapeutic alliance using the Human Connection Scale.42 The Human Connection Scale is a valid and reliable measure of therapeutic alliance between patients with advanced cancer and their physicians.42 We assess patient perception of the quality of communication with their clinician32 ,43 using the ‘Quality of Communication’ (QOC) scale, a 13-item validated questionnaire that measures the quality of end-of-life communication in two scales: a six-item ‘general communication skills’ scale and a seven-item ‘communication about end-of-life care’ scale.44 We measure quality of life and general physical health function by the SF-12 V2 health survey.45 It consists of 12 items and provides scores for both overall physical and mental health. We use the Brief R-COPE, a 6-item measure that assesses positive religious (PRC)/spiritual methods of coping and dealing with life stressors, and negative religious (NRC)/spiritual methods of coping that are representative of the religious struggle when dealing with life stressors.46
Sample size
Power calculations were performed for the two primary aims of the study: comparison of enhanced goal-consistent care and comparison of the PEACE measure across the randomised arms. In order to ensure an overall 5% type I error rate for the two primary aims, we will use a 2.5% type I error rate for each of the two primary hypotheses. Both aims are based on patient death; we expect to follow each patient for at least 1 year from randomisation, or until death if <1 year from randomisation. The power calculations below are based on having 200 evaluable patients per arm. We allow for 6% unevaluability due to patient dropout, meaning a total of 426 patients (213 per group) will be accrued at an estimated accrual rate of 200 patients per year. Given that each patient must be followed for at least 1 year from randomisation, we expect the study to be open for at least 3 years.
Primary aim 1
Enhanced goal-consistent care: The outcome for a patient will be a score of 0, 1, 2 or 3 corresponding to the number of the top three high priority goals that are met in the last week and 3 months of life. Based on previous data, the SD of ‘number of high priority goals met’ is conservatively estimated to be 1.35, and we expect the average ‘number of high priority goals met’ to be at least 0.6 point higher with the SICG (a clinically important increase based on prior studies). The two arms will be compared using a robust generalised estimating equations (GEE) Wilcoxon rank-sum-type score test47 for ordinal categorical data; this approach does not assume normality of the outcome, and accounts for a possible cluster effect of patients within clinician. Using the GEE Wilcoxon rank-sum score test with a two-sided type I error rate of 2.5% and 200 evaluable patients per arm, we have over 80% power to detect an average 0.6 point higher average score in the SICG arm. In this power calculation, an intracluster (clinician) correlation coefficient (ICC) of approximately 0.1 has been assumed, as is (conservatively) commonly used in this type of cluster randomisation study.48
Primary aim 2
PEACE scale: From previous data,38 the SD of the ‘Peaceful acceptance subscale’ is conservatively estimated to be 3.3 (‘conservatively’, since this is the largest SD found in Mack et al38), and we expect the average score to be at least 1.3 points higher with the intervention (again, a clinically important increase based on prior studies). The two arms will be compared using the GEE Wilcoxon rank-sum score test accounting for clustering of patients within clinician. Using a GEE Wilcoxon rank-sum score test with a two-sided type I error rate of 2.5% and 200 evaluable patients per arm, we have over 80% power to detect a 1.3-point higher average ‘Peaceful acceptance subscale’ in the intervention arm, assuming the ICC=0.1.
Interim analysis/early stopping rules
For primary aims 1 and 2, the trial will be monitored for possible early stopping due to a large intervention effect using a Haybittle-Peto approach.49 Specifically, one interim GEE Wilcoxon rank-sum score test will be performed after approximately 50% of the total patients are enrolled, which should occur approximately 6 months after baseline and with 213 patients. In order to stop the study at this point in favour of the SICG arm, the p value for GEE Wilcoxon rank-sum score test must be <0.001. The power calculations above take into account the possibility of one interim analysis. The stopping rule for this study will be used as a guideline rather than as a hard-and-fast rule. Any final decision will also consider additional end points such as differences in complications and process measures. If the findings of the interim analysis are in favour of stopping the trial due to beneficial effect of the SICG, the research study will be stopped. We note here that we used a simpler conservative interim analysis approach49 because the less conservative approaches50 require independent increments of data; however, the data will not likely come to us in independent increments because of the cluster randomised design. Further, as we have chosen a conservative interim analysis approach, the one interim analysis can be performed at any time during the study, and the stopping rule of p<0.001 still applies.
Randomisation
The oncologists are stratified by disease centre or satellite facility. The strata correspond to the disease centres (breast, gastrointestinal, genitourinary, leukaemia, lymphoma, thoracic, sarcoma, head & neck, neuro-oncology) and two satellite facilities. The smallest disease centre, melanoma, was not randomised because cross contamination would be likely due to its small size; it served as a pilot site. Clusters are organisational units of clinicians within a disease centre; a typical cluster would have one NP and 2–3 physicians, although the numbers of particular clinicians vary across disease centres; randomisation was carried out by cluster.
Within strata, one-half of the clusters were randomised to the intervention and one-half of the clusters were randomised to standard care. The cluster is randomly assigned to intervention or control based on a random number drawn in SAS. The GEE statistical methods described in the power calculations take into account the stratification (disease centre) and clustering (clinicians) variables in the analysis.
Blinding
For the telephone bereavement interviews, social workers who are not involved in the study conduct the interviews and are blinded to the study arm of the patient and surrogate (intervention vs control).
Planned analytic approach
The objective of this study is to evaluate whether, for patients with cancer, the SICP is better than usual care at helping patients achieve healthcare goals and quality of life in the setting of serious illnesses. The design is a cluster-randomised controlled trial in which patients are nested within clinician clusters. One-half of the oncology clinicians are randomised to the SICP and one-half of the oncology clinicians are randomised to standard care. Since this is a randomised trial with stratification by disease centre prior to randomisation, we expect the demographic characteristics and other possible confounders (age, disease severity, etc) to be similar in the two groups. However, since randomisation is at the cluster-level and there are 50 total clusters, there is a slightly greater chance that characteristics will not balance out than if randomisation was done at the patient level. Prior to evaluating the effect of the intervention, the demographic characteristics of test arms will be compared by the Rao-Scott χ2 (accounting for stratification by disease centre and clustering by oncology clinician) for discrete variables, and by the GEE Wilcoxon rank-sum score test for ordered categorical variables and continuous variables (accounting for stratification by disease centre and clustering by oncology clinician).47 If, as expected, there are no differences in demographic or other confounders, the primary outcomes across arms will be compared using the GEE Wilcoxon rank-sum score test for ordered categorical variables and continuous variables (accounting for stratification by disease centre and clustering by oncologist).47
If baseline differences are found between the two arms with respect to important confounders (such as age, race, comorbidities), the GEE Wilcoxon rank-sum test will incorporate propensity weights. In particular, to conduct the propensity score adjustment, we will use a logistic regression model to calculate the propensity (probability) of being in the intervention or control groups based on all possible confounders, and then weight each participant in the GEE Wilcoxon rank-sum score test based on the inverse propensity of being in one of the two treatment groups.51 This study evaluates the impact of the entire intervention, and will not address which components of this multicomponent programme are effective.
Ethics and dissemination
Ethical review
All participants provide informed consent and may withdraw at any time without impacting their treatment or relationship with their clinical team. An approved protocol to monitor for adverse events is followed and additional support for patients with symptoms of psychological distress is available through the Palliative Care and Psychosocial Oncology clinical programmes. Additionally, we monitor patient responses to the PHQ-9 measure of depression whenever these responses are collected. If the patient answers ‘More than half the days’ or ‘Nearly every day’ to the question, ‘Thoughts that you would be better off dead, or of hurting yourself’, or if the patient responses indicate severe depression (PHQ-9 score of 20 or greater), we immediately notify the patient's NP or physician by pager or phone. We also monitor the GAD-7 measure of anxiety and the pain score to screen for the following indicators of patient distress: severe anxiety (GAD-7 score of 15 or greater), and severe pain (level of 8 or greater). When any of these conditions are met, we notify the patient's NP or physician by email within 24 h.
Relevance and dissemination
The design of the SICP addresses critical deficiencies in the conduct of end-of-life conversations. The SICP, if successful, provides a simple, scalable structure to support oncology physicians, NPs and PAs in conducting state-of-the-art serious illness conversations with a broad array of oncology outpatients at a high risk of dying within a year. We do not know the generalisability to other populations of seriously ill patients, such as those with congestive heart failure or chronic obstructive pulmonary disease. Likewise, we are limited to analysing the data of the patients who agreed to participate in the trial and cannot characterise patients who opted out, who might be less willing to discuss these issues.
The Conversation Guide, while not comprehensive, has been designed to balance brevity to enhance scalability, while at the same time addressing the issues that matter most to patients. The length of the clinician training (2.5 h) was chosen as an acceptable amount of time that would be feasible for many healthcare systems to adopt, if successful. We anticipate that clinician training will improve the quality of these conversations, and that enhancing clinician confidence, knowledge, and skill, the lack of which are known barriers to ACP, will increase the frequency of effective serious illness conversations. By triggering the conversations early in the course of the illness, our goal is for patients with serious illness and their families to be able to consider decisions about their lives and choices about medical care with adequate time for reflection and discussion. The design of the EMR module creates a repository of information about patient values and goals, reinforces use of the SICG, reduces time needed to record information, and communicates patient goals and values in a readily accessible place in the EMR that is easily retrievable by other clinicians, especially in an emergency.
Our ultimate aim is to determine if we can provide a proven means for transforming end-of-life care through an innovative model that enables patients with serious illness and non-palliative care clinicians to discuss preferences for end-of-life care more often, earlier, and more effectively. We believe that developing scalable models for improving serious illness conversations will contribute to better alignment of healthcare with the preferences of oncology patients, and eventual extension to other patient populations and care settings.
References
Footnotes
Twitter Follow RACHELLE E. BERNACKI at @rbernack
Contributors SDB is the Director and Principal Investigator of the Serious Illness Care Program. RB is the Project Director and has been centrally involved in all aspects of the trial, including the development of the study protocol. MH is study coordinator and has the primary responsibility of coordinating development of the study materials, and contributed to the development of the protocol. JV, GS and JP contributed to the development of the materials as well as the protocol. SL is the primary biostatistician for the study. AAG and SDB obtained funds for this trial; AAG also serves as a senior advisor and co-investigator for the project. All authors reviewed and approved the manuscript. AAG receives royalties from multiple publishers and media outlets for essays, books, and films on improvement of healthcare, including those on end-of-life care.
Funding This work was supported by the Charina Endowment Fund, Partners Healthcare, and the Margaret T. Morris Foundation. RB is supported by Health Resources Services Administration grant K01HP2046.
Competing interests None declared.
Ethics approval The study was approved by the Dana-Farber Cancer Institute Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.