Article Text

Abstract
Objectives To systematically investigate the prevalence of pain, factors related with pain and pain management interventions in patients with chronic obstructive pulmonary disease (COPD).
Design Systematic review and meta-analysis.
Data sources and study eligibility criteria PubMed (MEDLINE), EMBASE, CINAHL and PsychINFO from 1966 to December 2013. Studies were included if they presented clinical data on pain or symptom burden in patients with COPD, or pain as a domain of quality of life (QoL). All types of study designs were included.
Results Of the 1571 articles that were identified, 39 met the inclusion criteria and were included in this review. Fourteen studies focused on pain and symptom burden (including pain) in patients with COPD and 25 studies focused on QoL using a questionnaire that included a separate pain domain. Reported pain prevalence in high-quality studies ranged from 32 to 60%. Included studies report that pain is more prevalent in patients with COPD compared to participants from the general population. Comorbidity, nutritional status, QoL and several symptoms were related to pain. None of the included studies reported a significant relationship between lung function and pain prevalence or severity. However, studies investigating pain in patients with moderate COPD reported higher pain prevalence compared to studies in patients with severe of very severe COPD.
Conclusions Although literature on this topic is limited and shows substantial heterogeneity, pain seems to be a significant problem in patients with COPD and is related to several other symptoms, comorbidity and QoL. Data synthesis suggests that pain is more prevalent in patients with moderate COPD compared to patients with severe or very severe COPD. Further research is needed and should focus on determining a more accurate pain prevalence, investigating the relationship between pain prevalence, disease severity and comorbidity and explore implementation and efficacy of pain management interventions in patients with COPD.
- PAIN MANAGEMENT
- PRIMARY CARE
- RESPIRATORY MEDICINE (see Thoracic Medicine)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first systematic review on pain in patients with chronic obstructive pulmonary disease (COPD).
A broad search strategy was used, to minimise the risk of missing any relevant published studies.
Literature on pain in patients with COPD is limited and included studies that showed great heterogeneity, therefore confounding and selection bias are likely to occur.
Owing to the search strategy that was used, data on pain as a subdomain of quality of life may not be complete.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic, usually progressive airway disease. Both the prevalence and disease severity of COPD are strongly related to age and worldwide, the rate of related morbidity and mortality is rising.1 COPD represents a major burden for individual patients, healthcare systems and society in terms of healthcare costs.2 As the disease progresses, health status becomes increasingly impaired. Especially in advanced COPD, patients suffer from high symptom burden, impaired functional capacity and poor quality of life (QoL).3 ,4
Well-known symptoms in COPD are dyspnoea, cough and wheezing, whereas other symptoms such as fatigue, nausea and insomnia are also frequently reported.5 Recent literature indicates that pain is also a significant symptom in patients with COPD. Two systematic reviews on patients with end-stage COPD6 ,7 reported prevalences of pain of 21–77%. Both these reviews reported only on studies including patients with advanced or terminal disease or studies on palliative care in patients with very severe COPD. Less is known about pain in patients with mild-to-moderate disease. In a cross-sectional study on pain in patients with moderate-to-severe COPD, HajGhanbari et al8 reported that pain is more prevalent among individuals with COPD compared with healthy adults. Bentsen et al9 found similar results, reporting pain in 45% of the patients with moderate COPD compared with 34% in the general population. Other questions remain about pain in COPD. For example, the relationship with disease severity and comorbidity remains unclear8 and information on the causes and characteristics of pain, and how pain influences functional capacity and QoL, is scarce.8 ,9 There are several factors related to COPD that may contribute to a higher pain prevalence in patients with COPD. The systemic inflammatory process, which activates cytokines, may generate chronic and neuropathic pain. Musculoskeletal disorders and comorbidities (including mechanical limitations of chest wall movement due to hyperinflation and osteoporosis) are also considered possible causes of pain in patients with COPD and inactivity may aggravate common age-related comorbidities such as osteoarthritis and low back pain.8 Improving knowledge on aetiology, characteristics, correlations and impact of pain is important and necessary to improve pain recognition and pain treatment in patients with COPD. It is likely that adequate pain recognition and treatment is important in improving QoL, exercise tolerance and lifelong adherence to physical activity in patients with COPD. Thus, pain seems to be a relevant but poorly understood problem in patients with COPD. Therefore, the aim of this review is to systematically describe and investigate pain in patients with COPD. More specifically, to examine the prevalence of pain and factors related with pain and to identify interventions that may reduce pain in patients with COPD.
Methods
Electronic searches
We conducted a systematic search using MEDLINE/PubMed (from 1966 to December 2013), EMBASE (from 1980 to December 2013), CINAHL (from 1981 to December 2013) and PsychINFO (from 1980 to December 2013) using the following groups of keywords:
Pain, pains, Pain Measurement, Analgesics, analgesic (PubMed), pain, pain assessment, analgesia, analgesic (EMBASE), Pain, analgesia, analgesic (CINAHL), Pain, Aphagia, Back Pain, Chronic Pain, Headache, Myofascial Pain, Neuralgia, Neuropathic Pain, Somatoform Pain Disorder, Analgesia, analgesic (PsychINFO).
Pulmonary Disease, Chronic Obstructive, COPD, Lung Diseases, Obstructive, chronic bronchitis, chronic obstructive airway disease, chronic airway obstruction, chronic airway obstructions, COAD, chronic airflow obstruction, chronic airflow obstructions, Pulmonary Emphysema.
Keywords were entered using controlled terms (eg, Medical Subject Headings in Medline) and as free-text word. Within each group the keywords were combined using ‘OR’ and the two groups were combined using ‘AND’ (see online supplementary file 1). No language or other restrictions were applied. Reference lists from included studies and reviews were searched by hand to identify additional articles. All articles that were identified by the electronic search were put into a reference database (Reference Manager V.12.0).
Selection of studies
Articles that reported original data on pain in patients with COPD, or assessed pain as a domain of QoL in patients with COPD, were considered eligible. We included all types of study designs (cross-sectional, longitudinal, prospective/retrospective, qualitative/quantitative design). Articles without an (English) abstract, reviews, editorials, conference abstracts and case reports were excluded. Two members of the review team (EFvDvI and KG) independently assessed the titles and abstracts of all potentially relevant publications that were identified from the search. Decisions of the two reviewers about inclusion/exclusion were compared and, in case of disagreement, were resolved by asking a third reviewer (DJAJ) and to achieve consensus. Subsequently, the same two reviewers evaluated the full text of all potentially eligible articles. Decisions about inclusion and exclusion were again compared and, in case of disagreement, resolved by asking the third reviewer in order to achieve consensus.
Data extraction and quality assessment
Details on study design, patients, setting and outcome were recorded by two independent reviewers (EFvDvI and KG). For each study the following items were recorded: author, journal, year of publication, country of origin, design and aim of the study, setting, inclusion and exclusion criteria, response rate, number of patients, patient characteristics (age, forced expiratory volume in 1 s as % of predicted value (FEV1% predicted), Global Initiative for Chronic Obstructive Lung Disease (GOLD) grade, and gender), pain and QoL instrument used, reported pain prevalence or mean score on the pain domain of the QoL instrument, correlations, limitations and conclusions.
All included articles were ranked for quality according to the Mixed Method Appraisal Tool (MMAT).10 The MMAT has recently been developed for the appraisal stage of systematic literature reviews that include quantitative, qualitative and mixed methods studies. The MMAT has proven to be an effective and practical quality assessment tool for mixed method review studies.10 The MMAT consists of four criteria for the appraisal of quantitative (descriptive, randomised and non-randomised) and qualitative studies. Hence, each study design is judged within its methodological domain (table 1). The MMAT scores range from 100% (all four criteria are met) to 25% (one criterion is met). In the present review, quality assessment scores were calculated for all included studies. Ranking according to the MMAT was conducted by two independent reviewers (EFvDvI and KG) and any disagreement in the MMAT scores was resolved by discussion or by asking a third reviewer (DJAJ) for advice to reach consensus.
Criteria Mixed Methods Appraisal Tool (MMAT), by Pluye et al10
Data synthesis and meta-analysis
A meta-analysis was performed concerning the Short-Form health survey (SF)-36_Bodily Pain data.
The SF-36 is a widely used, self-administered, reliable and valid instrument to assess generic health-related QoL.11 The SF-36 consists of 36 items divided into eight subdomains. The score of each subdomain ranges from 0 to 100, with 100 representing the best quality of life. The questionnaire contains two questions related to pain: the SF-36 bodily pain subdomain (SF-36_BP): ‘How much bodily pain have you had during the past (4) week(s)?’ (score from 0 (no pain) to 6 (very severe pain)) and ‘During the past (4) week(s), how much did pain interfere with your normal work (including both work outside the home and housework)? (score from 0 (not at all) to 5 (extremely)) We performed a meta-analysis with a Forest plot using a Microsoft Excel spreadsheets, as developed by Neyeloff et al.12 They showed that this method produces a statistically adequate but graphically appealing forest plot summarising descriptive data. We assumed a random-effects model to calculate the mean score on the SF-36_BP item and a 95% CI. The heterogeneity was assessed with the Q statistic and the I2 index. Meta-analyses and Forest plots using a Microsoft excel spreadsheet were conducted by step-by-step guide focusing on descriptive data analysis.12 To determine the strength of the linear correlations between lung function (FEV1% predicted) and pain prevalence and the SF-36_BP score, we calculated the correlation coefficient between these variables. In case of normally distributed data, Pearson correlation coefficient was calculated. In case of non-normally distributed data a non-parametric test (Spearman's test) was used. We defined statistical significance at p≤0.05 (two-sided level of significance). In studies that presented only the GOLD grade distribution the mean GOLD grade was calculated and converted into a mean FEV1%-predicted.
Results
Study selection and characteristics
The electronic systematic search identified 1571 eligible citations (PubMed 1067, EMBASE 379, CINAHL 71, PsychINFO 54). Eight studies were identified using other sources. A total of 1491 citations were excluded based on title and abstract. In total, 88 articles were reviewed in detail. Reasons for exclusion are reported in the PRISMA flowchart (figure 1). Thirty-nine studies met the inclusion criteria and were included in the review (tables 2 and 3).
Pain and symptom burden
Pain as a subdomain of quality of life (QoL)

Flow diagram of the inclusion of studies (according to the PRISMA guidelines).
Fourteen studies focused on pain and symptom burden (including pain) in COPD5 ,8 ,9 ,13–23 and 25 studies focused on QoL using a questionnaire that included a separate pain domain4 ,24–47 (table 2 and 3). The included studies were published between 1995 and 2013. All included studies on symptom burden in COPD were published in the past decade (2000–2013) and studies with a specific focus on pain in COPD were published in the last 5 years (figure 2).

Number of publications on ‘pain’ and ‘symptom burden including pain’ in patients with chronic obstructive pulmonary disease.
Of the 14 articles on pain and symptom burden in COPD, three reports from Bentsen et al9 ,21 ,22 and two reports from Borge et al18 ,20 were based on the same original research study. Ten studies were conducted at the outpatient pulmonary department of a hospital (secondary and tertiary care), one in primary care and three were population-based studies. Most studies on pain and symptom burden (n=10; 71%) had a cross-sectional design. The majority of the included studies on pain as a domain of QoL also used a cross-sectional design (n=17; 68%), seven studies used a prospective design (observational (n=3) and interventional (n=4)) and one study used a retrospective design. Almost all studies (n=21) on pain as a domain of QoL included patients with COPD recruited from an outpatient pulmonary department or hospital/intensive care unit setting (secondary and tertiary care).
Quality assessment
Of the 14 studies on pain and symptom burden in COPD, 10 had a MMAT score of 100%, three scored 75% and one study scored 50% (table 2). Shortcomings in quality included insufficient response rate,13 ,14 ,18 ,20 or insufficient comparability between participants.13 Of the 25 studies on pain as a subdomain of QoL, 20 had a score of 75% (n=14) or 100% (n=6). The most frequent shortcoming in quality assessment was an insufficiently or not reported response rate (n=19; table 3).
Pain measurement
Pain was measured using different instruments. Five studies on pain and symptom burden in COPD used the Brief Pain Inventory (BPI), or the body outline diagram of the BPI.48 The BPI is a self-administered questionnaire used to assess the severity of pain (scale 0–10; cut-off points: mild pain (0–4), moderate pain: (5–6) and severe pain (7–10)) and the impact of pain on daily functioning (scale 0–10) in patients with chronic diseases or conditions. The BPI also contains a body diagram on which patients can indicate the location on which they experienced the most pain.20 ,48 In five studies pain was not measured with a specific pain or symptom questionnaire, but a screening question was used, such as: ‘Are you generally bothered with pain?’9 or ‘Are you usually free of pain and discomfort?’.15 Other instruments used include: the McGill Pain Questionnaire (MPQ), the Memorial Symptom Assessment Scale (MSAS), the VOICES questionnaire and the London and Leeds Pain Survey. One study measured pain using a Visual Analogue Scale (VAS).5
Pain as a subdomain of QoL was measured using five different instruments: the SF-36 (n=19), the EuroQol-5 Dimensions (EQ-5D; n=3), the Nottingham Health Profile (NHP; n=3), the Health Status Questionnaire (HSQ; n=1) and the Duke Health Profile (DHP; n=1).
Prevalence of pain
Of the 14 studies on pain and symptom burden, 11 reported the prevalence of pain: range from 21% to 72.1% (figure 3). Studies on prevalence of pain differed in design, setting and patient characteristics. Mean age was 57.9–76.8 years and mean FEV1% predicted ranged from 21% to 48%. Three studies did not report the mean FEV1% predicted or the GOLD grade of the included patients. The MMAT scores of the studies that reported pain prevalence ranged from 50% to 100%. The reported pain prevalence of the studies with a MMAT score of 100% ranged from 32.4% to 59.8% (figure 3). Five studies investigated the prevalence of pain in patients with COPD compared to participants from the general population,8 ,9 patients with other chronic diseases5 ,23 or patients with lung cancer.13Bentsen et al9 found a pain prevalence in patients with COPD of 45% compared to 34% in the general population (p=0.02) and HajGhanbari et al8 reported that patients with COPD reported 2.5 times more pain and 3.7 times more interference of pain with daily activities, compared to healthy people. Roberts et al also reported that a higher pain prevalence in patients with COPD compared to patients with other chronic diseases (59.8% vs 51.7%; p=0.001), but in the study conducted by Janssen et al, patients with chronic heart failure reported more pain than patients with COPD (48.8% vs 32.4%, p=0.05).

Prevalence of pain. prospective cohort study; ♦ cross-sectional study; ▪ mixed method; ▴ retrospective postbereavement study. green: Mixed Method Appraisal Tool (MMAT)-score: 100%; orange: MMAT-score: 75%; red: MMAT-score: 50%.
Of all included studies, 19 used the SF-36, the SF-20 or the SF-8. Of these, 17 reported scores on the bodily pain domain as a mean score (SD). In four of these studies, the SF-36_BP was measured in two separate groups of patients with COPD (cases and controls). A random-effects meta-analysis on the SF-36/20/8_BP data of the 21 studies and groups of patients with COPD, showed a mean score on the SF-36_BP of 66.7 (CI 95% 61.2; 72.2; figure 4). The three studies that used the EQ-5D showed that 45%,40 46%4 and 56%41 of the patients with COPD reported having any problems on the subdomain pain/discomfort of the EQ-5D, respectively.

Random effects meta-analysis of studies that examined the mean score on Short-Form health survey-36 (SF-36_BP) in patients with chronic obstructive pulmonary disease. The Forest plot shows the mean scores with 95% CIs for included study populations. The Q statistic was 19.32 with df=20 (p>0.10) and I2 was 0%. The MMAT scores are shown using different colours: green: MMAT-score: 100%; orange: MMAT-score: 75%; red: MMAT-score: 50%; purple: MMAT-score: 25%.
Characteristics of pain
Five studies measured pain intensity and interference using the BPI. Mean pain intensity scores ranged from 2.8 to 5.4 points (mild to moderate pain) and mean interference scores ranged from 3.6 to 5.8 points (mild to moderate interference) on a scale from 0 to 10 (higher scores indicating more pain intensity/interference). Three studies used the body outline diagram of the BPI to investigate the most prominent locations of the experienced pain.9 ,17 ,20 Most frequently reported locations of pain were the shoulders and neck: 33% (n=15),9 36.4% (n=56)20 and 50% (n=8)17; lumbar region: 29.2%(n=45)20 and 47% (n=21)9 and chest: 17.5% (n=27),20 36% (n=16)9 and 38% (n=6).17 None of the included studies investigated the type of pain (eg, neuropathic or nociceptive pain) or conducted a comprehensive pain assessment.
Factors related to pain
Of the 14 studies on pain or symptom burden, seven reported factors related to pain or correlations between pain and several variables, such as lung function, comorbidity and other symptoms (table 4).
Factors related to pain (presence and severity)
Four of these studies reported from the same two original studies.18 ,20–22 None of the studies on pain or symptom burden reported a significant relationship between lung function (FEV1% predicted, GOLD grade) and pain prevalence or pain severity. Several studies reported a significant correlation between pain and comorbidity.8 ,21 ,23 Bentsen et al21 reported that comorbidity was a risk factor for pain in patients with COPD; patients with COPD and pain were more likely to report the presence of a comorbidity and had a significantly higher number of comorbidities. However, the study from Borge et al20 found no significant difference in the number of comorbidities between patients with COPD with and without pain. These conflicting results are also found for the correlation between pain severity and the number of comorbidities8 ,18 (table 4). Other variables that showed a significant correlation with pain presence or pain severity are: QoL, breathlessness, insomnia, fatigue, anxiety, depression and nutritional status (table 4). Of the included studies on pain as a subdomain of QoL, none reported correlations between the SF-36_BP score and variables of interest. Two studies using other QoL instruments, that is, the EQ-5D40 and the NHP27 concluded that their analysis showed no significant correlation between pain as a subdomain of QoL and lung function.
Pain management interventions
None of the included studies aimed to investigate the effect of a specific intervention on pain in patients with COPD. Bentsen et al9 reported that 49% of the participants with pain received treatment with analgesics and 16% received physiotherapy. In a cross-sectional study in patients with advanced COPD, Janssen et al5 found that 47% of the patients with pain (VAS score >30 mm) reported that their symptoms were addressed. Furthermore, if symptoms were treated, patients reported only moderate satisfaction with symptom treatment. One study on symptom burden in patients with severe COPD in primary care reported that all patients who suffered from pain ever day or pain on most days, were on prescribed analgesics.19 Three studies investigated the effect of a pulmonary rehabilitation programme on health status.32–34 All reported no effect of the intervention on the pain domain of the health status instrument used (two studies used the SF-36, one used the HSQ).
Overall relationship between pain prevalence and disease severity
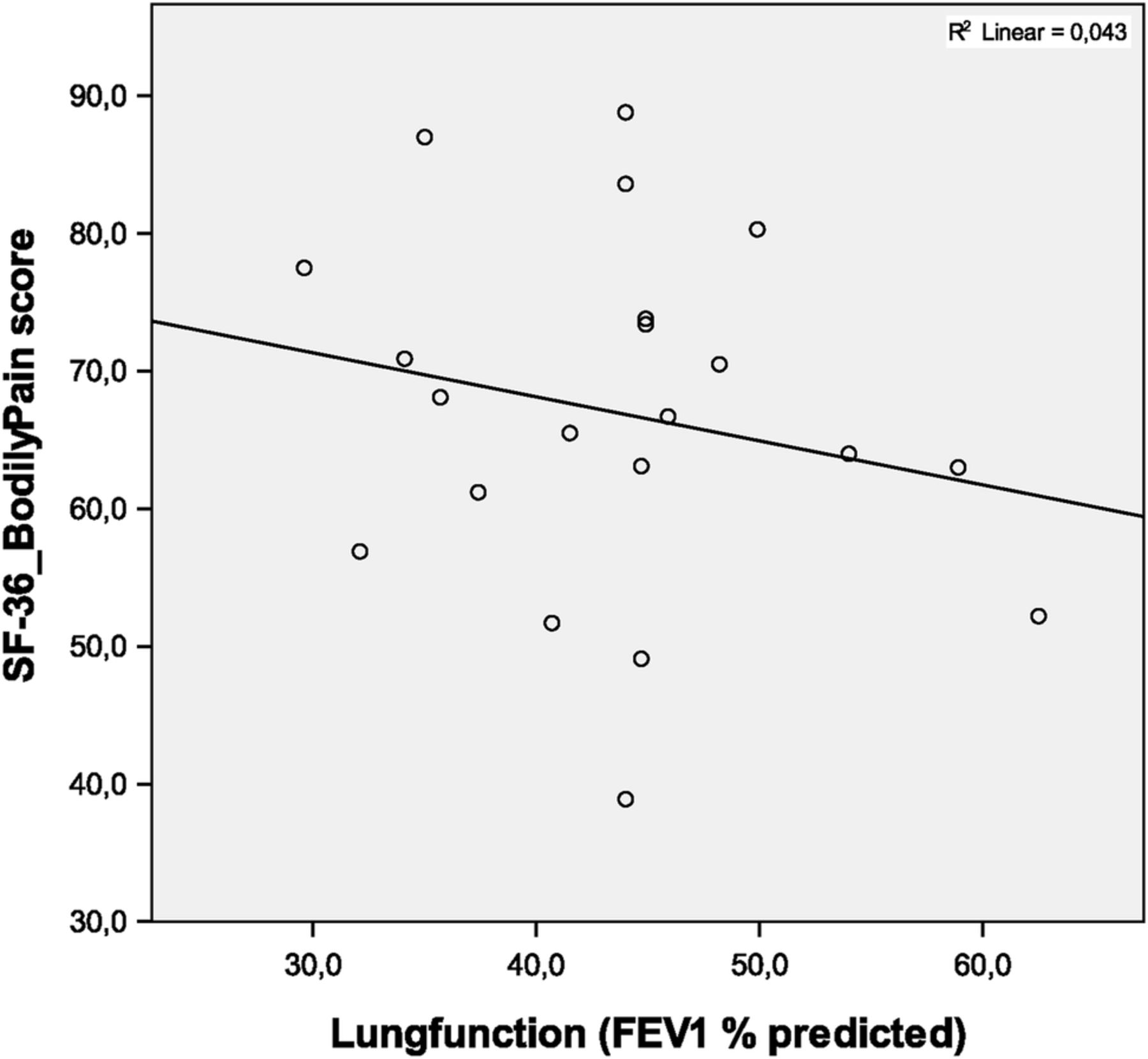
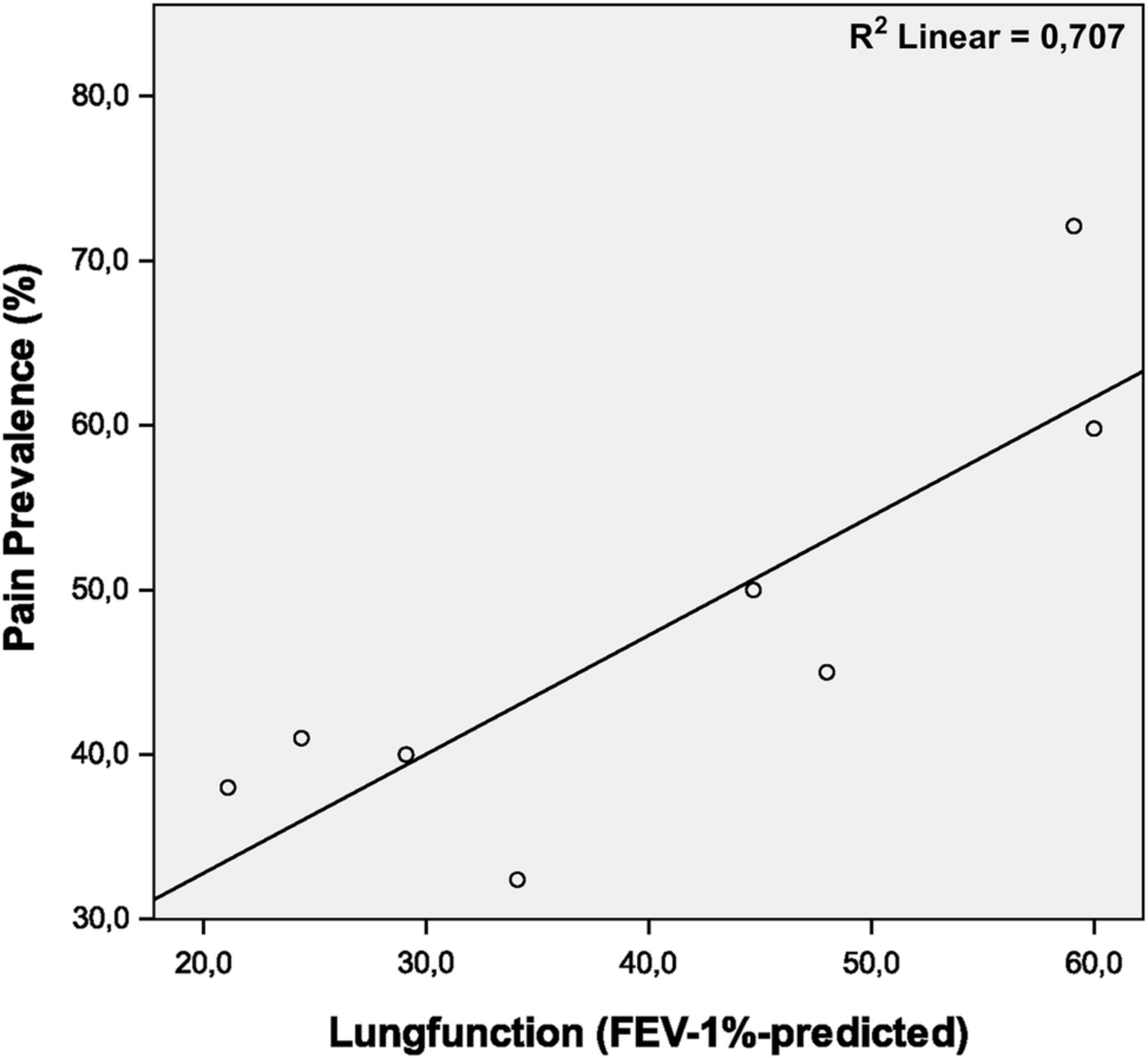
To determine the relationship between lung function and pain prevalence, we calculated the correlation coefficient between these variables. Of the 11 studies that reported on pain prevalence, seven also reported the mean FEV1% predicted and one study reported the GOLD grade distribution,23 which was converted to a weighted mean GOLD grade (figure 5). There was a strong correlation between lung function (FEV1% predicted) and pain prevalence; Spearmans r=0.79 (p=0.021). Of the 21 studies and groups that reported SF-36/20/8 scores on the pain domain, 18 reported the mean FEV1% predicted. In three groups of patients only the GOLD grade was reported,34 ,37 which was converted to a weighted mean GOLD grade. No significant correlation was found between the SF-36_BP score and lung function: Pearson's correlation coefficient=0.21 (p=0.37; figure 6).

Relationship between lungfunction and pain prevalence. Each data point represents a separate study. Correlation coefficient: Spearmans r=0.79 (p=0.021).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between lungfunction and Short-Form health survey-36 Bodily Pain (SF-36_BP) score. Each data point represents a separate study. Increasing units on the y-axis (eg, higher SF-36_BP scores) refer to less severe pain and better quality of life. Pearson's correlation coefficient=0.21 (p=0.37).
Discussion
Main findings
The first main finding of this systematic review is that pain seems to be a significant clinical problem in patients with COPD, with a reported prevalence in high-quality studies ranging from 32% to 60%. Second, literature on pain in patients with is limited; only a few studies with a specific focus on pain in patients with COPD have recently been published. Still, little is known about the causes and characteristics of pain, factors that are related to pain and literature on the effect of interventions aimed at reducing pain in patients with COPD is lacking. Third, our data synthesis shows that studies investigating pain in patients with moderate airflow limitation reported a higher pain prevalence compared with studies in patients with severe airflow limitation. This finding could suggest that pain is more prevalent in patients with moderate COPD compared to patients with severe or very severe COPD. However, confounding and selection bias are likely to occur and much remains unclear about the relation between pain and disease severity. Fourth, our results suggest a correlation between pain and several other symptoms, such as dyspnoea, insomnia, fatigue, anxiety and depression, QoL and comorbidity.
Strengths and limitations
To our knowledge, this is the first systematic review study on pain in patients with COPD. One strength of this study is that we included all types of studies and used a broad search method. Therefore, it seems unlikely that the search strategy we used failed to identify relevant published studies. Second, the selection strategy was objective, as it was performed by two, and in case of disagreement, by three individual members of the review team. Third, we were able to conduct a meta-analysis on the SF-36_BP data.
Some limitations also need to be discussed. First, as literature on this topic is scarce, only 14 studies on pain and symptom burden in patients with COPD were included. Moreover, these studies showed substantial heterogeneity in design, setting, patient characteristics and pain measurement instruments used. Selected studies included patients with relatively severe COPD; mean FEV1% predicted ranged from 21% to 48%. These differences in study methods might have influenced the reported pain prevalence and also limit the generalisability of the results. Furthermore, there were differences between the studies in patient selection criteria and the healthcare setting from which the patients were recruited, although most of the studies were conducted in a secondary (outpatient) care setting. Second, the appropriateness of including the SF-36_BP scores in this review is debatable. As our search strategy did not include ‘QoL’ as a keyword, we included only those studies on QoL that mentioned the keyword ‘pain’ in the abstract. This implies that our data on pain as a subdomain of QoL may not be complete. Nevertheless, we feel that the reported results do provide important information on this subject.
Interpretation of findings and relation to other literature
The wide range in pain prevalence can be explained by the heterogeneity in study design, setting, patient characteristics and instruments and definitions used to measure pain. We were interested in chronic and/or recurrent pain in patients with COPD. However, as we wanted a broad search method, we used ‘pain’ instead of ‘chronic pain’ as a major key word in our search strategy, as many studies do not clearly define pain as being ‘chronic’ or ‘acute’. We did however exclude studies that concerned ‘pain during acute bronchitis’ (figure 1). Different studies used different definitions of pain and none of the included studies presented longitudinal data on the course of pain. The wide range in pain prevalence can also be explained by differences in the quality assessment score. Three of the studies on pain and symptom burden that reported the prevalence of pain, had quality limitations as identified with the MMAT. Furthermore, in the study conducted by Elkington et al14 pain prevalence was based on reports of informants of the deceased participants. Agreement between the patient's and the proxy perception of pain is only moderate.14 ,49 This by-proxy reporting of symptoms and the fact that the study included only patients in the terminal phase of their disease, could explain the relatively high level of reported prevalence of pain (72%). Claessens et al13 reported a relatively low prevalence of pain (21%). However, pain was defined as ‘moderately severe or extremely severe pain at least half of the time’. Borge et al20 found a relatively high prevalence (72%) but used a much lower threshold, as pain was considered to be present in all patients that shaded pain on the body diagram of the BPI. Roberts et al23 also reported a relatively high pain prevalence of 60%. In their cross-sectional study, recurrent pain-related healthcare utilisation (diagnosis and treatment) was considered evidence of chronic pain; data were received from the managed care claims database and from the outpatient pharmacy. Although evidence of chronic pain based on diagnosis and management can be reliable, it should be noted that, in the latter study, 28.6% patients with COPD used short-acting or long-acting opioids, compared with 17% in the control group (patients with other chronic diseases).23 However, as the reason for prescribing opioids was not stated it is debatable whether opioid prescription was indeed aimed at treating pain, especially as it is also prescribed for chronic dyspnoea in patients with COPD.50 Therefore, the reported prevalence of chronic pain in the study of Roberts et al23 might be an overestimation. The reported prevalence of pain should be interpreted in relation to pain prevalence in the general population, as well as in patients with cancer and other chronic diseases. Recent population-based surveys showed that 25–35% of the adults report chronic pain.51 In patients with cancer this percentage is higher, as 50% of all patients with cancer experience chronic pain.51 Thus, the literature indicates that the prevalence of pain in patients with COPD is higher compared with the general population. Results from our meta-analysis on the SF-36_BP data also show that patients with COPD experience more pain compared to the general population: mean score of the SF-36_BP domain in the general US adult population is 75.2 (SD 23.7),11 which is higher than the mean score we found in our random-effects meta-analysis of the SF-36_BP data in patients with COPD. A higher score on the SF-36_BP domain refers to less pain and better QoL. We were not able to perform a meta-analysis on the results of the included studies that used other QoL instruments, because of the very small numbers of studies that used the same instrument (EQ-5D: n=3; NHP: n=2; HSQ: n=1; DHP: n=1). Results from the random-effects meta-analysis of the SF-36_BP scores show substantial heterogeneity. It is very likely, that parts of the heterogeneity is explained by research setting, population, study design, cultural diversity and other, unknown variables.
None of the included studies on pain or symptom burden reported a significant relationship between lung function (measured as FEV1% predicted or GOLD grade) and pain prevalence or pain severity. Interestingly, when we investigated the correlation between lung function and pain prevalence over all included studies on pain and symptom burden in patients with COPD, a strong correlation was found between lung function and pain prevalence. Studies that investigated prevalence of pain in patients with moderate COPD reported a higher pain prevalence compared with studies in patients with severe and very severe COPD. This might suggest that pain is more prevalent in patients with moderate COPD compared with patients with severe or very severe COPD. This finding has not previously been reported in literature on pain in patients with COPD. An explanation for this might be found in the hypothesis that when investigating the relationship between lung function and pain, confounding and selection bias are very likely to occur. Possible selection bias and confounding in the included studies might be an explanation for the observed relation between lung function and pain prevalence in the present study. For example, the number and severity of comorbidities may have caused selection bias: patients with very severe COPD and many comorbidities (cardiovascular and musculoskeletal such as osteoporosis) might have already died, or were not able to participate in the studies due to severely limited functional capacity. The number and severity of comorbidities might also have acted as a confounder in the relationship between pain prevalence and disease severity in the included studies. Furthermore, our results can be interpreted in line with a growing body of evidence showing that the correlation between FEV1, symptoms and impairment of a patient's health status is weak.52 Hence, in the recently updated GOLD Global Strategy for Diagnosis, Management and Prevention of COPD (GOLD strategy, 2014) the classification of a patient's disease severity requires assessment of symptoms and exacerbation history, in addition to the degree of airflow obstruction. Our results show some evidence for a relationship between pain and comorbidity, although the included studies are not entirely consistent on this topic. Musculoskeletal disorders and comorbidities (including mechanical limitations of chest wall movement due to hyperinflation and osteoporosis) are considered possible causes of pain in patients with COPD.8 ,9 However, due to the heterogeneity in the study designs we were unable to conduct a meta-analysis on pain prevalence and lung function controlling for comorbidity. In conclusion, much remains unclear about the relationship between disease severity, pain and comorbidity in patients with COPD and further research on this topic is needed.
We were unable to identify a study that investigated a specific intervention aimed at reducing pain in patients with COPD. The lack of literature on this topic is probably due to the fact that, in general, literature on pain in patients with COPD is scarce and pain seems to be a symptom that is often overlooked; this applies to daily practice and to research on the effect of comprehensive interventions, such as pulmonary rehabilitation (PR) and integrated disease management (IDM). In systematic reviews on PR and IDM in patients with COPD, pain is not mentioned as a patient-centred outcome in the field of symptom management.53 ,54 Also, in national and international COPD guidelines there is almost no discussion of pain as part of a comprehensive symptom assessment. For example, the GOLD Global Strategy for Diagnosis, Management, and Prevention of COPD (GOLD guideline 2014) does not mention chronic pain and discusses opioids only in the context of the relief of dyspnoea. Also, the combined statement on PR of two major international medical societies does not mention pain as a problem in COPD management.55 Moreover in the Institute for Clinical Systems Improvement (ISCI) guidelines for management of COPD, pain is not discussed. Only the American Thoracic Society (ATS) clinical policy statement on palliative care for patients with respiratory diseases and critical illness includes a separate section on pain management; however, this addresses only dying patients with respiratory diseases and critical illnesses in general.56
Conclusion and implications
Pain in patients with COPD is a significant problem with an estimated prevalence of 32–60%. Literature on this topic is scare, and studies specifically focusing on pain in patients with COPD have only recently been published. Little is known about the factors associated with pain and no literature is available on the effect of interventions aimed at reducing pain in patients with COPD. Studies that investigated pain in patients with moderate airflow limitation reported a higher pain prevalence compared with studies in patients with severe and very severe airflow limitation. This finding might suggest that pain is more prevalent in patients with moderate COPD compared with patients with severe or very severe COPD. However, there was a substantial heterogeneity in patient characteristics and outcome assessment tools. More research on this topic is needed. Standardisation of assessment tools of pain in patients with COPD is needed. Future studies should focus on determining a more accurate prevalence of pain in patients with COPD, also in relationship to disease severity and comorbidity. Research should also pay more attention to the causes, course and characteristics of pain and clinical intervention trials are warranted. Furthermore, adequate pain recognition and treatment in clinical practice is important and pain assessment should be incorporated into regular comprehensive symptom assessment in the clinical care of this group of patients. Finally, pain prevalence and its possible impact on QoL should be discussed in guidelines on COPD in order to raise awareness and recognition of this topic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors EFvDvI, KHG-S and DJAJ selected the studies. EFvDvI wrote the manuscript. KHG-S, MS-vE, MWMW, DJAJ, NHC and WPA reviewed and helped writing the manuscript. All authors contributed to the design of the study.
Funding EFvDvI is financially supported by Zorggroep Solis, Deventer, the Netherlands. Zorggroep Solis is the long-term care facility at which EFvDvI works as elderly care physician.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.