Article Text

Abstract
Objective To investigate the association of the duration of use of prescription medications and nicotine replacement therapy (NRT) with smoking cessation using a national sample of the general population in the USA, controlling for nicotine dependence and sociodemographic variables.
Setting USA.
Participants We used data from the 2010–2011 Tobacco Use Supplement to the US Current Population Survey. We limited the analysis to current daily smokers who made a quit attempt in the past year and former smokers who were a daily smoker 1 year prior to the survey (n=8263). Respondents were asked about duration of use of prescription medication (varenicline, bupropion, other) and NRT (nicotine patch, gum/lozenges, nasal spray and inhaler) for smoking cessation.
Primary outcome measure Successful smoking cessation. Individuals who reported to have smoked at least 100 cigarettes in their lifetime but were not smoking at all at the time of the interview and were a daily smoker 1 year prior to the interview were considered to have successfully quit smoking.
Results After adjusting for daily cigarette consumption and sociodemographic covariates, we found evidence for an association between duration of pharmacotherapy use and smoking cessation (p<0.001). Adjusted cessation rates for those who used prescription medication or NRT for 5+ weeks were 28.8% and 27.8%, respectively. Adjusted cessation rates for those who used prescription medication or NRT for less than 5 weeks varied from 6.2% to 14.5%. Adjusted cessation rates for those who used only behavioural counselling and those who attempted to quit smoking unassisted were 16.1% and 16.4%, respectively.
Conclusions Use of pharmacotherapy for at least 5 weeks is associated with increased likelihood of successful smoking cessation. Results suggest that encouraging smokers who intend to quit to use pharmacotherapy and to adhere to treatment duration can help improve chances of successful cessation.
- PREVENTIVE MEDICINE
- PUBLIC HEALTH
- SOCIAL MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This was the first population-based study to examine the association between the duration of use of prescription medication as well as nicotine replacement therapyNRT for smoking cessation and successful smoking cessation, controlling for nicotine dependence and sociodemographic variables.
A strength of this study was that it used a large nationally representative sample with a relatively high response rate.
Our results strengthen the findings of clinical trials on the efficacy of pharmacotherapy for smoking cessation and indicate that these aids might also be successful in the general population if they are used for at least 5 weeks.
A strong possibility of reverse causation such that relapse would determine duration of pharmacotherapy use rather than vice versa, was a major limitation of this study. Recall bias, especially related to the smokers’ previous quit attempts, and the observational nature of the study precluding the establishment of a causal link between the duration of pharmacotherapy use and successful smoking cessation, were the other limitations.
Introduction
Clinical trials provide strong evidence that pharmacotherapy for smoking cessation, including various forms of nicotine replacement therapies (NRT), bupropion or varenicline, greatly increases the chances of a successful smoking cessation attempt.1 ,2 However, observational population-based studies have shown mixed results. While some have shown that pharmacotherapy increases smoking cessation rates,3–6 others have concluded the opposite.7–11 Yet, other population-based studies have shown no difference in cessation rates between those who use and those who do not use pharmacotherapy.12 ,13 The population-based reports that have found no favourable effect of pharmacotherapy have been criticised for not controlling for nicotine dependence,14–16 which is a predictor of abstinence and is usually higher among smokers who choose to use pharmacotherapy for smoking cessation.4 ,14 ,17 ,18 Some of the analyses that have controlled for nicotine dependence have found a favourable effect of pharmacotherapy on smoking cessation,3 ,4 ,19 but others have not.7
An additional confounder that rarely is taken into account in population-based studies is duration of use of pharmacotherapy, which has been found to be associated with treatment success in clinical trials.20–22 We know of one population-based study that examined the association of duration of use of pharmacotherapy with smoking cessation and found no association.12 This study was conducted in the USA where NRT can be purchased over the counter, and medications such as bupropion and varenicline can only be obtained as prescription drugs.
While clinical trials have high internal validity and can provide evidence for the efficacy of pharmacotherapy, observational population-based studies can address effectiveness of these therapies under conditions that they are intended to be used.14 Furthermore, while clinical trials provide confidence in causal associations, population-based studies are strong in representativeness and external validity. Thus, both are needed to advance the science of smoking cessation.19
There is no literature on population-based studies that examine the association of duration of NRT and prescription medication use with smoking cessation. Our aim was to use a large representative sample of the general population in the USA and investigate the association of the duration of use of prescription medications and NRT with smoking cessation, controlling for nicotine dependence and sociodemographic variables.
Methods
Data
We used data from the 2010–2011 Tobacco Use Supplement to the Current Population Survey (TUS-CPS), sponsored by the National Cancer Institute and administered by the US Census Bureau in May 2010, August 2010 and January 2011.23 The TUS-CPS is administered as a part of the CPS, which is a monthly national survey of representative households by the US Census Bureau and the Bureau of Labor Statistics.24 The TUS-CPS utilises a multistage probability sampling of individuals 15 years and older, from a sample of approximately 56 000 housing units, in turn selected from 792 primary sampling units. The average response rate for CPS for the 3 months of surveys used in this study was 93%, whereas for the TUS it was 63%.
Measurement
Successful smoking cessation
Individuals who reported to have smoked at least 100 cigarettes in their entire life but were not smoking at all at the time of the interview and were a daily smoker 1 year prior to the interview (‘Around this time 12 months ago were you smoking every day… ?’) were considered to have successfully quit smoking (n=1769). Those who reported to have quit within the last 4 weeks were excluded from the analysis (n=322). Individuals who reported to have smoked at least 100 cigarettes in their entire life, were smoking every day at the time of the interview and had made a quit attempt in the past year were considered to have failed in their quit attempt (n=7304). Individuals who reported to have used both prescription medication and NRT for smoking cessation were excluded from the analysis (n=488), because after subdividing this group by categories of duration of use for prescription medication and NRT, some of the subgroup sample sizes were extremely small. The total sample size for the study was 8263 respondents, consisting of 1379 who successfully quit smoking and 6884 whose quit attempt was not successful.
Assisted quit attempt and duration of pharmacotherapy use
Daily and former smokers were both asked in three separate questions to indicate whether, in their last quit attempt in the past year, they used a prescription pill called (1) Chantix or varenicline, (2) zyban, bupropion or wellbutrin or (3) other prescription pills. They were also asked in three separate questions to indicate whether, in their last quit attempt in the past year, they used (1) a nicotine patch, (2) nicotine gum or nicotine lozenge or (3) nicotine nasal spray or nicotine inhaler. They were also asked to indicate how many days, weeks or months they used these prescription and/or NRT medications. Furthermore, daily and former smokers were both asked three separate questions about use of behavioural counselling in their last quit attempt in the past year. They were asked if they used (1) a telephone helpline or quitline, (2) one-on-one counselling or (3) a stop smoking clinic, class or support group. Based on the questions about use of prescription medication, NRT and behavioural counselling, we created the following two categorical variables:
Method of quit attempt
Prescription medication only;
Prescription medication and behavioural counselling;
NRT only;
NRT and behavioural counselling;
Behavioural counselling only;
Unassisted.
Duration of use of pharmacotherapy
Prescription medication: 5+ weeks;
Prescription medication: 3–4 weeks;
Prescription medication: 1–2 weeks;
NRT: 5+ weeks;
NRT: 3–4 weeks;
NRT: 1–2 weeks;
Behavioural counselling only;
Unassisted.
We categorised duration of use of pharmacotherapy based on a systematic review of studies assessing adherence to smoking cessation medication.20 In categorising duration of use, we made no distinction between whether or not the medication was combined with behavioural counselling as this distinction was inconsequential in the analysis.
Statistical analysis
We used multivariable logistic regression models to compute adjusted ORs for the association of the method of quit attempt and duration of use of pharmacotherapy with successful smoking cessation. Sampling weights were taken into account in the computation of parameter estimates. We computed p values using the jackknife, which is an unbiased estimator for a statistic and a data-dependent method to calculate SEs.25 All models controlled for daily cigarette consumption (current daily consumption among daily smokers and daily consumption 12 months ago among former smokers), age, race/ethnicity, education, occupation and family income. In order to account for the missing income data, CPS uses one of the three imputation methods, relational imputation, longitudinal edits or hot deck allocation. Details of these methods are described elsewhere.26 In multivariable logistic regression models, we omitted observations that had a missing value for any of the covariates. This constituted 1.7% of the full sample in the analysis pertaining to the method of quit attempt (n=142) and 6.3% of the full sample in the analysis pertaining to duration of pharmacotherapy use (n=491). We used the logistic regression results to compute adjusted cessation rates by method of quit attempt and duration of use of pharmacotherapy. These adjusted rates were computed by fixing covariates at their means in the fitted models.27
Results
Sample characteristics and bivariate associations
Weighted sample characteristics are shown in table 1. About 66.7% of the sample reported to have made an unassisted quit attempt; 10% used only prescription medication; 1.1% used prescription medication plus behavioural counselling; 18.2% used only NRT; 2.5% used NRT plus behavioural counselling; and 1.3% used only behavioural counselling. When broken down by duration of use, while most of those who used prescription medication did so for five or more weeks, the great majority of those who used NRT did so for 2 weeks or less. The reported number of cigarettes smoked per day was 14 or less for about 54.5% of the sample. Age was distributed with 11.8% of the sample under 25 years of age, 33% between 25–39 years, 32.3% between 40–54 years and 22.8% 55 years or older. The sample was 76% non-Hispanic white, 11.3% non-Hispanic Black, 7.4% Hispanic and 5% of other race/ethnicity. About 15.2% of the sample did not have a high school diploma, 73.3% had a high school diploma and 11.4% had at least a bachelor's degree. The distribution of family income was skewed such that over a third of the sample had an income of less than $25 000 and less than a 10th of the sample had an income of $100 000 or greater.
Weighted sample characteristics and unadjusted smoking cessation rates across categories of each covariate
Table 1 also provides smoking cessation rates across categories of each covariate, indicating bivariate (unadjusted) associations between the covariates and quitting. Cessation rate was 17% in the whole sample. There was very little evidence that method of quit attempt was associated with cessation rate (p<0.074). However, the duration of pharmacotherapy use (p<0.001), number of cigarettes smoked per day (p<0.001), age (p<0.001) and race/ethnicity (p=0.003) were all associated with quitting. Higher socioeconomic status as measured by education, occupation and income, was associated with a higher cessation rate (p<0.001 for all three indicators of socioeconomic status). Sex had no association with cessation.
Adjusted results from multivariable logistic regression models
Table 2 provides adjusted ORs for the association of method of quit attempt with the probability of smoking cessation. Figure 1 shows the adjusted cessation rates for various quitting methods. Unlike the unadjusted results in table 1, which provided very little evidence of an association between quitting method and successful cessation, the adjusted results revealed some evidence of an association (p=0.025). The highest cessation rate was among those who used prescription medication and behavioural counselling (20.4%) followed by those who used NRT and behavioural counselling (17.4%), attempted to quit unassisted (16.4%), used behavioural counselling only (16.1%) and those who used prescription medication only (15.3%). The lowest cessation rate was among those who only used NRT as a quitting method (12.3%).
Adjusted* ORs and 95% CIs for the association of method of quit attempt and duration of pharmacotherapy use with the probability of successful smoking cessation
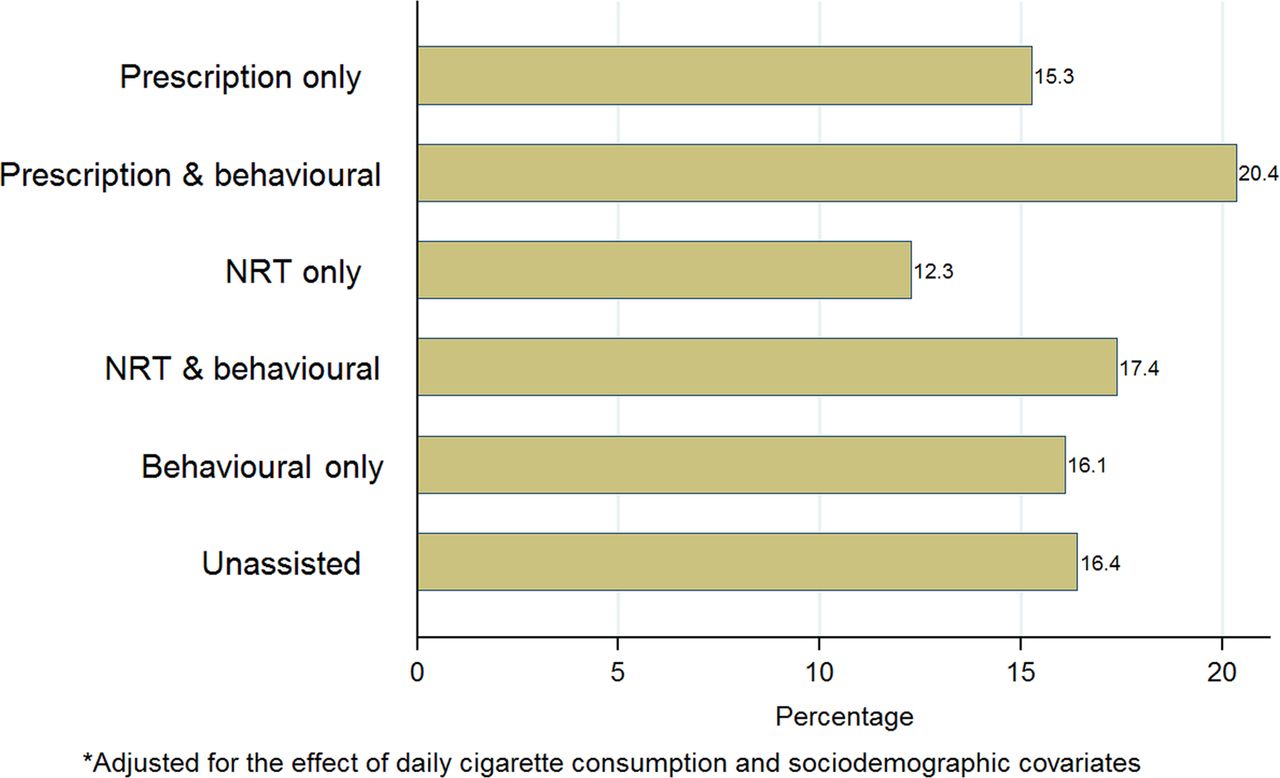
Adjusted cessation rate by method of quit attempt.
Table 2 also provides adjusted ORs for the association of duration of pharmacotherapy use with the probability of smoking cessation. Figure 2 shows the adjusted cessation rates for various durations of pharmacotherapy use. Consistent with the unadjusted results in table 1, the adjusted results in table 2 also provide evidence (p<0.001) of an association between duration of pharmacotherapy use and successful cessation. As shown in figure 2, cessation rates were highest among those who used prescription medication for 5+ weeks (28.8%) and those who used NRT for 5+ weeks (27.8%). Cessation rates for those who used prescription medication or NRT for less than 5 weeks varied from 6.2% to 14.5%. Cessation rates for those who used only behavioural counselling and those who attempted to quit smoking unassisted were 16.1% and 16.4%, respectively.

{kind=link}
{kind=link}
Adjusted cessation rate by duration of pharmacotherapy use.
The results pertaining to the association of other covariates with successful cessation were very similar in the multivariable regression models for method of quit attempt and duration of pharmacotherapy use. These results were consistent with bivariate associations reported above, except for the fact that there was very little evidence for an association of race/ethnicity and smoking cessation in multivariable analyses.
Discussion
This is the first population-based study to examine the association of successful smoking cessation and duration of use of prescription medication as well as NRT for smoking cessation. We found that using pharmacotherapy for 5 weeks or longer is associated with a higher probability of cessation compared to using pharmacotherapy for shorter durations, only using behavioural counselling or trying to quit unassisted.
Our findings are consistent with the results of a study of a hospital-based cessation programme where participants who used NRT for 5 weeks or longer were found to have a higher cessation rate at 6 month follow-up.28 However, our findings are not consistent with those of a population-based study that did not find any evidence that using NRT for more than 6 weeks versus not using NRT at all was associated with smoking cessation.12 In that study, the survey response rate was low, the sample size was small and prescription medications were not examined. These factors could explain the discrepant findings.
While we found that smokers who used pharmacotherapy for at least 5 weeks have a far more favourable outcome than others, only 11% of the sample was in this group and notably about 70% of the sample did not use any pharmacotherapy for smoking cessation. Previous research indicates that barriers to the use of these cessation aids include concerns with their addictiveness, cost and side effects, as well as the belief that no treatment of any kind is needed to quit smoking.29–31
A major limitation of the study is that there is a strong possibility of reverse causation such that relapse would determine duration of pharmacotherapy use rather than vice versa.32 Smokers who use varenicline to quit smoking are asked to completely stop smoking 1 week after their quit date.33 Thus, individuals who use pharmacotherapies and relapse a short while after a quit attempt may stop using these aids. In such cases, an unsuccessful quit attempt would cause a short duration of pharmacotherapy use instead of the reverse. Furthermore, because of its observational nature, our study cannot establish a causal link between the duration of pharmacotherapy use and successful smoking cessation. While our analyses controlled for several important predictors of cessation including daily cigarette consumption, age, race, education, occupation and income, it is possible that there might be residual confounding related to variables such as depression, anxiety, alcohol use and financial stress.34 ,35 Such confounding would further weaken the ability of the study to imply causation.
Another weakness of the study relates to the fact that smokers forget many quit attempts7 ,36 and they are more prone to recall attempts that used pharmacotherapy than those that did not.14 ,17 Such recall bias can underestimate the success rate of attempts at quitting with the aid of pharmacotherapy.17
A strength of this study was that it used a large nationally representative sample with a relatively high response rate. This was the first time that questions about the duration of pharmacotherapy use were included in the TUS-CPS. We know of no other national data on the general population that provide information on this variable. Many population-based studies of pharmacotherapies for smoking cessation have found these aids to be ineffective. It is likely that if these studies were able to account for duration of use, their findings would have been different. However, data on duration of use are not routinely collected and a large sample size would be required to provide a reliable estimate of the effect of using these medications for duration of a few weeks. Nonetheless, it would likely be an important area for further research to establish the relationship between duration of use of pharmacotherapy and successful quitting in the general population.
Our results strengthen the findings of clinical trials about the efficacy of pharmacotherapy for smoking cessation and indicate that these aids might also be successful in the general population if they are used for at least 5 weeks.
References
Footnotes
Contributors MS was instrumental in conceptualisation of research study, data analysis and writing of the initial draft of the manuscript. RAS and MM contributed in the development of study, data analysis and preparation of the results section. They also helped with writing the manuscript and editing it for final submission. ASK helped with literature review, provided inputs for the materials and method section, and contributed to writing and editing the manuscript. MT was involved with literature review and data analysis, and provided her inputs to the entire manuscript. GKS was involved with formulation of research study, and helped in the data analysis and contributed in the writing and editing of the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.