Article Text

Abstract
Introduction Success in the treatment of young people with cancer, as measured conventionally by survival rates, is mitigated by late effects of therapy that impose a burden of morbidity and limit life expectancy. Among these adverse sequelae are altered body composition, especially obesity, and compromised bone health in the form of osteoporosis and increased fragility. These outcomes are potentially reversible and even preventable. This study will examine measures of body composition and bone health in long-term survivors of acute lymphoblastic leukaemia (ALL) in childhood and adolescence. These measures will be complemented by measures of physical activity and health-related quality of life (HRQL).
Methods and analysis Survivors of ALL who are at least 10 years from diagnosis, following treatment on uniform protocols, will undergo measurements of body mass index; triceps skin fold thickness and mid-upper arm circumference; fat mass, lean body mass, skeletal muscle mass and bone mineral density by dual energy X-ray absorptiometry; trabecular and cortical bone indices and muscle density by peripheral quantitative CT; physical activity by the Habitual Activity Estimation Scale; and HRQL by Health Utilities Index instruments. Descriptive measures will be used for continuous variables and number (percent) for categorical variables. Associations between variables will be assessed using Fisher's exact t test and the χ2 test; correlations will be tested by the Pearson correlation coefficient.
Ethics and dissemination The study is approved by the institutional research ethics board and is supported by a competitive funding award. Dissemination of the results will occur by presentations to scientific meetings and publications in peer-reviewed journals, and by posting summaries of the results on websites accessed by adolescent and young adult survivors of cancer.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Treatment of young people with cancers has become increasingly successful in high-income countries as exemplified by 5-year survival rates for children, adolescents and young adults (0–29) in Canada of greater than 80%.1 ,2 This success has produced estimates such as—1 in 680 people aged 20–50 years in the USA is a survivor of cancer in childhood.3 However, the majority of these survivors experience long-term sequelae of therapy which increase in prevalence and severity with advancing age4 and result in shortened life expectancy.5 In the case of acute lymphoblastic leukaemia (ALL), the commonest form of cancer in children and adolescents, the 5-year survival rate now approximates 90%6 and is associated with numerous ‘late effects’. These include obesity, a component of the ‘metabolic syndrome’,7 and reduced bone mineralisation that can result in frank osteoporosis8; both disorders contribute to diminished physical activity and carrying the burden of morbidity and mortality.
Recognition of these hazards has led to guidelines for long-term follow-up of survivors, such as those developed by the Children's Oncology Group,9 which are undergoing international harmonisation.10 However, such guidelines have been based largely on expert opinion, with accumulating hard supporting evidence. In our ongoing work to generate such information we are examining in detail the body composition, in terms of fat and muscle compartments, and bone health with a focus on the trabecular component and osteal strength in long-term survivors of ALL in childhood and adolescence. These investigations are being complemented by measures of physical activity and health-related quality of life (HRQL) to assess the impact of related morbidities on these young people.
Overall objectives
The overall objective of this cross-sectional study is to evaluate global musculoskeletal health and body composition in survivors of ALL in childhood who are at least 10 years from diagnosis.
Aims
1. To evaluate body composition
Estimation of total body fat mass as measured by body mass index (BMI), triceps skinfold thickness (TSFT) and dual energy X-ray absorptiometry (DEXA), and exploration of the correlation of BMI and TSFT with fat mass as measured by DEXA.
Estimation of lean body mass (LBM) and skeletal muscle mass (SMM) as measured by mid-upper arm circumference (MUAC) and DEXA, and muscle composition as measured by peripheral quantitative CT (pQCT), and exploration of the correlations of MUAC with LBM and SMM, and of SMM with muscle composition.
2. To evaluate bone health
Estimation of bone mineralisation as measured by DEXA and exploration of the correlation of lumbar spine bone mineral density (LS-BMD) with trabecular volumetric BMD as measured by pQCT.
Estimation of bone integrity as measured by pQCT and exploration of the correlation of the strength-strain index (SSI) with the occurrence of fractures.
3. To evaluate physical activity as measured by the Habitual Activity Estimation Scale (HAES) and explore the impact of body composition and bone health on physical activity.
4. To evaluate the HRQL and explore the impact of body composition and bone health on HRQL.
A priori hypotheses are as follows:
Body composition
Long-term survivors of ALL in childhood and adolescence will have excessive fat mass, reflected in BMI, TSFT and DEXA, compared to population norms.
Long-term survivors of ALL in childhood and adolescence will have low muscle mass, reflected in MUAC and DEXA (LBM and SMM), as well as altered muscle composition as reflected in pQCT, compared to population norms.
Bone health
Long-term survivors of ALL in childhood and adolescence will have reduced bone mineralisation with an increased risk of fracture compared to population norms, reflected in LS-BMD Z and T scores from DEXA, and trabecular volumetric bone density and SSI from pQCT.
Long-term survivors of ALL in childhood and adolescence will have defective bone integrity, reflected in reduced network connectivity and increased maximal hole sizes on pQCT.
Other measures
Long-term survivors of ALL in childhood and adolescence will exhibit low physical activity, as measured on the HAES, compared to population norms.
Long-term survivors of ALL in childhood and adolescence will display a greater burden of overall morbidity, reflected in Health Utilities Index (HUI) scores of HRQL, than in the general population.
Methods and analysis
Study participants
The study participants are all survivors of ALL who are more than 10 years from diagnosis and therefore, likely to be cured.11 Between 1 January 1985 and 31 December 2004 there were 221 patients diagnosed with ALL who were following or enrolled on Dana-Farber Cancer Institute (DFCI) therapeutic protocols that follow a common structure.12 Of these, 5 had Down syndrome, 22 relapsed and 38 died. From the remaining 183, a total of 172 (94%) were enrolled in the Aftercare long-term follow-up clinic at a single institution, McMaster Children's Hospital (MCH) in Hamilton, Ontario, Canada. MCH was the first Canadian institution to join the DFCI Childhood ALL Consortium, in 1985. We have demonstrated previously that, as a group, children and adolescents so treated manifest excessive weight gain, reflected in BMI13 with a disproportionate increase in fat mass14 accompanied by loss of bone mineral content, represented by reduced LS-BMD,15 by the end of the 2-year programme of therapy. The current study is exploring whether those trajectories are sustained or modified among long-term survivors.
Eligible participants (n=172) were 1–17 years of age at diagnosis with any form of ALL. Those with Down syndrome and those who experienced a relapse, even if ‘salvaged’ by second-line chemotherapy, were excluded. Participants are completing all elements of the study during the single day that encompasses their annual visit to the Aftercare clinic. The study has a cross-sectional cohort design.
Body composition
Body composition is being assessed in three ways
Height in centimetres (cm) and weight in kilograms (kg) are measured in standard fashion and used to determine BMI (weight/height squared) which is recorded in centiles for participants less than 18 years of age and in absolute values for those 18 years and older. Being overweight is defined as having a BMI between the 85th and 95th centiles or an absolute value of 25–29, while obesity is defined as at or above the 95th centile or an absolute value of 30 or greater.16 ,17 Although imperfect, BMI provides an acceptable measure of excessive fat mass.18 As was concluded in a recent meta-analysis, “Additional evidence is needed to determine whether obesity is persistent in long-term ALL survivors.”19
Arm anthropometry is performed as described previously20 and yields measures of MUAC and TSFT. MUAC provides an estimate of fat-free mass, which is very similar to LBM, while TSFT yields an estimate of fat mass. We have used arm anthropometry to determine nutritional status in a large sample of Central American children and adolescents with cancer at diagnosis.20 MUAC is measured to the nearest millimetre. With the forearm held at a right angle, a mark is made at the mid-point of the upper arm between the olecranon process of the ulna and the acromial process of the scapula. A paper measuring tape is passed around the arm at the mark. The measurements are repeated twice and the mean of the three measurements is used for analysis. TSFT is measured using a Harpenden calipre (John Bull British Indicators Ltd, England) to the nearest 0.2 mm in the posterior line with the arm hanging loosely at the same level as the site used for the MUAC and by lifting the skin and fat away from underlying muscle with one hand and applying the calipre blades to either side of this fold of skin. The reading is determined 2–3 s after the full pressure of the jaws has been exerted. The measurement is repeated twice within 1 mm of the previous one and the mean of the three measurements is used for analysis. The results of MUAC and TSFT are compared with age and sex-matched norms,21 ,22 and expressed as Z scores. The reproducibility of anthropometry has been established in children23 and adults.24
DEXA has been described by the International Society for Clinical Densitometry as “the most commonly used bone densitometric technique for children throughout the world, preferred over other techniques because of its speed, precision, safety, low cost, and widespread availability.”25 DEXA scans give accurate measures of whole body fat mass, LBM and bone mineral content that sum almost exactly to body weight.26 DEXA scans are being performed with a Hologic Discovery A densitometer (Hologic, Waltham, Massachusetts, USA) that exposes the participants to 1–5 μSv of radiation, less than that of a standard posteroanterior chest X-ray.27 DEXA scans are also being used to provide a measure of SMM; we have undertaken this previously in children and adolescents with ALL on therapy28 to allow correlations to be drawn with other study variables, including physical activity. Whole body SMM is related directly to appendicular lean tissue mass;29 therefore, it can be derived from the latter that is extractable from the whole body DEXA scans.28 We have derived normal reference values for SMM.30 Deficits in muscle strength and mobility have been described in adult survivors of ALL in childhood.31 However, the relationship of SMM and mobility is unknown.
Bone health
Bone health is being assessed in two ways
DEXA provides measures of LS-BMD. These are provided as Z scores, based on locally generated normative data32 and adjusted for height and weight33 in participants less than 18 years of age. For older participants these are provided as T scores. In both instances osteopenia is classified as scores between −1 and −2, and in osteoporosis the scores are −2.5 or lower, although a cut-off of −2 has been recommended for children.34 Conventionally DEXA scans yield areal values in g/cm2, but computation of volumetric density (bone mineral apparent density, BMAD) can be accomplished.27
The use of pQCT in children and adolescents has been assessed by the International Society for Clinical Densitometry.35 This technique not only provides direct measurement of volumetric bone density but also does so for the separate cortical and trabecular compartments (figure 1).36 It is possible to also derive a measure of bone strength in the form of SSI. We are performing pQCT at the 4% and 20% sites of the non-dominant radius and at the 4%, 20% and 66% sites of the ipsilateral tibia. The distal sites provide measures of trabecular and the proximal sites of cortical bone. These measurements are accomplished in 10 min with a Stratec XCT 2000L instrument (Stratec Medizintechnik, Pforzheim, Germany), and expose the participants to approximately 5 μSv of radiation, equivalent to 2 days of natural radiation exposure.37
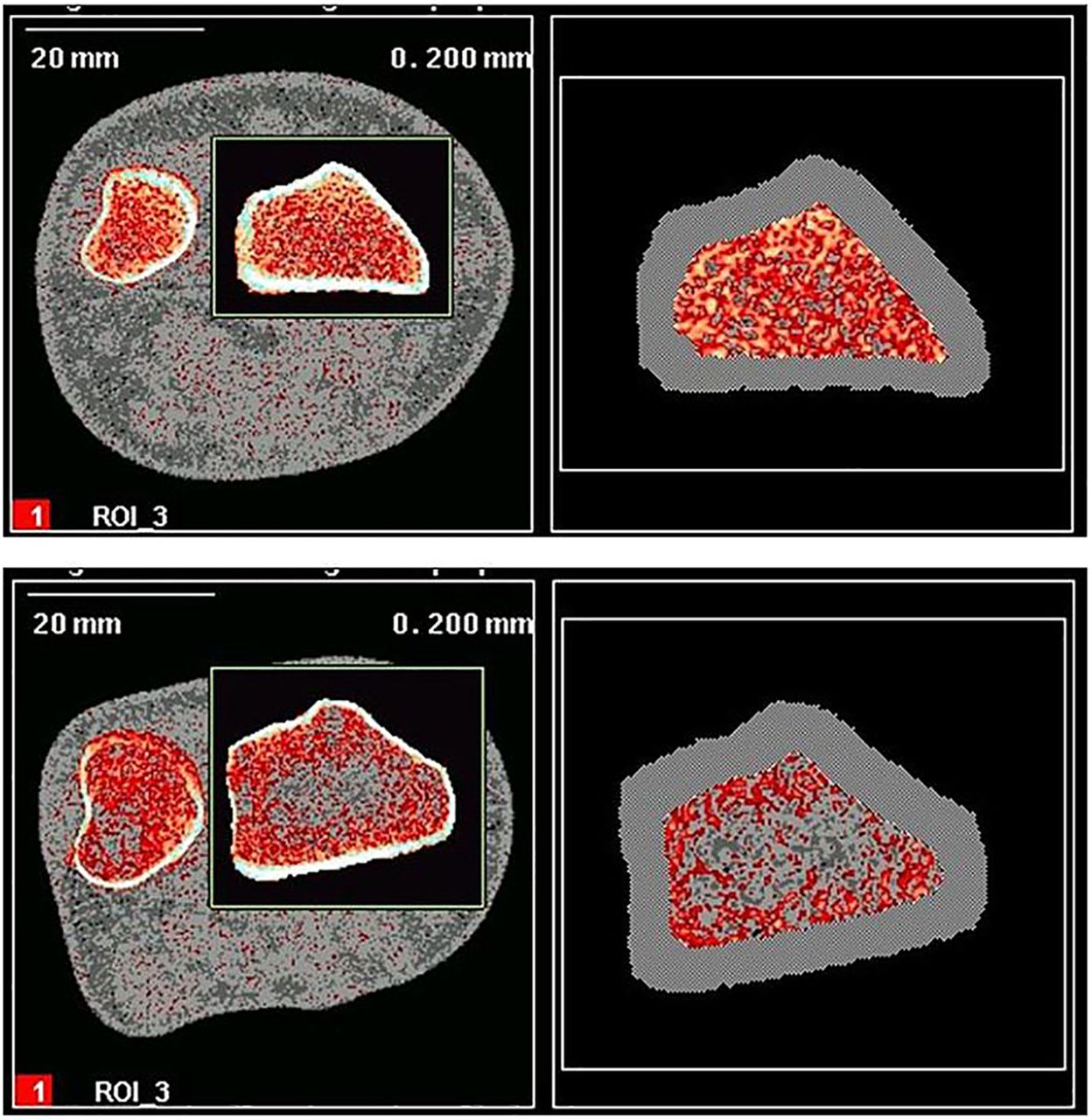
The upper image corresponds to the peripheral quantitative CT scans acquired at the distal 4% and 20% radius for a 20-year-old woman. The trabecular density, at the former site, is 236.5 mg/cm3 while the cortical density, at the latter site, is 1208.8 mg/cm3. The lower image corresponds to the scans acquired for a 35-year-old woman with trabecular density of 115.5 mg/cm3 and cortical density of 1283.5 mg/cm3.
Additionally, we are providing the pQCT scans to a local colleague for detailed measurements of trabecular architecture using software that he has developed for that purpose.38 This allows for the measurement of ‘network connectivity’ as well as average and maximal ‘hole sizes’ that are better predictors of fracture than BMD.39 Furthermore, we are measuring muscle density in the calf to complement the measurement of SMM by DEXA. LBM in children who are 4-year survivors of ALL exhibits greater hydration and lower density than in healthy controls.40 pQCT allows determination of muscle adiposity, fat within and between muscle cells.
Such detailed assessments of bone geometry and architecture will be useful in determining the long-term effects of bisphosphonates in children, for 20 of the participants in this study received one of these agents to reverse progressive demineralisation of bone,41 as exemplified in figure 2. Alendronate demonstrates short-term safety and efficacy in children,42 but the long-term effects are unknown and bisphosphonates are incorporated into the skeleton as structural analogues of bone pyrophosphate.8

{kind=link}
{kind=link}
Lumbar spine bone mineral density (BMD) Z scores in an adolescent male during (2+ years) and after the treatment for acute lymphoblastic leukaemia.
Other measures
Physical activity is being estimated by the validated HAES, developed in Hamilton,43 that is self-completed by the study subjects. The scale has been used previously in survivors of ALL in childhood and adolescence,44 and is based on the duration and intensity of physical activity with the latter categorised as inactive (eg, lying down), somewhat inactive (eg, sitting), somewhat active (eg, walking) and very active (eg, running).
HRQL is being assessed with one of the HUI family of instruments developed at McMaster University. These are preference-based measures that provide utility scores for single attributes (domains or dimensions) of health and multiattribute HRQL.45 For single attribute scores the range 0.0–1.0 represents the span of greatest to no morbidity. For multiattribute HRQL scores, the range 0.0–1.0 spans the equivalence of being dead to perfect health. Negative scores for HRQL represent states of health worse than being dead.46 HUI instruments have been used in a longitudinal study of HRQL in children and adolescents undergoing treatment of ALL with a DFCI protocol,47 as well as in a cost-utility analysis of the treatment of ALL in young people.48 We are using the HUI123S4.15Q instrument to allow self-report for the preceding period of 4 weeks. Like the HAES measure, this HUI questionnaire is suitable for self-assessment by participants ≥11 years of age.
Data acquisition, entry and management
Participants are assigned a unique subject identifier to facilitate data entry. Raw data are provided to two clinical research coordinators by the investigators responsible for the individual components of the study; they enter the data in a master Excel spreadsheet. The coordinators also abstract demographic, disease and clinical baseline data at diagnosis from the medical charts. Results of height, weight and BMI, and of arm anthropometry are entered in the master file, together with a history of fracture elicited from the participants and the use of bisphosphonates provided by the pharmacist.
DEXA scans provide fat mass and LBM as kg and Z scores, together with LS-BMD Z and T scores. pQCT gives trabecular and cortical bone volumetric densities (mg/cm3), cortical thickness (mm), trabecular texture and SSI (mm4). These are all submitted in Excel format and merged with the master database.
Data analysis
Patient demographics, body composition (BMI, TSFT, whole body fat mass, MUAC, LBM, SMM) and bone health (LS BMD Z and T scores, trabecular volumetric bone density and SSI) parameters, physical activity (HAES) and HRQL will be summarised using descriptive measures expressed as mean (SD) or median (minimum, maximum) for continuous variables and number (percent) for categorical variables. Association between categorical outcomes and groups will be assessed using Fisher's exact t test or χ2 test. Pearson correlation coefficient will be used to test correlations between different variables such as BMI and fat mass, TSFT and fat mass, MUAC and LBM, and MUAC and SMM. By focusing on bone health the following associations will be explored: LS-BMD with trabecular volumetric BMD, cortical thickness with SSI, cortical thickness with fracture (a binary variable), SSI with fracture. Univariate and multivariate regression analyses will be used to study the impact of bone health and body composition on HAES and HAES with overall HRQL. The limit for statistical significance will be set at α=0.05. In all comparisons, 95% CIs of the measure of association between groups will be reported. Table 1 outlines the plan for statistical analyses.
List of analyses
Ethics and dissemination
In addition to the conventional strategy of disseminating the results of this study by presentations at national and international meetings, and publications in peer-reviewed journals (a total of nine manuscripts is anticipated at present), the authors intend to place summaries in the websites of organisations that are accessed by adolescent and young adult survivors of cancer. These include
In Canada: cancerview.ca
In the USA: criticalmass.org/about us
In Australia: canteen.org.au
In the UK: tyac.org.uk/about-us
The participants in this study will receive a summary of the results individually as a hard copy by mail.
Discussion
Among the novel components of this study are correlation of SMM with physical activity in survivors of ALL; assessment of muscle composition by pQCT in such a population; detailed analysis of the structure of trabecular bone by unique purpose-designed software; and determination of the long-term effects of bisphosphonates on bone integrity in children.
The anticipated findings of excessive fat mass and low SMM will provide a stimulus to customised programmes of physical activity that will increase time spent in exercise and improve HRQL while reducing the risk of metabolic syndrome, and associated morbidities and premature mortality.49 ,50
Detection of defective bone integrity, associated with inadequate mineralisation and abnormal architecture, will prompt the exploration of a role for bisphosphonates to enhance bone health and thereby minimise the risk of osteoporosis and debilitating/life-limiting fractures.51
The main limitation of this study is the size of the sample, though this is bigger than those reported by others 52 ,32 using DEXA in long-term survivors of ALL. Again, the composition of the sample may not be generalisable to other populations. While this may be unimportant with respect to obesity, it is unknown with reference to other outcome measures.
It can be estimated that there are hundreds of thousands of survivors of ALL in childhood and adolescence globally. The majority are young people who are at risk of well-defined long -term sequelae of therapy that impose burdens of ill-health and limit life expectancy. Among the sequelae that are most amenable to amelioration are perturbations of body composition and bone health.
The findings of this study will shed light on these adverse ‘late effects’ and offer avenues for therapeutic modification with the prospect of enhancing HRQL and improving the life expectancy of this considerable population. In addition, this study will provide valuable information regarding correlations of various parameters measured using different techniques, allowing for the selection of techniques that are suitable for future studies.
References
Footnotes
Contributors Dr Colin Webber played a leading role in the study concept, design and implementation. He died in September 2012. RB is the Principal Investigator on the study, responsible for its overall conduct. TN is responsible for assembly of the data base together with data capture and management. CG is responsible for the analysis and interpretation of pQCT data. CM has responsibility for the detailed results of DEXA. UA has responsibility for the overall analytical methods.
Funding This study is supported by an award (NIF 11290) to TN from the New Investigator Fund of Hamilton Health Sciences.
Competing interests None.
Ethics approval This study has continuing approval from the Hamilton Integrated Research Ethics Board (REB Project # 10-508-S) that represents Hamilton Health Sciences, McMaster University and St. Josephs Healthcare.
Provenance and peer review Not commissioned; externally peer reviewed.